DOI: 10.31038/CST.2017251
Abstract
Investigations in immunomodulating therapies for cancer treatment over the past 20 years have flourished. Given the complex tumor microenvironment and differential signaling pathways a wide variety of potential targeting mechanisms have come to attention. Herein we review the immunomodulating potential of Chemokine 21 in pre-clinical and clinical studies, as well as examine the novel multi-faceted immune-based treatments in advanced head and neck cancer.
Introduction
Head and neck squamous cell carcinoma (HNSCC) is the sixth most common cancer in the world, accounting for more than 300,000 deaths annually [1]. Despite advances in surgical techniques and chemo-/radiation treatment strategies, patients with advanced T3 or T4 HNSCC continue to demonstrate 20%-30% survival with failure of primary surgical or medical (radiation and chemotherapy) management. Salvage therapies, in recalcitrant or recurrent disease, are limited by systemic toxicity or operative morbidity owing to nearby vital structures (carotid artery, skull base). Immunotherapy and modulation in HNSCC is a promising venture given recent advances in cancer biology and investigations in the tumor microenvironment.
Historically studied in the contexts of inflammation and immune response, chemokines have increasingly been studied in the context of tumor proliferation [2, 3]. Chemokines are a family of small chemotactic cytokines involved in cellular signaling and inflammation. Through interactions within a subset of G-protein- coupled transmembrane receptors (GPCRs), secreted cellular chemokines regulate cellular homing, activation, and recruitment of a variety of diverse leukocytes and activated adhesion molecules [2, 4-6]. In the tumor microenvironment, responses to specific chemokines result in the migration of different immune cell subsets and regulate tumor immune responses; these are both pro- and anti- inflammatory in nature. Chemokines, have been directly associated with cancer immunity, proliferation, and metastases [7,8]. In this review, we address the role of Chemokine 21 (CCL-21) in tumor progression, its role as an immunotherapy platform, and the potential within head and neck oncology.
CCL-21 chemotaxis and lymphocyte recruitment
Divided into four subfamilies, chemokine nomenclature is related to the location of their first N-terminal cysteine (C) residues; classified as: C-, CC-, CXC-, and CX3C-chemokines [9]. CCL-21 (also known as Thymus-derived chemokine 4, 6Ckine, or Exodus-2) is a CC chemokine expressed in high endothelial post-capillary venules, T-cell stromal zones of the spleen, Peyer’s patches, and afferent peripheral lymph nodes that strongly attracts naïve T-cells and mature dendritic cells (DC) including NK T-cells [10-13]. The effects of CCL-21 on chemotaxis have been demonstrated in neutralization studies, where the homing of T-cells and DCs has been shown to be significantly reduced [14, 15]. Acting through the GPCR CCR7, a convergence of the immune response elements to sites of CCL-21 production have been demonstrated to co-stimulate the expansion of CD4+ and CD8+ T cells and induce Th1 polarization [16]. Additionally, chemokine bound DCs form T cell adhesions resulting in a hyper-responsive T-cell on subsequent exposure to CCL-21 and antigen-presenting cells [17].
Role in cancer immunotherapy
The cancer immunosuppressant microenvironment results in ineffective antigen processing and presentation; resulting in poor host response. The CCL-21/CCR-7 axis has been studied in efforts to create a more immunogenic environment through chemotaxis of DCs, NK cells, and lymphocytes. By recruiting host antigen presenting cells (APC) for tumor antigen presentation, T cells within lymphoid organs have the ability to prime anti-tumor specific activity. Of note, while CCL-21 aids in the polarization of Th1 lymphocytes, the secondary lymphoid chemokine has also been shown to have minimal effect on the proliferation of suppressor cell population; CD4+CD25+ T-regulatory cells are hypo responsive to CCL-21 induced migration and unresponsive to CCL-21 co-stimulation [16]. High levels of T-regulatory cells within the tumor microenvironment has demonstrated poor prognosis in many cancers, dependent on the type and location of neoplasm [18].
Pre-clinical animal models
The ability to process and present a high ratio of activated tumor-antigen-APCs has long been the goal of immunotherapy in the immunosuppressive cancer microenvironment. The first established model for the creation of a CCL-21 chemotactic gradient in restoring tumor-antigen presentation was undertaken by Sharma and Dubinett [19]. In an immune competent murine lung cancer model, intratumoral injection of CCL21 induced infiltration of CD4+ and CD8+ T cells and DC in both tumor and draining lymph nodes. Additionally, a potent antitumor response was observed as complete tumor eradication was found in 40% of treated mice [19]. Furthermore, the tumor microenvironment displayed a concomitant decrease in immunosuppressive molecules such as PGE-2 and TGF-ß [19]. When introduced to the afferent axillary lymph nodes, CCL-21 injections resulted in a marked infiltration of lymphocytes and DCs into the lung tumor microenvironment, associated with a significant reduction in tumor burden [20]. The anti-tumor efficacy of CCL-21 has further been confirmed in a variety of transgenic lung, ovarian, melanoma, and liver cancer models [21-25]. Despite the promising results, in vivo studies have utilized specific cancer cell lines, with greater success observed in low-malignant weakly metastatic clones as compared to highly-metastatic clones [26]. Further research on the efficacy within specific tumor phenotypes, locations, timing, and dosing of CCL-21 continues to be underway.
Antigen presenting cells as a platform
APCs are fundamental in the activation of specific immunity and have been investigated as adjuvants to cancer immunotherapy to stimulate tumor-specific antigen presentation for promotion of T cell activation and anti-cancer immunity [27, 28]. Prior investigations have generated DCs with enhanced immune stimulatory and T-cell activity through pulsed electroporation of antigens or viral transduction of cytokines [29-33].
A platform to transduce DCs with CCL-21 (DC-CCL21) through an adenovirus vector has also recently been developed demonstrating viable in vitro chemotaxis of activated lymphocytes [34, 35]. The anti- tumor efficacy of DC-CCL21 has been studied in the murine lung and melanoma cancer models. These studies demonstrated a significant reduction in melanoma tumor growth and complete eradication of lung tumor burden in 60% of mice with lung cancer [32, 34]. Clinical trials are currently underway in late stage non-small cell lung cancer patients based on the promising results of this preclinical data [36].
Head and neck oncology
Recurrent and advanced HNSCC has been extraordinarily challenging to treat, with stagnant survival and cure rates over the past 20 years [37]. Depending on the tumor site, reoccurrence rates may range from 25%-50%, and the incidence of subsequent reoccurrences similarly fall within this broad range [38-40]. Morbidity from current salvage treatment strategies are unfortunately common and include chronic pain, respiratory distress, and dysphagia oftentimes resulting in tracheotomy, or, gastrostomy tube dependence [41]. Despite cancer outcomes, cosmetic and functional deficits may negatively impact the head and neck cancer patient’s quality of life [42-44]. Limited surgically by nearby structures and systemically by toxic effects, advancements in locoregional therapies in the tumor microenvironment are strongly desired.
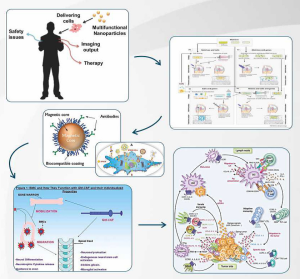
Recent advances in material science, have developed biocompatible, functional, three dimensional polymer systems for molecular and cellular delivery in cancer care [45]. A novel implantable polymer- based system for the delivery of chemokines to interact directly with tumor cells, has the potential to integrate with a wide range of anti- cancer treatments. Recently, a biodegradable poly-ε-caprolactone (PCL), polylactide-co-glycolide (PLG), co-polymer seeded with DC- CCL21 and/or cisplatin has been tested in an animal model resembling unresectable head and neck squamous cell carcinoma (HNSCC) [46, 47]. Tumor cells from the squamous cell carcinoma (SCCA) VII/ SF were injected, grown, and debulked in the flanks of C3H/HeJ mice. The animals then underwent debulking surgery to replicate an unresectable cancer setting. The flexible seeded PCL/PLCL polymer was then applied to contour the cancer tissue bed. In the first study, the cisplatin-polymer group effectively reduced tumor volume by over 16-fold when compared to control polymer with intratumoral cisplatin injection groups [47]. When combined with radiation, the cisplastin-seeded polymer group enhanced the efficacy of radiation therapy by tumor volume reductions of 53% when compared to surgery and radiation alonel [47]. Given the well-established literature in the role of cytokines in tumor regression, the HNSCC murine polymer model was then seeded with DC-CCL21 using a fibrin gel delivery mechanism. After implantation to the partially resected tumor, DC-CCL21 secreting polymer significantly reduced SCC VII/ SF tumors by 41% as compared to control groups [46]. Additionally, the DC-CCL21 polymer resulted in increased CD4+ and CD11+ DCs as well as a marked decrease in T-regulatory cells within the tumor microenvironment.
Current studies are underway to assess the anti-tumor efficacy of DC-CCL21 with combination of cisplatin and radiation therapy in the HNSCC murine model. Additionally, the promising findings of APC and T cell recruitment provide the rationale for combination with immune checkpoint blockade therapy to enhance the frequency of activated T cells in the tumor micro-environment for improved patient outcome.
Conclusion
Research in the field of immunology has evolved tremendously as the complex immunosuppressive tumor microenvironment continues to unravel. The role of CCL-21 is critical in promoting DC homing and T-lymphocyte activation. Tumor antigen presentation is significantly amplified both locally and peripherally following introduction of CCL-21. Head and neck cancer therapies, previously limited by morbidity,
may now have an alternative for locoregional control in unresectable tumors. A multi-faceted approach to innovative cancer treatment is necessary in order to maximize the immunogenic potential for tumor cell death. As described, it is clear that CCL-21 is a potent chemokine in eliciting an immune response with substantial evidence supporting its use in future oncologic therapies. Collaborations with materials scientists, immunologists, and physicians can not be underestimated in the ongoing pursuit for cancer cure.
References
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, et al. (2010) Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127: 2893–2917. [crossref]
- Zlotnik A, Yoshie O (2000) Chemokines Immunity 12: 121–127.
- Nagarsheth N, Wicha MS, et al. (2017) Chemokines in the cancer microenvironment and their relevance in cancer immunotherapy. Nat Rev Immunol 17: 559–572. [crossref]
- Luster AD, Chemokines — Chemotactic Cytokines That Mediate Inflammation. Epstein FH, ed. N Engl J Med 338: 436–445.
- Stoolman LM (1989) Adhesion molecules controlling lymphocyte migration. Cell 56: 907–910. [crossref]
- Elices MJ, Osborn L, Takada Y, et al. (1990) VCAM-1 on activated endothelium interacts with the leukocyte integrin VLA-4 at a site distinct from the VLA-4/ Fibronectin binding site. Cell 60: 577–584.
- Zou W, Chen L (2008) Inhibitory B7-family molecules in the tumour microenvironment. Nat Rev Immunol 8: 467–477. [crossref]
- Zou W (2006) Regulatory T cells, tumour immunity and immunotherapy. Nat Rev Immunol 6: 295–307. [crossref]
- Zou W (2005) Immunosuppressive networks in the tumour environment and their therapeutic relevance. Nat Rev Cancer 5: 263–274.
- Willimann K, Legler DF, Loetscher M, et al. (1998) The chemokine SLC is expressed in T cell areas of lymph nodes and mucosal lymphoid tissues and attracts activated T cells via CCR7. Eur J Immunol 28: 2025–2034.
- Nagira M, Imai T, Hieshima K, et al. (1997) Molecular cloning of a novel human CC chemokine secondary lymphoid-tissue chemokine that is a potent chemoattractant for lymphocytes and mapped to chromosome 9p13. J Biol Chem 272: 19518–19524.
- Hromas R, Kim CH, Klemsz M, et al. (1997) Isolation and characterization of Exodus-2, a novel C-C chemokine with a unique 37-amino acid carboxyl-terminal extension. J Immunol 159: 2554–2558.
- Hedrick JA, Zlotnik A (1997) Identification and characterization of a novel beta chemokine containing six conserved cysteines. J Immunol 159: 1589–1593.
- Cyster JG (1999) Chemokines and the homing of dendritic cells to the T cell areas of lymphoid organs. J Exp Med 189: 447–450.
- Gunn MD, Kyuwa S, Tam C, et al. (2010) Mice lacking expression of secondary lymphoid organ chemokine have defects in lymphocyte homing and dendritic cell localization. J Exp Med 189: 451–460.
- Flanagan K, Moroziewicz D, Kwak H, Hörig H, Kaufman HL (2004) The lymphoid chemokine CCL21 costimulates naive T cell expansion and Th1 polarization of non-regulatory CD4+ T cells. Cell Immunol 231: 75–84. [crossref]
- Friedman RS, Jacobelli J, Krummel MF (2006) Surface-bound chemokines capture and prime T cells for synapse formation. Nat Immunol 7: 1101–1108. [crossref]
- Oleinika K, Nibbs RJ, Graham GJ, Fraser AR (2013) Suppression, subversion and escape: the role of regulatory T cells in cancer progression. Clin Exp Immunol 171: 36–45.
- Sharma S, Stolina M, Luo J, et al. (2000) Secondary Lymphoid Tissue Chemokine Mediates T Cell-Dependent Antitumor Responses In Vivo. J Immunol 164: 4558–4563.
- Sharma S, Stolina M, Zhu L, et al. (2001) Secondary lymphoid organ chemokine reduces pulmonary tumor burden in spontaneous murine bronchoalveolar cell carcinoma. Cancer Res 61: 6406–6412.
- Kar UK, Srivastava MK, Andersson A, Baratelli F, Huang M, et al. (2011) Novel CCL21-vault nanocapsule intratumoral delivery inhibits lung cancer growth. PLoS One 6: e18758. [crossref]
- Nomura T, Hasegawa H, Kohno M, Sasaki M, Fujita S (2001) Enhancement of anti-tumor immunity by tumor cells transfected with the secondary lymphoid tissue chemokine EBI-1-ligand chemokine and stromal cell-derived factor-1alpha chemokine genes. Int J cancer 91: 597–606.
- Novak L, Igoucheva O, Cho S, Alexeev V (2007) Characterization of the CCL21- mediated melanoma-specific immune responses and in situ melanoma eradication. Mol Cancer Ther 6: 1755–1764.
- Briles EB, Kornfeld S (1978) Isolation and metastatic properties of detachment variants of B16 melanoma cells. J Natl Cancer Inst 60: 1217–1222.
- Liang C, Zhong C, Sun R, et al. (2007) Local expression of secondary lymphoid tissue chemokine delivered by adeno-associated virus within the tumor bed stimulates strong anti-liver tumor immunity. J Virol 81: 9502–9511.
- Shields JD, Kourtis IC, Tomei AA, Roberts JM, Swartz MA (2010) Induction of lymphoidlike stroma and immune escape by tumors that express the chemokine CCL21. Science 328: 749–752. [crossref]
- Steinman RM (1991) The dendritic cell system and its role in immunogenicity. Annu Rev Immunol 9: 271–296. [crossref]
- Steinman RM (1996) Dendritic cells and immune-based therapies. Exp Hematol 24: 859–862.
- Wilgenhof S, Van Nuffel AMT, Benteyn D, et al. A phase IB study on intravenous synthetic mRNA electroporated dendritic cell immunotherapy in pretreated advanced melanoma patients. Ann Oncol Off J Eur Soc Med Oncol 24: 2686–2693.
- Van Nuffel AMT, Benteyn D, Wilgenhof S, et al. (2012) Dendritic cells loaded with mRNA encoding full-length tumor antigens prime CD4+ and CD8+ T cells in melanoma patients. Mol Ther 20: 1063–1074.
- Miller PW, Sharma S, Stolina M, et al. (2000) Intratumoral administration of adenoviral interleukin 7 gene-modified dendritic cells augments specific antitumor immunity and achieves tumor eradication. Hum Gene Ther 11: 53–65.
- Yang S, Hillinger S, Riedl K, et al. (2004) Intratumoral Administration of Dendritic Cells Overexpressing CCL21 Generates Systemic Antitumor Responses and Confers Tumor Immunity Intratumoral Administration of Dendritic Cells Overexpressing CCL21 Generates Systemic Antitumor Responses and Confers Tu 10: 2891–2901.
- Sharma S, Batra RK, Yang SC, et al. (2003) Interleukin-7 gene-modified dendritic cells reduce pulmonary tumor burden in spontaneous murine bronchoalveolar cell carcinoma. Hum Gene Ther 14: 1511–1524.
- Kirk CJ, Hartigan-O’Connor D, Nickoloff BJ, et al. (2001) T cell-dependent antitumor immunity mediated by secondary lymphoid tissue chemokine: augmentation of dendritic cell-based immunotherapy. Cancer Res 61: 2062–2070.
- Riedl K, Baratelli F, Batra RK, et al. (2003) Overexpression of CCL-21/secondary lymphoid tissue chemokine in human dendritic cells augments chemotactic activities for lymphocytes and antigen presenting cells. Mol Cancer 2: 35.
- Sharma S, Zhu L, Srivastava MK, et al. (2013) CCL21 Chemokine Therapy for Lung Cancer. Int Trends Immun 1: 10–15.
- Goodwin WJ (2000) Salvage surgery for patients with recurrent squamous cell carcinoma of the upper aerodigestive tract: when do the ends justify the means? Laryngoscope 110(3 Pt 2 Suppl 93): 1–18.
- Bernier J, Domenge C, Ozsahin M, et al. (2004) Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 350: 1945–1952.
- Cooper JS, Pajak TF, Forastiere AA, et al. (2004) Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 350: 1937–1944.
- Agra IM, Carvalho AL, Ulbrich FS, de Campos OD, Martins EP, et al. (2006) Prognostic factors in salvage surgery for recurrent oral and oropharyngeal cancer. Head Neck 28: 107–113. [crossref]
- Argiris A, Karamouzis MV, Raben D, Ferris RL (2008) Head and neck cancer. Lancet 371: 1695–1709. [crossref]
- Ho AS, Kraus DH, Ganly I, Lee NY, Shah JP, et al. (2014) Decision making in the management of recurrent head and neck cancer. Head Neck 36: 144–151. [crossref]
- Rathod S, Livergant J, Klein J, Witterick I, Ringash J (2015) A systematic review of quality of life in head and neck cancer treated with surgery with or without adjuvant treatment. Oral Oncol 51: 888–900.
- Ko C, Citrin D (2009) Radiotherapy for the management of locally advanced squamous cell carcinoma of the head and neck. Oral Dis 15: 121–132. [crossref]
- Shikani AH, Domb AJ (2000) Polymer chemotherapy for head and neck cancer. Laryngoscope 110: 907–917. [crossref]
- Lin Y, Luo J, Zhu WE, et al. (2014) A Cytokine-Delivering Polymer Is Effective in Reducing Tumor Burden in a Head and Neck Squamous Cell Carcinoma Murine Model. Otolaryngol Neck Surg 151: 447–453.
- Lau OD (2012) A Novel Modular Polymer Platform for the Treatment of Head and Neck Squamous Cell Carcinoma in an Animal ModelNovel Modular Polymer Platform. Arch Otolaryngol Neck Surg 138: 412.