DOI: 10.31038/ASMHS.2021531
Abstract
The brain coordinates the reproduction and understanding of internal speech. The processes of thinking are given in the form of internal speech. The perception of internal speech involves the primary and secondary crust centers of analyzers, which record the corresponding waves, signals and rhythms and qualify them as language. This is achieved in two ways: either use functional neuroimaging and other additional research methods that allow localizing the structures currently functioning, or select patients with damage to certain areas and conduct a detailed neurocognitive study in comparison with healthy people from the control group, determining which functions in this lesion fall out. The principal issue of internal speech research is languages. A more complex question is the study of the connection of thinking, memory with internal speech. Now, especially when neurologists take into account the plasticity of the brain, functional relationships, general principles, pathways of excitation are of greater interest. Technologists of non-invasive neurointerfaces use methods and technologies to localize structures that control the understanding and reproduction of internal speech, the communication between them, the stages of speech signal processing and the role of each structure at these stages. The introduction to the study highlights approaches and methods for identifying various functional speech aspects. The mental lexicon section discloses the semantic component and the syntactic component, as well as the perceived and reproducible forms of words of internal speech. The section holographic human consciousness describes aspects of storing life information. The hologram of consciousness is the main form of storage of information about human life. In the section, holographic fixation of internal speech presents functional magnetic resonance tomography focused on BOLD effect detection, which is today the optimal tool for mapping neuronal activity, more precisely, the functional state of neural networks – the basis for visualizing our holographic images in real time. Using nanoresonators with Fourier transducers, the brain activity of a human internal speech holographic image can fix mental noninvasive neurointerface in language form by mental lexicon.
Keywords
Mental lexicon, Holographic consciousness, Neurointerface, Functional magnetic resonance tomography
Introduction
Internal speech is related to thinking: the modern position of cognitive science is such that without internal speech, thinking, primarily abstract-logical, is impossible [1]. If the studies are supplemented by functional neuroimaging, they are also of particular interest as a reflection of neuronal plasticity processes [2,3]. Electrophysiological studies use the method of induced potentials. The area in which the identified potential is generated can be determined based on its severity in different leads:
– The potential N400, negative, reaches the maximum amplitude 400 ms after the presentation of the corresponding stimulus, most pronounced in the centroparietal zone, reflects the processes of semantic analysis, that is, awareness of meaning.
– LAN potential (front left negative wave), resembling a N400 in delay, but most pronounced in leads from the left frontal departments, responds to the use of parts of speech that do not fit into the syntactic structure of this sentence (for example, “soft toy” instead of “soft toy”) [4];
The most famous electrostimulation studies belong to Canadian neurosurgeon Wilder Penfield. He described the results of his work in the monograph “Language and Brain Mechanisms,” still relevant for neurologists and cognitive specialists [5].
This can also include studies using deep brain stimulation [6] and transcranial magnetic stimulation, which began to be carried out relatively recently.
Functional neuroimaging methods are currently leading methods in the study of the neurophysiology of internal speech. Let us judge which structures are functioning at the moment:
– Functional magnetic resonance imaging (fMRI) and positron emission imaging of certain brain regions;
-diffuse-tensor MRI allows visualization of conducting brain pathways connecting these areas; magnetoencephalography (MEG) makes it possible to measure and graphically represent magnetic fields that are formed due to electrical activity of the brain.
The structure responsible for understanding speech is the Wernicke zone, the posterior part of the upper temporal gyrus. This area is adjacent to the auditory cortex, specialized in speech perception and contains sensory images of words and their combinations characteristic of the native language. The model also claims that sensory images do not carry semantic content – this aspect of speech cannot be specifically localized in the brain, but, nevertheless, in the process of signal processing, there should be an appeal to the “repository” of concepts – the semantic units of our speech. There are links between the Wernicke zones and the “repository” of concepts [7].
The “double flow” model was open to visual perception. After treatment in the visual cortex of the occipital lobe, the signal follows ventral and dorsal flows. Ventral goes to the temporal lobe and is necessary for identifying the object (answers the question “what?”), And dorsal goes to the parietal lobe and is designed to recognize the spatial characteristics of the object, its position and possible ways of interacting with it (answers the question “how?”)
Primary processing regarding the phonological composition and frequency-time characteristics occurs in the back of the upper temporal gyrus and the areas surrounding the upper temporal furrow, for the most part this is the Wernicke zone. The ventral flow is directed to the front and middle parts of the temporal lobe, it participates in the actual recognition and lexical analysis of speech (understanding its meaning, correlating with concepts stored in memory). Dorsal participates in sensorimotor integration, that is, correlation with motor images of words, and includes two separate paths: both pass through the temporal-parietal region, then the first is directed to the lower frontal gyrus, and the second to the prefrontal cortex. Presumably, one of them participates in the perception of internal speech, that is, controls the construction of segment sequences and provides more complex skills.
Hicoca-Popel claims that the perception of internal speech, through the functioning of the ventral flow, occurs bilaterally, and the intermediate center of dorsal flows working exclusively in the dominant hemisphere is placed in the temporal-parietal zone along the sylvium groove, at the junction of the temporal platform and operculum parietale [8].
In ventral flow, which is mainly involved in semantic and syntactic processing, excitation also moves along several paths. The lower frontal-occipital tuft connects the lower frontal cortex and dorsolateral frontal cortex with the posterior part of the temporal and parietal lobe. It passes through the anterior leg of the external capsule into the temporal lobe and gives branches to the middle and lower temporal gyrus, as well as the occipital lobe [9]. When stimulating this beam, semantic paraphasias are observed in the experiment [10]. Dorsal flow, in turn, is related to extended syntax and is evolutionarily later and perfect [11].
In speech perception activation of interested structures is asymmetric [12-14]. Differences were found in the activation of parietal and frontal centers: it is shown that the latter are characterized by a large degree of lateralization, this indirectly indicates in favor of the possible bilateral activity of the ventral flow, which, however, as the level of treatment increases to a more complex one, is “interrupted” by a more lateralized dorsal [15]. There is mutual activation between symmetric speech structures of different hemispheres. What is observed in healthy patients as equilibrium [16]. The left hemisphere is logical, and the right emotional and creative, for example, specifically-shaped thinking, tasks related to the manipulation of objects, images. The left hemisphere is more specialized for recognition of time characteristics, and the right hemisphere is more specialized for recognition of frequency characteristics [17]. This distribution was shown for the anterior part of the upper temporal gyrus, where information is processed immediately after the primary auditory cortex [18]. This is confirmed, for example, by recent tractographic analysis [19].
Scientists at Carnegie Mellon University and Minnesota State University have been able to create a virtually non-invasive technology that will allow paralyzed patients to control mechanisms and robotic prostheses with the power of thought. To do this, they had to overcome the main problem of non-invasive neurointerface: unlike the implant, it receives a much more noisy signal, and therefore, the accuracy and speed of control decreases. With the help of the latest sensors and machine learning, the researchers were able to get signals from the depths of the brain, clear them of interference and for the first time achieved high quality control by a robotic hand, On the BrainBit neurointerface tape there are 4 dry EEG electrodes, reference and common electrodes, as well as a miniature electronic module. This allows you to register a professional electroencephalogram with the best quality among the neurointerfaces available on the market. The device amplifies and digitizes the received signal and transmits it using the Bluetooth protocol to a computer, smartphone or tablet. Unlike analogues, the position of the electrodes on the tape BrainBit corresponds to the international arrangement of electrodes 10-20. Electrodes provide direct contact in areas of temporal lobe T3 and T4, as well as in occipital region O1 and O2. According to advanced international studies, these zones are optimal for recording the level of four main types of brain waves. BrainBit records electrical activity in the form of “raw data” of EEG, which are presented as levels of the four main rhythms of the brain. All brain activity data obtained can be sent to the cloud for analysis and processing by machine learning methods. The BrainBit SDK contains a set of tools for developers that allow you to obtain both raw EEG data and calculated values of brain activity rhythms. The SDK facilitates complex data processing and analysis by simplifying application development. The application can display the state of the user’s brain based on color indicators. These graphical indicators complement qualitative and quantitative indicators demonstrating the current state of the brain.
Mental Lexicon
A mental lexicon is a collection of word information that includes the actual meaning of a word, a semantic component, a syntactic component, as well as perceived and reproducible forms of words [2]. In the mental vocabulary, the brain finds and learns what we ourselves are going to fish. We are trying to look where our thought processes take place into the mental lexicon [2].
Firstly, morphemes are considered its smallest unit – minimal meaning-containing units [2]. These are roots, suffixes, prefixes. At the same time, the mental lexicon can have several levels, and on one of them the minimum unit will be a word.
Secondly, it is not a list that is sequentially viewed, but a network where each unit is associated with many others. The essence of such an organization is that words related in meaning are often used in the same mental situation, and if internal talk is about one, it would be wise to keep the rest carefully. The more often words are used together, the stronger the connection between them, the more inclined it is to move along this connection during the associative process. Freud’s invented free association method confirms this.
Thirdly, the mental lexicon does not have one organizing principle, but several at once. The master is semantic, that is, the connections are made by value. The importance of this principle is proved by the semantic priming effect, in the Russian-language literature the term “precedence effect” is used. Two words are used in the experiment: “previous” is always a real word, and “target” can also be a real word, a pseudo word that is built in accordance with phonetic principles, but is not in the language, or simply an unreadable set of letters. The subject needs to click the button to decide whether the target word shown to him is real, a pseudo word (similar in structure to the present, but non-existent, as a “deep cusd”) or an impracticable set of letters – the so-called situation of the “lexical solution.” If the “previous” word is associated in meaning with the “target,” the subject performs the task many times faster: the memory has already passed to the “catalog section” in which this word was in one semantic bundle, it remained only to find it [2].
The mental lexicon is central to the organization of internal speech. Each word is present in the “library” in all grammatical forms, for example, the times of verbs or the genera of adjectives. Due to this, semantic and syntactic information is extracted simultaneously at the lexical access stage. When calling the word “red,” the names of other colors, red objects and others associated with it are activated in the semantic network (Figure 1).
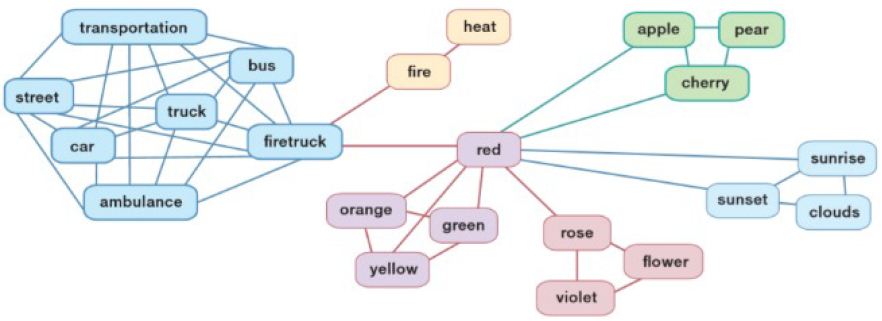
Figure 1: Semantic principle of mental lexicon organization
Lexical selection is the stage at which, among all activated word forms, the most suitable is selected. Lexical integration is the combination of all words into larger structures: phrases, sentences, up to whole internally connected texts. The preparation of texts includes macro and micro planning.
Communication is one way to influence the environment. Therefore, communication, like any action, is subordinate to the motivational sphere and can be aimed at meeting the need or eliminating inconvenience. On the example of instructive expressions, this can be seen especially clearly, but our other statements seem to have the same goal, because there are simply no other sources of motivation. Thus, any statement should be formulated based on the result that we want to receive – this aspect of the preparation of the message is called macro-planning. When microplanning, the question is developed how the information should be presented: which group of words to use, in which relationships to put them. After preparing the message at the output, a “concept” is obtained, the general meaning of the whole sentence.
The mental lexicon is a specific concept, and it manages smaller, more formal units than the “repository of concepts.” Similarly, only people can be the bearers of ideas that really understand them, and although all the rich variety of expressions for these ideas are stored in the library, only books that read them “animate.”
The formulation of expressions is to give the sentence a specific form, grammatical and phonetic, ready for pronunciation. The concept obtained in the first stage interacts already with the mental lexicon; the first thing to decide on is part of internal speech. At the output, we get the corresponding lemma – the initial form of the word. Many different word forms are associated with lemma. According to the grammatical principle, lexical selection of word forms occurs. Then there is morphemic analysis. The resulting word will need to be called, preparation for which is phonological analysis: analysis of the number of syllables and the position of emphasis in the word.
There is little neuroscience evidence that addresses the issue of mental lexicon; they make it possible to create a holistic picture. Elizabeth Warrington and colleagues investigated the problem of selective items belonging to only one category, and how they can relate to semantic memory. It turned out that semantic memory is divided into “categories.” In our mental vocabulary, not every word is connected with each so that you can come to it in a different way; some kind of division, dispersal is still there. Warrington identified such groups: living beings, which are mainly associated with terms describing their appearance and other properties perceived by the senses; and artificial objects – they are usually described by the function that they perform.
Human Holographic Consciousness
Human consciousness, like a hologram, contains everything that is in a multiple updating system from finite shifting professions. The hologram of consciousness is the basis for storing information about human life.
The principle of the hologram “everything in each part” allows a fundamentally new approach to the issue of organization and order. The hologram shows that some things cannot be investigated by an analytical method: to dissect an object and study its constituent parts. If we dissect anything on the hologram, then we will not get the parts of which it consists, but we will get the same, but with less accuracy.
Our ability to quickly find the right information from the vast volume of our memory is provided by a brain that works on the principle of a hologram. Indeed, one of the most amazing properties of human thinking is that each piece of information is instantly and mutually associated with the other – another property inherent in the hologram.
Memory location is not the only neurophysiological mystery that has become more solvable in the light of Pribram’s holographic brain model. The other is how the brain is able to translate such an avalanche of frequencies that it perceives by various sensory organs (frequencies of light, sound frequencies, and so on) into our specific idea of the world. Frequency coding and decoding is exactly what the hologram handles best. Just as the hologram serves as a kind of lens, a transmitting device capable of turning a apparently meaningless frequency interfere into a coherent image, so the brain, according to Pribram, contains such a lens and uses the principles of holography to convert frequencies from the senses into the inner world of our perceptions.
Pribram’s idea that our brains construct solid reality by relying on input frequencies has also received experimental confirmation. It has been found that any of our sensory organs has a large frequency range of susceptibility. In particular, the researchers found that our visual organs are susceptible to sound frequencies, that our sense of smell depends somewhat on what is now called osmotic frequencies, and that even our body cells are sensitive to a wide frequency range. This is the work of the holographic part of our consciousness, which converts separate chaotic frequencies into continuous perception.
The holographic model also shows that consciousness is not a function of the brain, but, on the contrary, the neural networks of the brain are controlled by consciousness, which, therefore, does not die if the brain dies. In holographic reality, thought is as real as consciousness.
A single universe has projections in the form of a discretely updated frequency wave-like structure – a hologram, the main content of which is consciousness, which is its copy. Discrete update of the projection by consciousness means the appearance of durations, which qualifies as time.
A single universe enters time by means of its own projection in the form of a frequency wave-like structure – a hologram, forming its own time and at the same time – the general of the entire structure of being due to its holographic essence (the whole and part coincide). The active living in the holographic projection of the Single, copying fragments of the passive from the Single, are combined with them individually and as a whole, and through themselves form the current time, space and things in motion.
The conversion of wave matter (packets of information) from the holographic projection of the Single in any living creature, including in man, into his environment, is carried out by him no longer in the form of images, but in the form of material objects of different “density” and various forms using the corresponding matrices (shaping abilities), creating both the living being itself and its environment within the framework of common time, which is the consequence of the action of a single consciousness in a combined set of living beings.
The formation of objects of various forms in accordance with the mass-forming abilities (matrices) of a living creature is carried out according to the type of work of a 3D printer.
The holographic image of living beings allows them to be separate, living each time their own life, having their own time, their own being, and at the same time in their totality – to be a single being that is eternal both in its singularity and in each of its own.
As for the genome, it is based on a program copied by consciousness in a projection from the Unified to the molecular chains of the genome in accordance with its existing shaping abilities for each particular case.
Information is an activity property. Without material objects-carriers, including consciousness itself, information does not exist. For each person, discrete information is automatically (with the help of a single consciousness) converted into things, images, meanings, feelings, which are also quite material components of each individual consciousness, entailing subsequent actions of the carrier of consciousness.
Living beings are involved in the information process. With the help of information processing centers, they are able to immerse themselves in a liveable environment. All human achievements are connected in the form of acquired experience in this field, existing knowledge and skills with certain target focus.
In the form of light and sound, a person can approach the harmony of his own wave basis of the ideal, which is actually the holographic basis of a person.
The time of any living creature, in particular, and man, is an information process during which material objects are recognized by consciousness by scanning the environment by the processing centers at its disposal. The informational (impulse) nature of time formation is asymmetric (one-sided), differing from the usual real or energy interactions of objects in that a living being unilaterally scans the surrounding one, sequentially copying the data recognized and grouped by it. This high-frequency complete update of one position of the next, etc., in particular, does not allow you to go back or run forward due to the asymmetry (one-sidedness) and completeness of the update of each position. Therefore, it seems to each person that time flows in one direction: from the past to the future through the present. Due to the complete updating of one position by another, that is, irretrievably and infinitely, in the form of an infinitely updated ultra-high-frequency wave-shaped holographic projection in the form of intermittent moments-durations (pulses of information).
For humans, information passes every moment to brain neurons from different human sensory organs in the form of sequences of nerve impulses; each of the pulses contains corresponding information. Immediately after the pulse generation, the nerve fiber is in the so-called refractor state, and cannot be reactivated for 1-2 milliseconds, that is, the nerve fiber is able to conduct nerve pulses with a frequency not higher than 500 hertz. The duration of the pulse itself passing through the nerve fiber is a fraction of a millisecond in each moment.
A pause between nerve impulses containing information means that they do not go continuously. However, this pause is below the threshold of perception by her consciousness and therefore does not fall into it. In particular, the moving picture for human consciousness is provided by an interval between the run-through successive frames of about 0.04 seconds, which is said threshold. Its duration, as you can see, is more than an order of magnitude longer than the duration of the pause. Therefore, the resulting discrete sequential moments (in each of them there is an update of the “reality”) of a person’s own time, which contain in their sequence all the paintings and all the events of life for a person, merge into a continuous, inseparable flow in his mind.
Each person, starting from the moment of birth, selects through sensations from a diverse environment only those information that can be deciphered, or information, in accordance with the achieved level of consciousness development (shaping abilities). The holographic approach to the structure of consciousness fully reflects the connections of various regions of the brain.
Holographic Recording of Internal Speech
Magnetic resonance imaging (MRI) today is used not only for diagnostics, but also for mapping the functional state of neural networks, allowing you to literally see the brain’s work in real time [20-24].
The ability to directly observe the dynamics of cognitive (cognitive) brain activity appeared only with the introduction of functional magnetic resonance imaging technology into research practice.
A little more than two decades ago, employees of the American research organization AT&T Bell Laboratories described the principle of visualizing the activity of brain zones in real time using magnetic resonance imaging (MRI). A dynamic study of active zones of brain structures at the time of their activity was first tested on a person two years after the first publication.
MRI (magnetic resonance imaging) is a diagnostic procedure based on the effect of nuclear magnetic resonance. Modern MRI techniques allow not only to visualize organs with high quality, but also to investigate their function. Due to the absence of ionizing radiation, this method can be used without restrictions and repeated studies are repeatedly carried out.
It follows that the relative magnitude of the MRI signal can serve as a measure of the activity of brain zones. Moreover, the results obtained under the control of electroencephalography on the visual cortex of the primate open brain suggest that the MRI signal is a linear response to the electrical activity generated by the active neural ensemble.
Functional MRI focused on BOLD effect detection is today the optimal tool for mapping neuronal activity, more precisely, the functional state of neural networks – the basis for visualizing our holographic images in real time.
Closely related to fMRI technology is the neurobiological technology “of the brain-computer interface. We are talking about the possibility with the help of an electroencephalogram to obtain a display of a stable hologram of the bioelectric activity of the brain, tying it to the function of brain structures and the formation of new stable neural ensembles in them. The electroencephalogram is a source of information on intracerebral events. At the same time, fMRI makes it possible to visualize the real temporal and spatial dynamics of the brain. If you briefly describe the most general route of activation of brain structures during internal speech, then after the start, the broad cortical fields of the brain are first involved in the work, and the cognitive route in the cerebellum ends.
Psychology is one of the most promising areas of use of neuroimaging technology by FMRT, because this scientific field is practically devoid of ideas about the localization (in the anatomical sense) of cognitive functions.
In one of the works of American researchers, an attempt was made to answer the question of the localization of brain structures designed to classify such cognitive categories as equality and efficiency. It turned out that the emotional assessment of the “effectiveness,” “justice” and “general benefit” of the decision is carried out by three different brain structures. The brain department, called the “shell” (lat. Putamen), is responsible for efficiency, the bark of the “islet” (lat. Insula) protects the interests of justice, a cumulative measure of efficiency and inequality, that is, utility, assesses the septal organ (lat. Septum), while other areas of the brain are involved in the cognitive process.
The development of cognitology, a direction of neurosciences that studies the basic mechanisms of the brain’s work: “mental strategies,” their localization, dynamics, ways of using and improving in everyday life, also opens up great prospects. The so-called “interactive stimulation” makes it possible to organize training feedback directly through the “interested” brain structure (Figure 2).
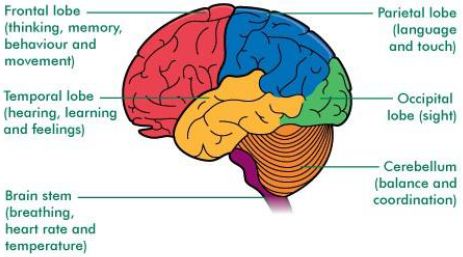
Figure 2: Brain functions
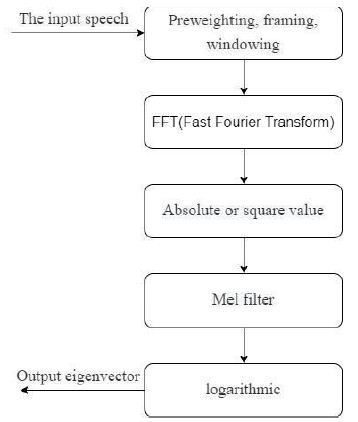
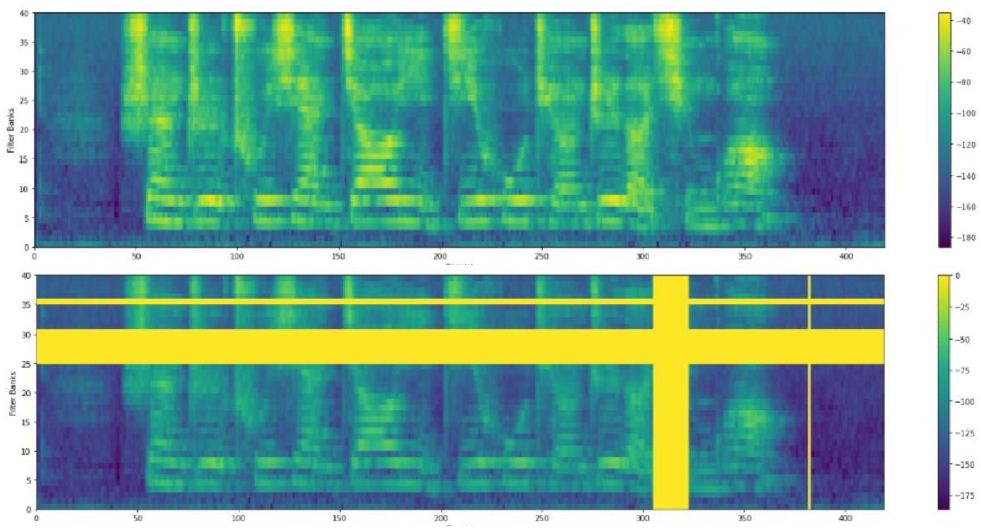
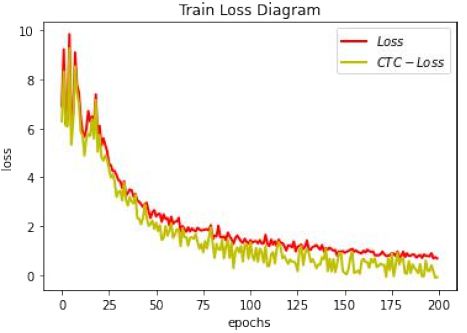
By visualizing the cingulate gyrus or hippocampus, you get a chance of “direct conversation” with the brain. Knowing how the brain is activated, you can restore the holographic image of internal speech by a resonant energy trace. Using nanoresonators with Fourier transducers, brain activity of human internal speech holographic image can fix mental noninvasive neurointerface in language form by mental lexicon [25,26].
Conclusion
Thanks to the development of holographic methods, technologies and the creation of smart neuroiterfaces, in the coming years humanity can move to a completely different world in which everything will be technological. Almost all modes of transport will be controlled through neurointerfaces with smart artificial intelligence. Human thinking will be a kind of hybrid of biological and non-biological. We are considering the prospect of connecting to the cloud from the human neocortex. Already, we can connect a computer to the human brain and thus convey feelings and emotions to the Internet. It will be possible to read memories and impressions from the human brain, transmit them over the Internet or even upload them to the brains of other people. This will open the way to turning the Web into a brain-net, that is, a brain-net. You will be able to share your memories and load them into a break-no, and then loved ones with their eyes and heart knock via smart neurointerface will survive your events and experience joy. Neurointerfaces with intelligent artificial intelligence and technological singularity are already in demand in the industrial and social spheres. Especially in environments and situations incomprehensible to the consciousness of specialists, where huge risks arise.
References
- Chuprikova NI (2017) Differential integration theory of development as the basis for solving the problem of the relationship of language and thinking. Differential Integration Theory of Development 2: 165-190.
- Gazzaniga, Michael S, Richard B Ivry, Mangun GR (2014) Cognitive Neuroscience: the Biology of the Mind. Fourth edition. New York: W. W. Norton & Company, Inc.
- Roux FE, Boulanouar K, Lotterie JA, Mejdoubi M, LeSage JP, et al. (2003) Language functional magnetic resonance imaging in preoperative assessment of language areas: correlation with direct cortical stimulation. Neurosurgery 52: 1335-1347. [crossref]
- Friederici AD, Weissenborn J (2007) Mapping sentence form onto meaning: The syntax–semantic interface. Brain research 1146: 50-58. [crossref]
- Penfield W, Roberts L (2014) Speech and brain mechanisms. Princeton University Press.
- Sidtis DVL, Rogers T, Godier V, Tagliati M, Sidtis JJ (2010) Voice and fluency changes as a function of speech task and deep brain stimulation. Journal of speech, language, and hearing research 53: 1167-1177. [crossref]
- Chang EF, Raygor KP, Berger MS (2015) Contemporary model of language organization: an overview for neurosurgeons. Journal of neurosurgery 122: 250-261. [crossref]
- Hickok G, Poeppel D (2007) The cortical organization of speech processing. Nature reviews Neuroscience 8: 393-402. [crossref]
- Sarubbo S, Benedictis AD, Maldonado IL, Basso G, Duffau H (2013) Frontal terminations for the inferior fronto-occipital fascicle: anatomical dissection, DTI study and functional considerations on a multi-component bundle. Brain Structure and Function 218: 21-37. [crossref]
- Mandonnet E, Nouet A, Gatignol P, Capelle L, Duffau H (2007) Does the left inferior longitudinal fasciculus play a role in language? A brain stimulation study. Brain 130: 623-629. [crossref]
- van der Lely HKJ, Pinker S (2014) The biological basis of language: Insight from developmental grammatical impairments. Trends in Cognitive Sciences 18: 586-595. [crossref]
- Specht K (2013) Mapping a lateralization gradient within the ventral stream for auditory speech perception. Frontiers in human neuroscience 7: 629.
- Bemis DK, Pylkkänen L (2012) Basic linguistic composition recruits the left anterior temporal lobe and left angular gyrus during both listening and reading. Cerebral Cortex 23: 1859-1873. [crossref]
- Friederici AD, Bahlmann J, Heim S, Schubotz RI, Anwander A (2006) The brain differentiates human and non-human grammars: functional localization and structural connectivity. Proceedings of the National Academy of Sciences of the United States of America 103: 2458-2463. [crossref]
- Price CJ (2010) The anatomy of language: a review of 100 fMRI studies published in 2009. Annals of the New York Academy of Sciences 1191: 62-88. [crossref]
- Häberling IS, Steinemann A, Corballis MC (2016) Cerebral asymmetry for language: comparing production with comprehension. Neuropsychologia 80: 17-23. [crossref]
- Witteman J, Goerlich-Dobre KS, Martens S, Aleman A, Van Heuven VJ, et al. (2014) The nature of hemispheric specialization for prosody perception: ERP evidence. Towards a Cognitive Neuroscience of Prosody Perception 63.
- Mitchell RLC, Ross ED (2013) Attitudinal prosody: What we know and directions for future study. Neuroscience & Biobehavioral Reviews 37: 471-479. [crossref]
- Frühholz S, Gschwind M, Grandjean D (2015) Bilateral dorsal and ventral fiber pathways for the processing of affective prosody identified by probabilistic fiber tracking. Neuroimage 109: 27-34. [crossref]
- Bakulin IS, Poydasheva A, Medyntsev A, Suponeva N, Piradov MA (2020) Transcranial magnetic stimulation in cognitive neuroscience: Methodological basis and safety. Russian Journal of Cognitive Science 7: 25-44.
- Lanfang Liu, Xin Yan, Hehui Li, Dingguo Gao, Guosheng Ding (2020) Identifying a supramodal language network in human brain with individual fingerprint. NeuroImage 220: 117131. [crossref]
- Nima Asadi, Yin Wang (2020) A heuristic information cluster search approach for precise functional brain mapping. Human Brain Mapping 41: 2263-2280. [crossref]
- Xiaoxiao Wang, Xiao Liang, Zhoufan Jiang, Benedictor Nguchu A, Yawen Zhou, et al. (2020) Decoding and mapping task states of the human brain via deep learning. Human Brain Mapping, 41: 1505-1519.
- Takumi Mitsuhash, Masaki Sonoda, Jeong-Won Jeong, Brian Silverstein H, Hirotaka Iwaki, et al. (2021) Four-dimensional tractography animates propagations of neural activation via distinct interhemispheric pathways. Clin Neurophysiol 132: 520-529. [crossref]
- Evgeny Bryndin (2021) Mental Communication of Internal Speech with Communicative Associative Robot via Spectral Neurointerface. American Journal of Applied Psychology 10: 55-64.
- Evgeny Bryndin (2021) Resonance Technology of Communication of Specialists via Mental Neurointerfaces. International Journal of Neurologic Physical Therapy 7: 7-13.