DOI: 10.31038/IDT.2021223
Abstract
By critically analysing and exploding the key foundation myths that have arisen around the origin, mode of spread and immunity on COVID-19 we lay out the evidence and critical arguments supporting an immediate end to all COVID-19 justified lockdowns. These emergency laws, invoked by many previously free and democratic societies, involve social distancing, obligatory wearing of masks, limited crowd sizes and gatherings (funerals, weddings, religious gatherings, sporting fixtures etc), the closures of schools and many small and large businesses not deemed necessary to containing the virus, border closures, and thus free travel movements, domestic and international. The basic premise in all these dictums is that the primary mechanism of spread of COVID-19 is assumed via person-to-person contacts only. We show this premise to be false. Our recommendations are anchored in the key relevant evidence and observations of the past two years gathered by us and published in a series of papers through 2020 and 2021. Our analysis documents the plausible putative first cause to the arrival of COVID-19 from space in a carbonaceous meteorite bolide the in stratosphere over China on October 11 2019; and then its blanket China-wide viral-laden meteorite dust contamination through November-December 2019 followed by further global dispersal of these viral-laden meteorite dust clouds by prevailing stratospheric and tropospheric wind systems, including human passaged virus aerosol-plumes adding to lower level (tropospheric) viral laden clouds. We explain why all lockdowns of any type cannot possibly work in principle against viral dispersal and transportation of this type – emergence of new clusters of disease, with poor evidence of connectivity through contact, clearly does not support person-to-person infections as the primary cause of spread. The initiation of mass infective events (“Mystery Cases”) in each regional and localised COVID-19 epidemic is caused by unsuspecting victims most likely catching the virus by rubbing up against a virus contaminated environment. We also deal with the efficacy of current vaccination roll outs on population-wide scales. It is most unfortunate that currently available mRNA expression vector vaccines, delivered by the intramuscular route (“Jab in the Arm”), may not only be dangerous in inducing many putative adverse reactions as their human safety is untested, they also cannot protect in principle against common cold and other respiratory pathogen infections like COVID-19 that arrive via the oral-nasal route. That evidence is discussed along with our recommendations for mankind’s preparedness for future suddenly emerging pandemics of this type.
Introduction
We have published recent papers that review the evidence that the prevailing global wind systems are the primary distributors of COVID-19 viral-rich clouds [1-3] and a detailed summary of the analysis of a clear set of mystery outbreaks in Victoria, Australia May-June 2021 [4] which constitute unequivocal evidence of a non-person-to-person introduction of the virus. These airborne viral in-falls from the troposphere have resulted in significant region-wide environmental viral contaminations, both small and large scale across the globe, of meteorite-derived viral-laden dust clouds. These include sudden strikes of COVID-19 outbreaks on crew and passengers on ships at sea [5,6] islands such as Sri Lanka that had avoided the epidemics until Oct 6 2020 [7] and the remote Chilean O’Higgins Army Outpost in Antarctica where most of the personnel were struck down suddenly and simultaneously with COVID-19 in late Dec 2020 [3].
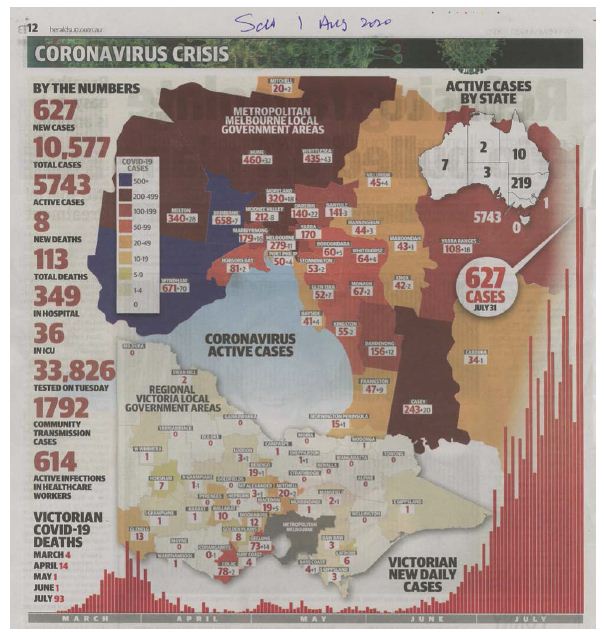
While some infections can theoretically be caught by victims from breathing in viral-laden dust particles in the air, the case Incidence maps which show the stability of an infected zone outbreak in carefully analysed specified regions (as an example, selected parts of the State of Victoria in Australia and State New South Wales, covering pre-Winter and Winter months May-Sept both 2020 and 2021) suggest alternate explanations. We surmise that most infections are caught by unsuspecting victims from contact with a virus-contaminated environment (e.g. contaminated fingers or contaminated face masks themselves) with subsequent transfer to portals of entry via oral-nasal passages, initiating an infection in the lining of the respiratory tract. Case Incidence maps for Victoria, Australia and the prevailing weather directions of rain visiting Victoria from Southern Ocean are shown in Figure 1a and 1b.
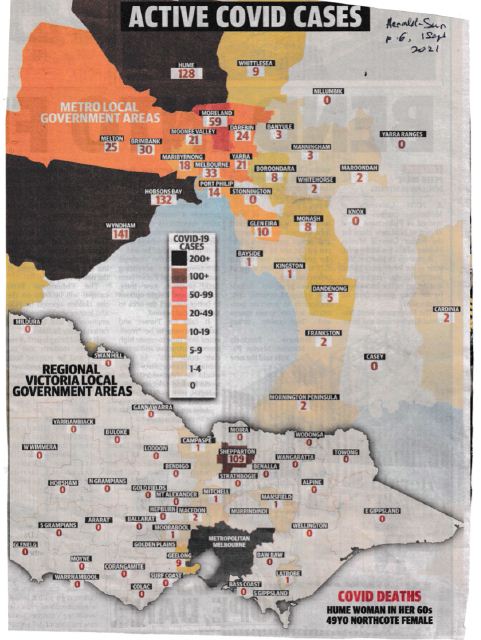
Figure 1a: Map of COVID-19 outbreaks (40-50% Mystery cases) in Victoria Winter 2021. Note the whole town of Shepparton 190 km north of Melbourne was a cluster of numerous and sudden mystery outbreaks (unlinked genomically in sequence to Melbourne ‘Delta’ outbreaks according to newspaper reports) as Melbourne was sealed off by a ‘ring of steel’ hard lock down with night time curfews, no movement in or out of Melbourne, no travel through country regions, and the border with New South Wales was sealed by police, army and surveillance drones.
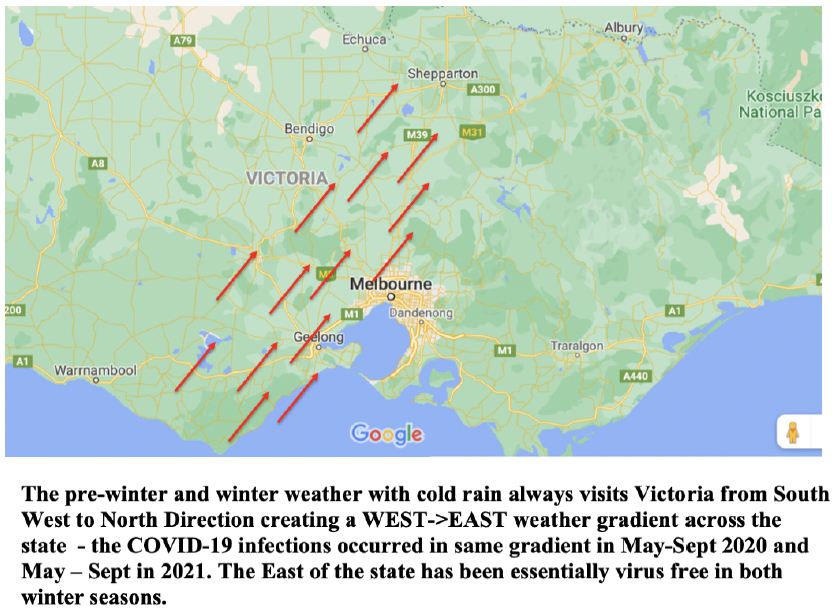
Figure 1b: Infection arc of Figure 1a showing very similar to prevailing Winter weather into Victoria from the Southern Ocean. Notice that the East of the State (Figure 1a) is basically virus free. The same pattern was observed in 2020 (see Appendix A).
The viral-laden dust clouds would need to be brought down to ground by local precipitation (rain). This likely occurred through most of 2020 across the globe given the localised stability of regional outbreaks (USA, Europe, Pakistan, Japan, South Korea, South Africa and the Indian subcontinent), particularly through April-May 2020 on the 40° N Latitude band prior to the strike on New York City. Early outbreaks in South Korea and Japan were also centred on this latitude line [1]. On either side of this line, during this 2020 time interval, there were many countries which represented infection “null zones”, which soon became engaged north and south of the 40° N line (France, United Kingdom, most countries in Europe and Russia and Scandinavian countries). Subsequently we have suggested that the putative meteorite viral-laden dust clouds then washed down and entered the Southern Hemisphere over the Atlantic Ocean [2]. The viral clouds were then brought to Australia in 2020 along the 40° S latitude Line, via the W->E Roaring Forties prevailing winds to Victoria and to a far lesser extent into NSW, Australia (May-Sept 2020, and then again in 2021, including the significant out breaks in French Polynesia 2020-21 as well as small outbreaks in New Zealand [3]. In Australia in both winters Western Australia (Perth), South Australia (Adelaide), Tasmania (Hobart, Launceston), and Queensland (Brisbane) were all null zones, only suffering transient outbreaks via infected international passengers entering by jet planes. It is very important to understand such null zones, as they confirm the annual regularity of the prevailing wind and weather systems – the COVID-19 strikes in Australasia were clearly governed by these predictable weather systems.
Later in the year 2020, and into 2021, the main spreads and regional in-falls could well have been of human passaged COVID-19 rich viral dust clouds generated by the significant tropospheric plumes of viral aerosols above United Kingdom, India, South Africa, Brazil and other countries through the later months 2020 and through 2021 [4]. Other genomic and epidemiological evidence to be referred to here is an analysis of >12,000 full length COVID-19 genomes and associated epidemiology data publicly available from the 2nd Wave COVID-19 epidemic in Victoria, Australia June-Sept 2020 [8]. This analysis builds on the COVID-19 full length genome analysis in clear hotspot epidemics in [9]. Here we expose to critical scrutiny the unscientific myths in wide mainstream media circulation (and also actively promoted by the same media particularly the global News Ltd media) which has driven the global response of all governments and their health authorities.
What Actually Happened in China Late 2019 and Early 2020?
Before exposing the key circulating myths we must have a clear-eyed view of what actually transpired in China late 2019 through January 2020, and into the explosive exponential rise in COVID-19 case numbers per day in January 2020 [9]. The earliest confirmed cases in retrospect emerged from late October-early November [10]. The widely discussed data is based on the Wuhan epidemic in Hubei province central China but it is clear from all the data collected at the time from across China that a series of China-wide explosive epidemics occurred simultaneously (Figure 2). Any explanation has to manage this clear fact – tens to hundreds of millions of Chinese were exposed and succumbed to COVID-19 infections over a short time period, too fast for any type of person-to-person (P-to-P) spread as is commonly assumed by mainstream epidemiological theory and bat-human and most Lab leak conspiracy theories.
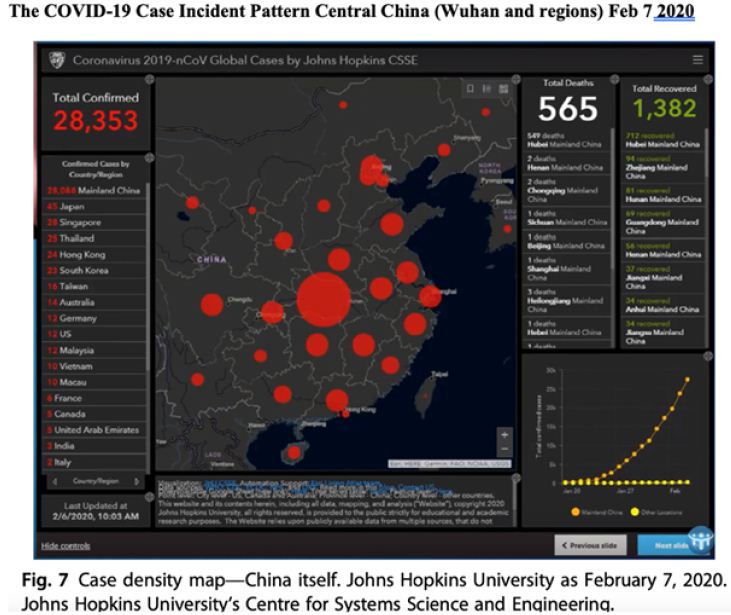
Figure 2: This is Figure 7 discussed in depth in Ref [11], Steele EJ, Gorczynski RM, Lindley RA, Tokoro G, et al. (2020) Origin of new emergent Coronavirus and Candida fungal diseases- Terrestrial or Cosmic? Advances in Genetics 106, 75-100 https://doi.org/10.1016/bs.adgen.2020.04.002
Current Myth#1
The COVID-19 pandemic began with a sudden explosive animal – to – human jump on China-wide scale of the earlier SARS-CoV-1 now in a bat or pangolin reservoir in South East Asia.
Both we and mainstream viral molecular evolutionists (e.g. Professor Andrew Rambaut, University Edinburgh; Professor Ed Holmes, University of Sydney) agree such a jump is statistically impossible on the basis of all existing SARS-CoV-2 “like” sequences isolated from putative bat, pangolin or cat reservoirs. We discuss these data and calculate the odds of a “jump” giving a COVID-19 sequence match [6]. For the closest known bat sequence, 96.2% similar to COVID-19 across the full length 29903 nucleotide (nt) positions of the Wuhan or Hu-1 reference sequence, the probability of getting a match of a correct nucleotide substitution at approx. 1100 positions is of the order one successful trial in 10684 random trial jumps. If we are generous and assume there is a sequence of 99% similarity to COVID-19 lurking in some unknown bat or pangolin animal reservoir it is 10184. If the reader has difficulty grasping the essence of such astronomical numbers a good comparator number is 1084, the number of Hydrogen nuclei in the known Big Bang Universe (H atoms quantitatively dominate the known Universe). So getting a successful jump outstrips, by many orders of magnitude, the molecular and statistical resources of the known universe. To re-state the obvious conclusion: this infection did not come from an infected bat via wet market contact (supported also by all the early reports that exclude such ‘origin’ sources on other grounds [11-13].
Current Myth#2
The COVID-19 pandemic began with a sudden explosive release of a genetically engineered virus just like COVID-19 (the full length 29903 nt Hu-1 sequence) from the Wuhan Institute of Virology. This has been actively and strongly pushed by Professor Nikolai Petrovsky (Flinders University), Sharri Markson the lead investigative journalist in News Ltd in Australia, other writers in The Australian newspaper, many Fox News Channel (News Ltd) talking Heads eg Tucker Carlson Tonight and others on FNC) and many writers in The Wall street Journal (News Ltd) and The London Times (News Ltd, including Professor Luc Montagnier [14]). It is a fair assessment that the News Ltd media in particular has actively pushed this Cold War Conspiracy. Theory propaganda globally on a massive scale. Ex-president Trump also argued the same case with his ‘China Virus’ accusations in 2020, despite having been told this story was most likely false “in a big power telephone communication” on Feb 6 2020 with President Xi – see Appendix B, pages xviii-xix Bob Woodward’s book Rage: “It goes through the air,” Trump said. “That’s always tougher than the touch. You don’t have to touch things. Right? But the air, you just breathe the air and that’s how it’s passed. And so that’s a very tricky one. That’s a very delicate one.”
Notice that none of the material put out by those advocating a human-engineered cause (Petrovsky, Markson, Carlson, Montagnier et al ) ever attempts to grapple with a wealth of precise facts that need to be considered (see Figure 2). Our own explanation of a natural cosmic cause is plausible in terms both of timing and location, given the Oct 11 2019 meteorite strike over Nth East China [15,16], and all existing historical and recent knowledge on life bearing carbonaceous meteorites arriving in the stratosphere prior to COVID-19 [17-19]. Our analysis comes to grips with this explosive first strike (Figure 2) of putatively tens of millions of mystery infections imposed across a vast area of China (Dec 20219-Jan 2020) and the subsequent sequelae of epidemics (and genetics of the virus) on the ground in the first few months after Oct 11 2019, first in China, then elsewhere in South East Asia, Western Pacific, then Iran, Italy, Spain and New York City [1,6,9]. Of course, following a mystery infection (falling from the sky) there would then be person to person (P-to-P) spread to close contacts and to close uninfected family members (the genetic data from the Wuhan sequences suggest 1 or at most two P-to-P transfers, [9]). This we do not deny. Such a human passaged transmission would have begun immediately in China, resulting eventually in a rising aerosol plume of human passaged COVID-19 virions being lofted into the troposphere above China. The infective strikes on the cruise ships in the South China Sea and Sea of Japan (Diamond Princess, Westerdam), the USS Theodore Roosevelt aircraft carrier (May 2020, north Pacific Ocean) and the sudden strike in late February 2020 on the other side of the Pacific Ocean on the Grand Princess cruise ship, support lower level West -to-East global transport of the Wuhan human passaged viral plume cloud across the Pacific in this time interval [3]. This is consistent with the available genetic evidence viz. unmutated and lightly mutated Hu-1 sequences (L or in Pango, B) among infected passengers/crew on that ship [9].
The meteorite viral-laden dust cloud arising from a cometary strike over Jilin, North East China on the 40° N line on the night Oct 11 2019 was, we believe, the likely first deposit of viral-laden dust into the stratosphere above China – and its East to West stratospheric jet stream transport ensured global spread – coincident with a first ground strike by the direct faster fall of a fragment of the viral-laden meteorite cloud to ground blanketing China through November and December 2019, although still centred on Wuhan. The estimate of the earliest cases in November fit this explanation [10]. This explanation is consistent with all known facts about the early months as the pandemic ignited in China. It is far more plausible and parsimonious than the animal jump or Lab leak theories, and does not require multiple additional, and implausible, assumptions (further discussed below and Appendix C). The cause of the many genuine ‘mystery cases’ observed in Victoria (and NSW) in Australia in 2020 [8], and 2021 needs to be interpreted in the same way, but on a far smaller scale of infection numbers [4]. The stability of the infection arc over two winters in Victoria (Figure 1 and Appendix B for 2020) implies prevailing weather patterns. The null zones of Perth (Western Australia), Adelaide (South Australia), Hobart & Launceston (Tasmania), Brisbane (Queensland), despite all the political finger pointing in Australia, are most simply explained as arguing that all those other Australian states were lucky- they were not in the “teeth” of prevailing weather winds and in consequence they have avoided the political, social and economic mayhem which has followed the “conventional dogma explanations”.
Implausibility of Lab Leak Theories
We next turn attention to confront in detail and properly assess the “Lab Leak Conspiracy” theories that are gaining widespread apparent momentum and respectability in the public mind. As stated above these models require multiple additional, and in our view implausible, assumptions, which are discussed in depth in a series of numbered points (below and Appendix C). In exploring in detail the implications of the ‘Predictions’ of this theory, as we would for any scientific theory, which must be tested also for coherence and robustness, and here to, by necessity, we will limit the number of tacit and overt assumptions (and Appendix C). The advantage of the latest claims is we can examine the predictions. The claim now is that an engineered COVID-19 virus culture at very high titre and thus dose was somehow deposited in the stratosphere and thus entered into the global weather system over China. In our view this is a concocted and politically convenient cold war conspiracy fantasy (Sharri Markson Wed 15 Sept 2021 p.1 The Australian newspaper “Revealed: US failed to act on Covid-19 intelligence, says Wei Jingsheng”, the latter is a Chinese defector to the USA).
In exploring the implications and predictions of this assertion for coherence and scientific plausibility, readers must also stay aware of the scientific plausibility of the argument, critique any data put forward to support it, and ask themselves whether it even “makes sense” to imply a ‘human purpose’ and ‘motivation’ for a first strike stratospheric cause which fits the observed and sudden China-wide infection data (vide supra). We have already made clear that in our view all the available scientific data is consistent with the pandemic being a natural phenomenon – like that which occurred 100 years ago in an era before viruses were not fully characterised and a time when DNA/RNA genetic manipulation biotechnology did not exist. As we shall show the assumptions needed to defend a conspiracy alternative are ad hoc, without independent evidence, and so also are the number of additional concepts needed to reconcile with the available epidemiologic and genetic data
Points to Consider as Arguments in Favour of a “Lab Leak Conspiracy”
- A balloon launch or drone plane flight released a viral ‘bomb’ in the stratosphere over China. There is no reported evidence, from China, US or European satellites of a balloon launch, drone flight, or spy-plane which could be responsible, in Oct-Dec 2019. No coherent argument (political) has been suggested for who might have been responsible for such a strike, and why.
- If it was from outside China, one would expect the Chinese military to have neutralised it quickly and for there to have been political repercussions-it is hard not to expect repercussions detected by the rest of the world if a launch occurred from within China itself. The viral vector vehicle is postulated to harbour a pure culture of COVID-19 virions with an exact genomic sequence to the Hu-1 (Wuhan) reference sequence, and would need to be in the stratosphere on the 40° N line above China in the period Oct-Dec 2019 to fit the known subsequent global spread and time lines. Simultaneous infection of multiple Chinese cities, with the biggest dose over Hubei/Wuhan, has also to be explained-does this imply multiple deliberate releases?
- How and where was the exact COVID-19 29,903 nt sequence made? Was it at the Wuhan Institute of Virology, or the National Institutes of Health (NIH), Bethesda Maryland, where Dr. Fauci’s group are based, and are known collaborators with the Wuhan laboratory (according to Tucker Carlson and many other news outlets). Furthermore, if the infection source was a product of a bioweapon development program, why was a common cold coronavirus chosen, which has such low mortality effects, causing death in <1% of the exposed population (with deficits in Type I and III Interferon responses [21-26]? One could claim that this was a “trial run”, but that also brings up the question (if this really does represent a trial bioweapon) how is it planned that the designers of this agent would be protected?
This short summary shows that Sharri Markson, Luc Montagnier, Wei Jingsheng, Nikolai Petrovsky and all the other writers elsewhere and at News Ltd on the influential The Australian newspaper in particular (Nick Cater, Adam Creighton, Paul Monk) have not thought through the implications of these proposals. There must be, as was the case with the 9/11 strike on the World Trade Centre, a significant amount of discoverable ‘human-factor’ associated-evidence behind this stratospherically launched viral attack over China and thus the world in Oct-Dec 2019, if there is any credibility to this theory-none has been reported. Scientific analyses of data and observations and building of explanatory models works in a different way. Science sticks to known facts, plausible mechanisms, with an absolute minimum number of useful assumptions, to explain the observed facts in a coherent way. As soon as the tested theory starts to flounder without the introduction of an ongoing series of ad hoc assumptions, the theory is abandoned and new, testable, hypothesis considered. Our published explanation has, to date, consistently explained the myriad of global data, without any need for further modification.
Current Myth#3
COVID-19 is a very severe respiratory disease resulting in death in many people.
All the current evidence strongly suggests that a very small immune defenceless group of patients lacking type I and type III interferon innate immunity responses are vulnerable and at high risk of death to COVID-19 infection [20-25]. In longitudinal studies these innate immune deficits are revealed, as expected, very early in infection in patients with a poor prognosis [24] (Figure 2c in that paper). Therapies to quell the respiratory crisis clearly need to be implemented very early in the infection in order to prevent life threatening pneumonia and other respiratory compromise. Included amongst such conventional therapies are pulse steroids (including prednisone; inhaled budesonide; dexamethasone) along with anti-viral agents (remdesivir) and other more novel immunobiologic interventions (monoclonal antibodies). Ivermectin therapy, although controversial, has also been suggested as a novel treatment [26]. What proportion of the population falls into the “immune defenceless elderly co-morbid group”? In surveying Cases and Deaths world-wide for some 18 months, and applying reasonable correction factors for the Numerator and Denominators in different countries and an assessment of the coverage and reliability of the tests and death outcomes in different countries and regions an estimate of 0.1% of all Covid-19 exposures appear to result in severe outcome, viz. death by COVID-19. A concrete example illustrates the calculation on data released on September 12 2021 at the NSW Dept Health Website, https://www.nsw.gov.au/covid-19/find-the-facts-about-covid-19#nsw-covid-19-datasets
For all COVID-19 Cases to date (for 2020 -21) there have been 41,999 confirmed cases of COVID-19 (severity has not been appended or made public here). There have been 14,701,732 PCR tests in a population of about 7 million over 2020 -21 to Sept 12 2021. The number of lives lost 2020-21 is 226. The great bulk of the deaths (as in Victoria in 2020 [9]) would occur in the ≥ 60 yr group (≥97%) or ≥ 70 yr group (≥94%). Clearly COVID-19 infection caused by any variant (raw meteorite dust or human passaged plume dust) causes high mortality in a very small vulnerable subset of the elderly population, as was evident in Wuhan in Jan 2020 and New York City (Mar-April 2020). What is this fraction? In NSW the Death rate is 0.54% on the above numbers, if you correct the Numerator (x2) and Denominator (divide by 2) for undetected cases and those dying with COVID-19 you arrive at a proportion close to the global estimate mentioned already of 0.1% deaths of all COVID-19 exposed cases in New South Wales in 2020-21. In the USA the correction to the Denominator is obligatory as in April-May 2020 the White House Chief Medical Advisor Dr Deborah Birx made it clear on several occasions in public that all deaths in COVID-19 positive patients would be scored as “COVID-19 deaths”. This has catastrophic consequences for an accurate appraisal of all the data coming out of the USA- the data, as presented, simply is not reliable, and needs to be corrected the way it has been done above. Indeed, the same erroneous calculation has almost certainly been going on all over the world – and is clearly also evident in public information released by the Victorian and New South Wales Departments of Health, their Chief Health Officers and their Health Ministers. viz a sensational headline of young people dying of COVID-19, only to be revealed later or fine print of the same report that many of the patients had very severe comorbidities (a curated and backed up digital file of most newspaper reports of this type in Australia 2020-21 has been maintained by the authors and the assertions can be backed up by news reports).
We posit the inescapable conclusion that the COVID-19 pandemic is a pandemic of a (slightly more severe?) common coronavirus (influenza-like) infection which >99% of people shrug off as they have throughout previous cold and flu outbreaks in past years. This has been dealt with in the past without widespread isolation, wearing of masks, and being locked at home with businesses and schools closed down. Indeed in past Influenza seasons the mortality rates in geriatric, aged care /nursing home facilities have often been higher during influenza epidemics (Table 1, summarised from Melbourne’s Herald-Sun p.32 29 August 2021). A comparison with influenza in Australia 2019 prior to COVID-19 shows that the seasonal influenza outbreaks in that year took a greater toll in cases and similar numbers in deaths. The numbers are biased because of the situation in Victoria [8]. There was massive political incompetence and chaos in Victoria in 2020 (and into 2021) – a reflection of the poor government and health system incompetence. Also, all the aged carers (usually Asian women with families to feed on poor wages) worked across multiple aged care and nursing homes and were very efficient viral vectors- a veritable bonfire of the nursing and aged care homes, almost simultaneous ignitions on scale. It was mainly caused by the single clone the L241f.1vic haplotype identified which the health authorities tracked and released genomic sequences of – although they did not release the genomes of the approx. 40% of mystery genome sequences (>3500) where it is hard not to see those infections not playing a role in the aged care and nursing homes. This is covered in detail [8].
Table 1: INFLUENZA v COVID-19: By the numbers.
Australian Influenza Cases in 2019
|
NSW |
112,841 |
| Vic |
66,015 |
|
Qld |
66,407 |
| WA |
22,720 |
|
SA |
22,754 |
| ACT |
3,952 |
|
TAS |
2,937 |
| NT |
1,458 |
Source: National Notifiable Diseases Surveillance System, Oct 2019.
Australian COVID-19 Cases in 2020-21
|
NSW |
20,466 |
| Vic |
21,618 |
|
Qld |
1,972 |
| WA |
1,064 |
|
SA |
870 |
| ACT |
300 |
|
TAS |
235 |
| NT |
201 |
Source: covid19data.com.au, 25 Aug 2021.
Australian Influenza Deaths in 2019
|
NSW |
334 |
| Vic |
138 |
|
Qld |
264 |
| WA |
80 |
|
SA |
119 |
| ACT |
10 |
|
TAS |
0 |
| NT |
5 |
Source: NSW Health, Victorian Influenza Snapshot, Qld Health, SA Health, ACT Health NT Health.
Australian COVID-19 Deaths in 2020-21
|
NSW |
129 |
| Vic |
820 |
|
Qld |
7 |
| WA |
9 |
|
SA |
4 |
| ACT |
3 |
|
TAS |
13 |
| NT |
0 |
Source: covid19data.com.au, 25 Aug 2021.
However, we have deduced, no real viral cloud in-fall occurred in the other Australian states. More than 95% of COVID-19 infections were in Victoria in 2020. The other states had mainly infected travellers from overseas or interstate from Victoria. Mystery infections in Victoria in 2020 were about 40% of all cases (often publicly confirmed as unlinked by genomic sequencing to known nursing home clusters) – these 3500-4000 genomes have yet to be released into the public scientific domain by the Peter Doherty Institute despite repeated requests in writing by the authors. Very few deaths this year so far in both Victoria and NSW, and mystery cases when reported are running at least at 50% of all PCR positive cases. All the details are not being released by the health authorities. It is conceivable that in 2021 lessons have indeed been learnt and aged care facilities may well be applying immediate therapies to the infected elderly to quell the respiratory crisis (and prevented employees working across multiple facilities). The infection flare-ups discussed below (Figure 3) appear now in large migrant 3-generation families under one roof in West-North suburbs of Melbourne (but same infection arc as 2020), and South-West arc of infections in Sydney, NSW.
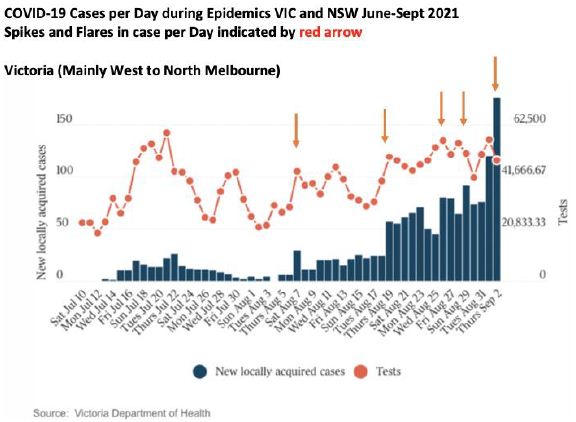
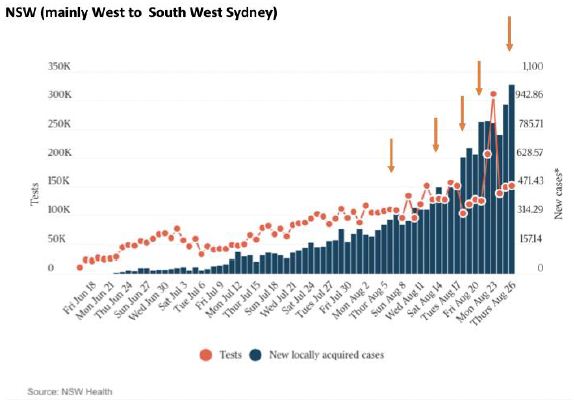
Figure 3: Cases per day plots in Victoria and NSW May-August 2021.
So COVID-19 is potentially dangerous for those with severe innate immune deficit in type I and III interferon responses [8] and references above. The target vulnerable group that requires special immediate therapeutic care are our elderly citizens in geriatric, aged care and nursing homes – as has always been the case in past cold and flu seasons in Australia. Indeed, in the early phases of this pandemic, the global argument for any restrictions (“lockdowns”) was to give time for health care systems everywhere to “get their ducks in order” so they were not overwhelmed and could be better prepared to deal with infections in those most at risk-that valid argument was rapidly forgotten, and people seemed to accept the early response strategy as a valid long-term one, without ever questioning why this viral infection should merit such long-term draconian responses. It is apparent with COVID-19 that elderly grandparents that still live with a wider three-generation family under one household roof are now especially vulnerable – as is typically the case for many recently arrived migrant families in the communities of western Sydney and western /northern Melbourne in Australia, in particular.
Current Myths#4
Nature of “Virulence’ with COVID-19? “Highly virulent rampaging and transmissible variants” (UK Mutant, South African mutant, Indian Delta etc).
Virulence is a term now widely and loosely used in the media and by political leaders and Chief Health Officers, without any good consensus as to its biologic meaning. In the current “Delta” outbreaks in Victoria and NSW the public is told that “Delta” seems to be “speeding through the community” indeed so fast it out runs the contact tracing teams, and it must therefore represent a highly virulent and transmissible variant, and thus a forebearer of a dangerous disease. When the sudden outbreaks in Shepparton, 190 km north of Melbourne began to appear from August 21 2021, one might have hoped for a pause for critical thinking by Victorian Premier Daniel Andrews and Chief Health Officer Brett Sutton. A “ring of steel” had been erected around Melbourne (from Aug 11) and hard stage 4 lock downs (and night curfews) had begun much earlier. This meant that no one from Melbourne could have travelled to/from Shepparton- and given the northern border with NSW was sealed (by police, army and drones) no one from the highly infected northern state of NSW could have come to Shepparton. We argue that only one infection route could and should have been considered……. “It must have come via an airborne route”. There is no public evidence that this explanation has been considered. At the time of preparing this paper, Sept 12-13 2021, the hard Stage 4 lockdown is still in place, cases per day are going up, 50-60% of all cases are genuine “mystery cases”, mandatory masks required inside and outside, QR tracking everywhere, hysterical headlines every day “to get tested” then “get jabbed”. Full night curfews are still in place. Only AFL Footballers (and NRL Footballers) seem to be able to move around. Many businesses have literally gone broke and many families will never recover. The number of bordered up businesses in the neighbourhood of EJS (Prahran, Toorak, Armadale, and South Yarra) is staggering. Long term social and health damage has been caused in Victoria, we are now in our 8th month of hard Stage 4 lock down.
However, we must be very clear, these lockdowns have had zero impact on the spread or apparent ‘virulence’ of the virus and course of the epidemics. The lockdown during the 2nd wave in Victoria in 2020 also had no effect, leaving us with the following conclusion [3]: “With respect to the symmetrical nature of the bell-shaped curves (Figure 4 below) describing the distributions of cases per day seen in such well documented epidemics such as the Victorian 2nd Wave an important deduction can be drawn about the impact of extreme ‘lockdown’ social distancing measures aimed at reducing viral reproduction rate Ro to less than 1. We have statistically analysed the Gaussian features of the Victorian 2nd Wave (which peaked on August 1-2, 2020). The best Gaussian fit with R2 gives 0.8999 which implies an almost perfect statistical fit to a symmetrical bell-shaped curve. Such a result would be consistent with the epidemic curve being overwhelmingly dominated by the growth and decay of a localised atmospheric in- fall event. The hard Stage 4 lockdown in Victoria came into effect on August 2, 2020. Given this perfect symmetry we conclude that the hard lock down measures had little impact, if any, on the course of the 2nd Wave COVID-19 epidemic in Victoria, Australia. This conclusion is consistent with the independent analyses of the impact of extreme lockdown measures on the course of the COVID-19 lockdowns introduced in a number of States in the USA during 2020 [27].”
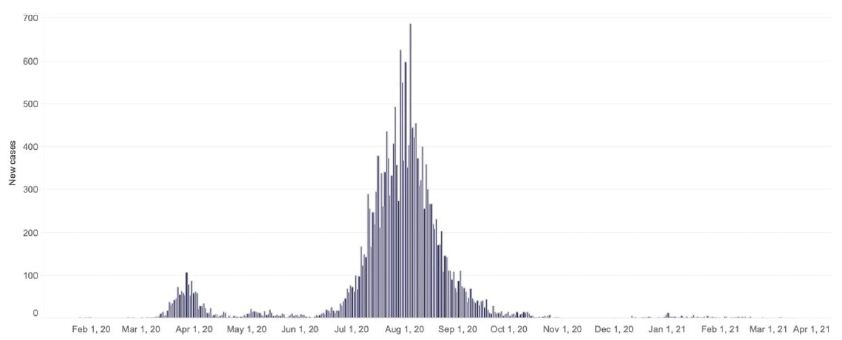
Figure 4: New SARS-CoV-2 cases per day recorded in Victoria, Australia, during 2020. These data can be accessed at https://www.dhhs.vic.gov.au/victorian-coronavirus-covid-19-data
Further Comment on COVID-19 Virulence
In our view the high virulence of a variant is an illusion caused by occurrence of multiple simultaneous ‘mystery cases’ occurring over a defined short time periods- a month or two via airborne region wide viral contamination. The impression of speed of transmission is created as unsuspecting victims catch CVOVID-19 via touching their contaminated environment. What then is the nature of the this suddenly emergent pandemic? Since COVID-19 first emerged in China in Dec 2019- Jan 2020 we have been trying to quell and eliminate a variant annual respiratory viral infection (similar to a common cold) – most (>99.9%) of all infected people handle the virus by Innate Immunity and Adaptive Immune Responses in the cells and tissues lining the mouth, nose, respiratory tract and lung- there is a vulnerable group about 0.1% of all infected people. The best response would have been to provide therapies and pro-active care of all Immune Defenceless Elderly Co-Morbid citizens through the respiratory crisis: Vulnerable age group for death by COVID-19 is ≥ 70 yrs and median is somewhere around 80-90 yr. COVID-19 is therefore basically a common seasonal respiratory virus, but if there is an Innate Immune Deficit that would result in uncontrolled replication and potential pneumonia [8].
Another Media Claim: Rampaging Virulent Variants?
Answer: No it just appears that way.
According to the main stream media and political leaders the human passaged COVID-19 variants currently engaging Australia and Northern Hemisphere infected zones (2021) such as the UK Mutant (alpha’), Indian Plume Mutants (‘Delta’, Kappa’) are apparently highly rampaging and virulent transmissible variants. This is not true. They have been spread and globally transported as viral-dust clouds first by prevailing tropospheric winds from the plumes of human passaged viral aerosols that arose in the original host country, and were then brought to ground by precipitation (rain) in defined regions. Figure 1 is illustrative: In Australia the prevailing weather systems have struck repeatedly in Victoria (South West-West- North arc of Melbourne into Northern regions (Shepparton, and maybe also further north east to ACT). The East of the State of Victoria has been virus free, 2020, 2021; in Sydney, NSW a similar defined arc Bondi-South West-West Sydney suburbs in 2021. Thus a viral-laden contaminated environment causing large numbers of effectively (in time) simultaneous “mystery cases “of community transmissions i.e. the variant(s) only appear as “Rampaging Virulent variants”.
However, they are dangerous in geriatric, aged care/nursing homes and in large three generation migrant families viz. closed clusters of Immune Defenceless elderly Co-morbid communities, where massive viral amplifications to trillions of virions contaminating all peoples and fomite surfaces in immediate environment. Thus carers, medical staff, family members and close associate who then all develop a flu-like illness (due to sheer viral dose loads at infection) are at risk of infection and likely to become PCR Positive. These are the ramping flare-ups in PCR Positive numbers per Day often seen in the published Cases Per Day Plots in both Victoria and NSW in 2021 (Figure 4) – and in the Victorian 2nd wave in 2020 (Figure 2). These striking features are NOT being discussed or mentioned in the mainstream media or press conferences. Such patients will be High PCR cycle number positives (i.e. very low numbers of virus or viral fragments in oral-nasal swab); and the primary infected amplifying elderly patients are expected to be very low PCR cycle number positive cases.
The other evidence against is that the “ UK Mutant” entered Australia by jet plane in Jan-Feb 2021 at multiple portals of entry (Perth, Adelaide, Brisbane, Melbourne etc) and also dispersed contacts to regional cities in Australia, with large numbers (hundreds) of putative contacts- hotel cleaners, drivers, departure and arrival lounges, trains, buses, kiosk workers at food counters, taxis etc: The UK mutant DID NOT spread person-to-person in Australia (but may well have amplified in communities of Immune Defenceless Elderly co-morbids if such an entry had happened, but it did not. So again the group that should be monitored and cared for are our elderly citizens. As we have discussed [8] these negative transmission data led the Australian epidemiologist at The Australian National University, Professor Peter Collignon, to release his considered opinion to The Australian newspaper [28]: “…In retrospect, the Melbourne lockdown was unnecessary… From my perspective, if you’ve got very little community transmission, I’m not sure that a short lockdown achieves much extra, if you’ve got good contact tracing and good testing,” he said. … “If I look at the lockdowns done in Adelaide, Brisbane, Perth, and now Melbourne, it didn’t turn up one more case than contact tracing did. … “The UK strain has not spread uncontrollably and wildly.” Further research is required to understand why the putative highly virulent “UK Mutant” did not spread when introduced via multiple entry points into Australia in the first few months of 2021.
Current Myths#5
Efficacy of current Jab in the Arm vaccines?
We have discussed [8, 29] why all “Jab in the Arm” vaccines, whilst stimulating systemic immunity in the blood stream (IgG and IgM complement fixing and other classes of serum antibodies and later potentially enduring cytotoxic T lymphocyte adaptive immunity) may not be the best antigen-delivery route for activating enduring mucosal immunity (non-complement fixing yet very avid neutralising secretory IgA including mucosal adaptive T cell responses). This can be expected based simply on current textbook knowledge and past experimental experiences. This explains why many examples are now emerging of a failure of twice vaccinated individuals to be protected against catching COVID-19 e.g. many high profile politicians, sportsmen, whole US baseball teams travelling on the road, and of course the current wide-spread infections in the State of Israel despite most of the population being double vaccinated. Further, the phenomenon of antibody dependent enhancement (ADE) means that such individuals are at additional risk to formation of complement fixing antigen-antibody complexes in lung capillary airways if they become subsequently COVID-19 infected compounding the severity of the pathogenic cytokine storms [30]. This unintended adverse consequence has been discussed at length by Professor Dolores Cahill in a recent May 21 2021 interview [31]. Indeed apart from all the other deep and genuine concerns widely held by scientists and in the community about the safety and adverse affects of these novel engineered mRNA expression vector vaccines [31], it is clear also to us, that the vaccine roll out has played little if any role at all in the clear decline of the severity of the pandemic in Northern Hemisphere infected zones [32]. Thus in exemplar countries, with a substantial vaccine roll out at time of writing, Sweden, Denmark, Netherlands, United Kingdom, France, Germany, Italy, and Israel it is clear the decline in respiratory disease severity as assessed by the metric “% COVIDI-19 associated Death” was well advanced and effectively over before the vaccine roll out began (Figure 5 for Denmark).
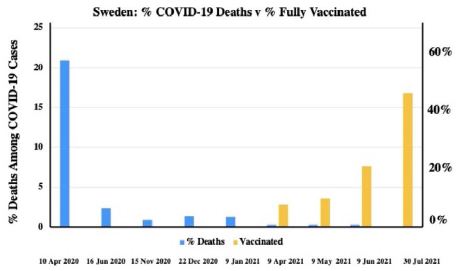
Figure 5: Percent Deaths Among COVID-19 cases versus the timing of the Vaccination roll out (% population vaccinated) in Denmark.
In the case of Denmark there is clear supportive independent evidence that natural herd immunity induced by prior oral-nasal infections throughout 2020 prior to the vaccine roll out was the clear cause of the type of decline in COVID case severity curve typical of many countries in Figure 5. Thus, to directly quote from [8]: “Natural infections with SARS-CoV-2 (in recovered patients) would therefore be expected to induce protective dimeric sIgA mucosal immunity. Certainly the recent longitudinal population scale study in Denmark implies that prior infection with SARS-CoV-2 affords upwards of 80% protection in the population under 65yr against reinfection between the first and second major surges of SARS-CoV-2 in Denmark in 2020; with the protective rate in the re-infected elderly vulnerable group a half lower again at 47% [33]. These are encouraging findings suggesting, at the time of writing, that natural ‘herd immunity’ could be well underway in Denmark and similar Northern hemisphere infected zones in 2020 and into likely surges and waves of SARS-CoV-2 in 2021.” There is also reason to believe, given the failure of a typical ‘virulent’ mutant (UK Mutant) to spread widely and quickly by P-to-P spread in Australia that the human passaged variants are attenuating- typical during decline phases of all epidemics as the host v parasite interaction tempers the replicative efficacy of the pathogen.
Our Recommendations
Given that all the fundamental assumptions of all governments and all their chief health advisors and epidemiologists have been wrong about every aspect of the COVID-19 pandemic – from its origin, its global mode of spread and the best way to medically treat and induce vaccine-immunity against oral-nasal acquired cold and flu infection, we recommend the following:
- All lockdown measures to stop P-to-P be immediately lifted viz. social distancing, mask wearing, curfews, crowd controls, border closures, restrictions on business operations, school closures, church closures, sporting club closures, fitness centre closures etc.
- Abolish vaccination rollouts and stop vaccine mandates and passports: All government (and main stream media) propaganda about vaccines protecting individuals needs to cease; all vaccine mandates of all types cease (for work, business trading, travel domestic and international) be lifted.
- All State and International borders be immediately opened.
- Immediate financial compensation scheme by the Federal Government to help all Australian citizens affected by any of these clearly erroneous and wrong emergency power laws especially small business owners.
- An apology is in order for wrongful actions that have caused harm. From: Governments and their Chief Health Officers and associated organisations that implemented all lockdown and vaccine procedures. In Australia, The Therapeutic Goods Administration (TGA) including major scientific organisations that actually gave a scientific blessing to the Federal and State Governments justifying their actions (The Peter Doherty Institute, The Australian Academy of Science) all need to apologise.
As we have suggested on numerous occasions the world needs to accept that suddenly emerging diseases from space have been a regular feature of our history and the evolution of life on Earth. Thus, the need for early warning surveillance, via orbiting satellite platforms and sampling the meteorite and cosmic dust on the external surface of the International Space Station. This would seem a logical step now for mankind to take as a unified collective. Since many suddenly emergent pandemic diseases are often cold or flu viruses that target the respiratory tract it would be sensible to design all such future vaccines to mimic the natural infection portal of entry via nose and mouth. Vaccines designed to be delivered via the oral-nasal route would certainly induce acquired mucosal secretory IgA immunity which is the most likely population-wide identifiable immune factors responsible the currently observed population-scale ‘Herd Immunity’ [32,33].
References
- Wickramasinghe NC, Steele EJ, Gorczynski RM, Temple R, Tokoro G, et al. (2020) Predicting the Future Trajectory of COVID-19. Virology: Current Research 4:1. https://www.hilarispublisher.com/open-access/predicting-the-future-trajectory-of-covid19-44601.html
- Wickramasinghe NC, Wallis MK, Coulson SG, Kondakov A, Steele EJ, et al. (2020) Intercontinental Spread of COVID-19 on Global Wind Systems. Virology: Current Research 4:1. https://www.hilarispublisher.com/open-access/intercontinental-spread-of-covid19-on-global-wind-systems-45198.html
- Steele EJ, Gorczynski RM, Lindley RA, Tokoro G, Wallis DH, et al. (2021) Cometary Origin of COVID-19 (2021) Infect Dis Ther 2:1-4. https://researchopenworld.com/cometary-origin-of-covid-19/
- Steele EJ, Gorczynski RM, Carnegie P, Tokoro G, Wallis DH, et al. (2021) COVID-19 Sudden Outbreak of Mystery Case Transmissions in Victoria, Australia, May-June 2021: Strong Evidence of Tropospheric Transport of Human Passaged Infective Virions from the Indian Epidemic. Infect Dis Ther 2:1-28. https://researchopenworld.com/covid-19-sudden-outbreak-of-mystery-case-transmissions-in-victoria-australia-may-june-2021-strong-evidence-of-tropospheric-transport-of-human-passaged-infective-virions-from-the-indian-epidemic/
- Howard GA, Wickramasinghe NC, Rebhan H, Steele EJ, Gorczynski RM, et al. (2020) Mid-Ocean Outbreaks of COVID-19 with Tell-Tale Signs of Aerial Incidence Virology: Current Research 4:2. https://www.hilarispublisher.com/open-access/midocean-outbreaks-of-covid19-with-telltale-signs-of-aerial-incidence.pdf
- Steele EJ, Gorczynski RM, Rebhan H, Carnegie P, Temple R, et al. (2020) Implications of haplotype switching for the origin and global spread of COVID-19. Virology: Current Research 4:2. https://www.hilarispublisher.com/open-access/implications-of-haplotype-switching-for-the-origin-and-global-spread-of-covid19.pdf
- Wickramasinghe NC, Steele EJ, Nimalasuriya A, Gorczynki RM, Tokoro G, et al. (2020) Seasonality of Respiratory Viruses Including SARS-CoV-2. Virology: Current Research 4:2. https://www.hilarispublisher.com/open-access/seasonality-of-respiratory-viruses-including-sarscov2-51923.html
- Lindley RA, Steele EJ (2021) Analysis of SARS-CoV-2 haplotypes and genomic sequences during 2020 in Victoria, Australia, in the context of putative deficits in innate immune deaminase anti-viral responses. Scand J Immunol. 00:e13100 https://doi.org/10.1111/sji.13100
- Steele EJ, Lindley RA (2020) Analysis of APOBEC and ADAR deaminase-driven Riboswitch Haplotypes in COVID-19 RNA strain variants and the implications for vaccine design. Research Reports. doi:10.9777/rr.2020.10001 https://companyofscientists.com/index.php/rr.
- Pekar J, Worobey M, Moshiri N, Scheffler K, Wertheim JO (2021) Timing the SARS-CoV-2 index case in Hubei province. Science 372: 412-417. [crossref]
- Steele EJ, Gorczynski RM, Lindley RA, Tokoro G, Temple R, et al. (2020) Origin of new emergent Coronavirus and Candida fungal diseases-Terrestrial or Cosmic? Advances in Genetics 106: 75-100. https://doi.org/10.1016/bs.adgen.2020.04.002
- Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan. Lancet 395: 497-506. [crossref]
- Cohen, J (2020) Wuhan seafood market may not be source of novel virus spreading globally. Science https://www.sciencemag.org/news/2020/01/wuhan-seafood-market-may-not-be-source-novel-virus-spreading-globally
- Luc Montagnier Gilmore Health https://www.gilmorehealth.com/chinese-coronavirus-is-a-man-made-virus-according-to-luc-montagnier-the-man-who-discovered-hiv/
- Wickramasinghe NC, Steele EJ, Gorczynski RM, Temple R, Tokoro G, et al. (2020) Comments on the Origin and Spread of the 2019 Coronavirus. Virology: Current Research 4: 1. https://www.hilarispublisher.com/open-access/comments-on-the-origin-and-spread-of-the-2019-coronavirus-33365.html
- Wickramasinghe NC, Steele EJ, Gorczynski RM, Temple R, Tokoro G, et al. (2020) Growing Evidence against Global Infection-Driven by Person-to-Person Transfer of COVID-19. Virology Current Research 4: 1. https://www.hilarispublisher.com/open-access/growing-evidence-against-global-infectiondriven-by-persontoperson-transfer-of-covid19.pdf
- Hoyle F, Wickramasinghe NC (1979) Diseases from Space JM Dent & Son London
- Steele EJ, Al Mufti S, Augustyn KA, Chandrajith R, Coghlan JP, et al (2018) Causes of Cambrian Explosion-Terrestrial or Cosmic? Biophys Mol Biol 136: 3-23. [crossref] https://doi.org/10.1016/j.pbiomolbio.2018.03.004
- Steele EJ, Gorczyski RM, Lindley RA, Liu Y, Temple R, et al (2019 ) Lamarck and Panspermia-On the efficient spread of living systems throughout the cosmos. Prog Biophys. Mol. Biol. 149: 10-32. [crossref] https://doi.org/10.1016/j.pbiomolbio.2019.08.010
- Acharya D, Liu G, Gack MU (2020) Dysregulation of type I interferon responses in COVID-19 Rev. Immunol 20: 397–98. [crossref]
- Blanco-Melo D, Nilsson-Payant BE, Liu WC, Uhl S, Hoagland D, et al. (2020) Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 181: 1036-1045. [crossref]
- Hadjadj J, Yatim N, Barnabei L, Corneau A, Boussier J, et al. (2020) Impaired type I interferon activity and exacerbated inflammatory responses in severe Covid-19 patients. Science 369: 718-724. [crossref]
- Sette A, Crotty S (2021) Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 184: 861-880. [crossref]
- Lucas C, Wong P, Klein J, Castro TBR, Silva J, et al. (2020) Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature 584: 463-469. [crossref]
- Zhang Q, Bastard P, Liu Z, Le Pen J, Moncada-Velez M, et al. (2020) Inborn errors of type I IFN immunity in patients with life-threatening COVID-19. Science 370: eabd4570. [crossref]
- Bryant A, Lawrie TA, Dowswell T, Fordham EJ, Mitchell S, et al. (2021) Ivermectin for Prevention and Treatment of COVID-19 Infection: A Systematic Review, Meta-analysis, and Trial Sequential Analysis to Inform Clinical Guidelines. American Journal of Therapeutics 28: e434–e460. [crossref]
- Luskin DL (2020) The failed experiment of COVID-19 lockdowns. The Wall Street Journal. https://www.wsj.com/articles/the-failed-experiment-of-covid-lockdowns-11599000890
- Baxendale R, Robinson N (2021) Spread of UK coronavirus variant limited to close contacts. The Australian.
- Gorczynski RM, Lindley RA, Steele EJ, Wickramasinghe NC. 2021 Nature of acquired immune responses, epitope specificity and resultant protection from SARS-CoV-2. Under submission
- Lee WS, Wheatley AK, Kent SJ, DeKosky BJ (2020) Antibody-dependent enhancement and SARS-CoV-2 vaccines and therapies. Microbiol 5: 1185-1191. https://www.nature.com/articles/s41564-020-00789-5
- Professor Dolores Cahill in a recent May 21 2021 interview on Asia Pacific Today: https://rumble.com/vjhasl-professor-dolores-cahill-says-the-mrna-vaccines-cause-injury-and-death..html
- Steele EJ, Gorczynski RM, Lindley RA, Tokoro G, Wallis DH, et al. (2021) An End of the COVID-19 Pandemic in Sight? Infectious Diseases and Therapeutics 2: 1-5. https://researchopenworld.com/an-end-of-the-covid-19-pandemic-in-sight/
- Hansen CH, Michlmayr D, Gubbels SM, Mølbak K, Ethelberg S (2021) Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: a population-level observational study. The Lancet 397: 1204-1212.