Articles in Progress
2 Replies
Abstract
Background: The effective implementation of evidence-based practices (EBPs) in healthcare is essential for enhancing patient outcomes. However, in acute care settings, the adoption of EBPs can be inconsistent due to organisational barriers, hierarchical structures, and limited resources. Interprofessional collaboration and continuous professional development (CPD) are critical in overcoming these challenges, empowering nurses to apply evidence-based knowledge in clinical practice.
Aim: This study aims to investigate how EBPs are implemented in two large acute care hospitals in East England, focusing on the roles of interprofessional collaboration, nurse led initiatives, and CPD in facilitating or hindering EBP adoption.
Materials and method: A collective qualitative case study design was used to examine EBP implementation across two hospitals with different organisational contexts. Data were collected through semi-structured interviews with nurses and physicians, and non-participant observation. Thematic analysis was conducted to identify key themes.
Results: The findings highlight that formal interprofessional collaboration, such as regular interdisciplinary meetings, significantly supports EBP adoption by enhancing communication and shared decision-making between nurses and physicians. However, professional silos and hierarchical barriers remain prevalent, often slowing EBP implementation and limiting nurse input. Nurses used their clinical expertise to independently advocate for and lead small-scale EBP changes, particularly in infection control and wound care, resulting in notable patient outcome improvements. CPD emerged as a powerful enabler, boosting nurses’ confidence and capacity to challenge outdated practices and advocate for evidence-based changes.
Conclusion: Formal collaboration structures and accessible CPD are essential to successful EBP implementation. Addressing hierarchical barriers and fostering interprofessional dialogue can improve the integration of evidence-based knowledge into routine care, empowering nurses as key drivers of change.
Background
Knowledge implementation stands at the forefront of healthcare advancements, essential for driving improvements in patient outcomes and elevating overall care quality [1-3]. Evidence-based practice (EBP) in nursing involves the integration of clinical expertise, patient values, and the best available evidence to inform clinical decision-making [4]. This approach not only enhances the effectiveness of patient care but also supports the professional development of nurses by grounding practice in research and evidence [1]. However, despite substantial evidence supporting EBPs and strong endorsements from health authorities like the National Institute for Health and Care Excellence (NICE) and the Nursing and Midwifery Council (NMC), there are significant barriers to EBP implementation in acute care settings, particularly in the United Kingdom [5]. These barriers often include organisational silos, hierarchical structures, and a lack of resources and time allocated for continuous professional development, which limit the capacity of nurses to fully integrate EBPs in routine practice [6,7]. Interprofessional collaboration has been shown to significantly enhance EBP implementation, as it encourages knowledge sharing and supports decision-making across disciplines [8]. Studies have demonstrated that healthcare environments promoting interdisciplinary teamwork foster more effective communication, increase the uptake of EBPs, and ultimately improve patient outcomes [9]. Yet, evidence also highlights that healthcare organisations often operate within rigid professional silos, which impede the collaborative processes essential for EBP integration [10,11]. In particular, nurses may face challenges when their input is undervalued or dismissed in favour of physician-dominated perspectives, limiting the full utilisation of their expertise and knowledge in decision-making [2]. The persistence of these silos suggests a gap in understanding the mechanisms by which interprofessional collaboration can be consistently and effectively integrated into acute care practices to support EBP.
Nurses play a pivotal role in identifying care gaps and initiating evidence-based changes due to their continuous patient interactions and hands-on care delivery experience [12]. Studies indicate that when nurses are empowered with autonomy and professional development opportunities, they can act as change agents, advocating for and implementing EBPs independently, which positively impacts patient care [13,14]. Nonetheless, despite the recognised value of nurse-led EBP initiatives, healthcare systems often lack structures that empower nurses to independently lead such efforts, particularly in resource-limited environments where formal professional development opportunities may be scarce [15]. This challenge is compounded in acute care settings where workload pressures and staffing shortages can further limit the ability of nurses to dedicate time to EBP [6]. Addressing these barriers through targeted support, professional development, and restructuring of roles could enable nurses to make greater contributions to evidence-based improvements. A key factor in empowering nurses to lead EBPs is continuous professional development (CPD), which has been shown to significantly increase confidence, advocacy skills, and the ability to challenge outdated practices [16]. However, studies highlight disparities in access to CPD, particularly in settings with limited resources [17]. While some research advocates for structured CPD to enhance EBP implementation [18], there remains a lack of comprehensive understanding regarding the ways CPD and nurse empowerment impact EBP adoption in under-resourced acute care settings. Given the crucial role of nurses in direct patient care, addressing the gap in CPD access and exploring its impact on EBP utilisation are essential for supporting sustained improvements in healthcare quality. In response to these gaps, this study aims to investigate the dynamics of interprofessional collaboration, nurse-led initiatives, and professional development as facilitators and barriers to EBP implementation in acute care settings. By examining these factors across two large hospitals in East England, this study seeks to provide insights into the specific organisational and professional elements that enable or hinder the effective integration of EBPs. The findings will contribute to a deeper understanding of how healthcare organisations can leverage interprofessional collaboration, empower nurses, and enhance CPD to optimise patient care and support sustained EBP adoption.
Material and Methods
Research Design
This study utilises a collective qualitative case study design. The collective case study approach is ideal for examining multiple cases with shared characteristics, allowing cross-case comparison and deeper analysis of complex phenomena like EBP in healthcare settings [19]. The qualitative case study design ensures a thorough and nuanced understanding of EBP implementation challenges across diverse hospital environments [3]. The study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) [20].
Study Settings
The study took place between September 2017 and July 2023. Purposive sampling was conducted in two acute care settings in the East Midland region of England. The sample included one mid-sized general hospital (600 beds) and one large general hospital (700 beds), both selected to represent diverse leadership experiences and organisational contexts. These hospitals, the largest in the region, shared similar geographical and socio-cultural characteristics and were chosen to explore EBP in a complex clinical environment with rich data potential. The decision to focus on these two hospitals was driven by practical considerations of cost, time, and accessibility, aligning with Stake’s [21] recommendation to select cases that are both welcoming and feasible for research.
Sample Size and Participants
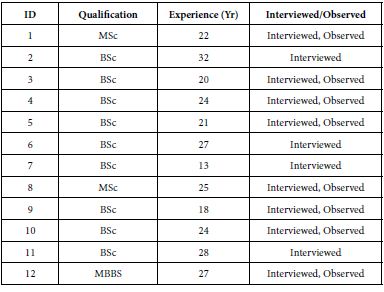
A total of 23 staff nurses (SNs) and nurse managers (NMs) and 2 Physicians participated in the study. The inclusion criteria were: (1) individuals with at least two years of experience working in these settings; and (3) those willing to participate and who signed the informed consent form. Participants were excluded if they had to withdraw due to work-related commitments or health issues during the interview period. Tables 1 and 2 present the demographics of participants. Participants in both study sites were similar. The participants’ years of experience ranged from 6 to 35 years, reflecting a broad spectrum of clinical expertise across both cases.
Table 1: Participants’ Demography (Site 1).
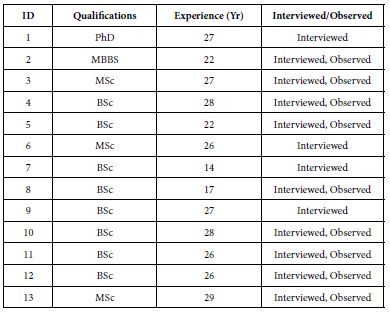
Table 2: Participants’ Demography (Site 2).
Data Collection
Data were collected through semi-structured interviews and non-participant observation (Table 3), enabling triangulation and validation of findings [22]. Interviews were guided by an interview guide (Table 4), recorded, and transcribed. Non-participant observation captured real-life interactions, providing insights into the practical implementation of evidence-based practices. In both sites, the lines of communication for EBPs were well-established, with the Research and Development (R&D) Unit playing a key role in facilitating communication and disseminating evidence-based guidelines. The R&D and Practice Development Units were also involved in developing local evidence guidelines for their respective teams.
Table 3: Data sources

Table 4: Interview Guide

Data Analysis
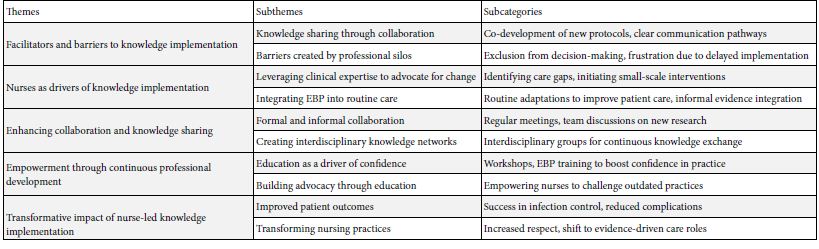
Braun and Clarke’s [23] thematic analysis framework was employed to systematically organise the finding following six key phases. The process began with familiarisation, where interview data, field notes, and observations were reviewed to understand participants’ experiences with EBP. During coding, key segments were labelled, including ‘collaborative protocol development’ ‘exclusion from decision-making’ and ‘empowerment through training’. These codes informed broader themes in the next phase: ‘Facilitators and Barriers to Knowledge Implementation’ ‘Nurses as Drivers of Knowledge Implementation’, ‘Enhancing Collaboration and Knowledge Sharing’, ‘Empowerment through Professional Development’, and ‘Transformative Impact of Nurse-Led EBP’. Themes were then reviewed for coherence and refined for clarity, defining each as it related to the study’s focus. For instance, ‘Knowledge sharing through collaboration’ addressed co-developed protocols, while ‘Barriers created by silos’ highlighted decision-making exclusions. In the final report, these themes collectively illuminated facilitators, barriers, and the impact of nurse led EBP, presenting a cohesive narrative on EBP integration in acute care settings. Overview of the key themes is presented in Table 5.
Table 5: A summary of key themes
Ethical Considerations
This study followed the ethical principles of the Declaration of Helsinki of 1964 and received approval from the University of Northampton Research Ethics Committee. Each hospital’s management also granted permission for participant recruitment. Broader ethical approval was not required, as the study did not involve minors, clinical trials, or pose any risks to participants, per UK regulations. Participants received electronic and written invitations detailing the study’s purpose, confidentiality, data handling, and their right to withdraw without consequences. Informed consent was obtained in line with GDPR. The researcher shared their professional background and explained the study’s aims to build trust [22], ensuring anonymity in reporting. All data will be securely stored and destroyed after publication, and participants were treated with respect throughout.
Rigour and Reflexivity
The study adhered to principles of credibility, transferability, dependability, and confirmability [22]. Triangulation, prolonged engagement, and multiple data collection methods, including interviews and observations, were employed to capture diverse perspectives. Spending eight months in the field enhanced credibility by providing a thorough understanding of issues affecting EBP implementation. The research process was meticulously documented, with detailed contextual information and a clear audit trail, ensuring transferability and potential replication [21]. Participant quotes supported data analysis, ensuring transparency [19]. Reflexivity was maintained through explicit acknowledgment of the study’s philosophical foundations, and a research diary preserved consistency during analysis. Finally, the COREQ guidelines were followed in reporting the qualitative results [20].
Findings
The findings reveal that effective knowledge implementation in acute care is influenced by interprofessional collaboration, nurse-led initiatives, and professional development. Key themes include the role of collaboration between nurses and physicians in facilitating knowledge sharing, though hindered at times by professional silos; nurses’ proactive leadership in driving EBPs, particularly in infection control and wound care; and the empowering effect of continuous professional development, which equips nurses to confidently advocate for and apply evidence-based changes in patient care.
Facilitators and Barriers to Knowledge Implementation
Findings from both sites show that the effective implementation of EBPs was influenced by the degree of interprofessional working between nurses and physicians. While collaboration often facilitated the integration of new practices, barriers still emerged where professional silos and communication breakdowns occurred. This theme explores how interprofessional collaboration supports or hinders the implementation of EBPs and highlights the challenges faced by nurses in these collaborative processes.
Knowledge Sharing Through Collaboration
Interprofessional collaboration was a crucial factor in facilitating knowledge implementation at both sites. The sharing of expertise between physicians and nurses allowed for the co-development of new care protocols, particularly when teams had clear communication pathways. In site 1, nurses shared: “…we worked with the doctors on a new pain management protocol, and by discussing the evidence together, we were able to agree on a more effective approach. It felt like real teamwork” (Interview, Senior Nurse, S1). Similarly, I site 2, collaboration led to quicker decision-making: “…the consultants started involving us in discussions about infection control measures…we shared our observations, and they adjusted the protocols…that kind of collaboration made a huge difference.” (Interview, Infection Control Nurse, S2). This finding demonstrates how interdisciplinary collaboration fosters a mutual understanding and respect for each profession’s expertise, enabling smoother EBP implementation.
Barriers Created by Professional Silos
Despite the benefits of collaboration, professional silos were a significant barrier at both study sites, with nurses often excluded from decision-making processes. This resulted in slower implementation of evidence-based changes and frustration among nursing staff. In site 1, nurses expressed that they “had solid evidence for a change in wound care practice, but we weren’t involved in the initial discussions…it took weeks for the doctors to acknowledge our input, which delayed everything” (Interview, Senior Nurse, S1). Similar experiences were reported in site 2 with nurses stating that they “…were pushing for months to update our catheter care protocol, but we weren’t getting feedback from the doctors…they would discuss it among themselves and leave us out, which slowed down the process.” (Interview, Nurse Manager, S2). These quotes highlight the negative impact that professional silos have on knowledge implementation, with nurses feeling marginalised and unable to influence critical decisions, despite having evidence-based insights to offer.
Nurses as Drivers of Knowledge Implementation
While hierarchical barriers remain, nurses at both study sites played a proactive role in driving the implementation of EBPs. Their clinical experience, patient proximity, and understanding of care needs positioned them as key advocates for change. This theme explores how nurses used their expertise to implement EBPs, even when formal collaboration with physicians was lacking.
Leveraging Clinical Expertise to Advocate for Change
Nurses at both sites demonstrated the capacity to introduce new practices based on evidence, using their clinical expertise to identify care gaps and push for changes. Even in environments with limited formal collaboration, nurses were able to initiate small-scale, impactful interventions. In site 1, Ward Managers seem to have utilised their expertise to advocate for EBP implementation. For example, one of the nurses expressed “…I noticed that our pressure ulcer incidence was increasing, so I introduced a new prevention strategy…the doctors were hesitant at first, but we showed results quickly, and it became standard practice” (Interview, Ward Nurse, S1)
Nurses in site 2 appeared to have done utilised similar strategies: “we started trialling a new dressing technique based on research, even before it was formally approved…once the physicians saw the improvement, they accepted it as part of our wound care protocol” (Interview, Senior Nurse, S2). These examples illustrate how nurses, using their practical knowledge, were able to implement EBPs independently, improving patient outcomes even without immediate approval from physicians.
Integrating EBP into Routine Care
Nurses at both sites consistently integrated evidence into daily care activities, often making subtle changes that did not require formal approval but had a significant impact on patient care. These routine adaptations of EBPs highlight nurses’ roles as continuous drivers of care quality improvements. In site 1, an observation of ward round revealed some clinical procedures related routine knowledge implementation: “…during rounds, a nurse adjusted a patient’s medication schedule to align with the latest evidence on pain management, even though the consultant had not yet approved the change. It made a noticeable difference in the patient’s comfort” (Observation, Ward Rounds, S1). A similar scenario played out in site 2 where during observation “nurses began closely monitoring post-surgical patients for early signs of infection, following new evidence on early detection, even though the formal guidelines hadn’t yet been updated” Observation, Post-Surgical Ward, Site 2). These examples demonstrate how nurses are able to integrate evidence into routine care processes, subtly driving improvements in patient outcomes, even when formal approval or recognition from physicians is delayed.
Enhancing Collaboration and Knowledge Sharing Through Interprofessional Initiatives
While professional silos remain a challenge, both study sites showed promising examples of initiatives aimed at fostering better collaboration between nurses and physicians. These initiatives helped to break down barriers, promote knowledge sharing, and accelerate the implementation of EBPs.
Formal and Informal Collaboration
A structured collaboration initiatives were established in site 1, with regular meetings to discuss new research and evidence-based changes in practice. This formal collaboration significantly improved communication and sped up the adoption of EBPs. One of the physicians shared: “…we’ve started having weekly meetings where the whole team, including nurses, discusses new research…it’s really improved our teamwork and made it easier to agree on new practices.” (Interview, Physician, S1). On the other hand, collaboration was less formal in site 2, but still made a positive impact as expressed by some of the nurses: “|…we don’t have regular joint meetings yet, but I’ve noticed that the doctors are increasingly asking for our input during rounds…it’s a good start” (Interview, Senior Nurse, S2). These examples suggest that while formal structures may enhance collaboration, even informal efforts can foster better communication and improve the implementation of EBPs.
Creating Interdisciplinary Knowledge Networks
Both sites showed an emerging recognition of the need for interdisciplinary knowledge networks that enable the continuous exchange of information and expertise across professional boundaries. In site 1, one of the nurses described the value of these networks as positive. “…we set up a group where nurses and doctors present the latest evidence guideline, they’ve come across…it’s helped bridge the gap between our roles and encouraged us to adopt new practices quicker.” (Interview, Senior Nurse, S1). A similar approach was developing in site 2 as indicated by the quote: “…whenever we get the chance to sit down together and discuss cases, it leads to real learning…that’s when the best ideas come up, and we’re able to implement them” (Interview, Nurse Manager, S2). The recognition of interdisciplinary knowledge sharing at both sites emphasises the importance of creating formal structures to support this collaborative learning, which is crucial for timely and effective EBP implementation.
Empowerment Through Continuous Professional Development
Education and continuous professional development are critical for empowering nurses to lead the implementation of EBPs. Both sites recognised the importance of investing in nurse education to strengthen confidence, knowledge, and the ability to advocate for evidence-based changes.
Education as a Driver of Confidence
Structured professional development opportunities, including workshops and training on EBPs, had a positive impact on nurses’ ability to implement new practices confidently. One of the nurses shared: “…after attending regular workshops on EBP, I feel much more confident bringing new ideas to the table…it’s made a huge difference in how we approach care” (Interview, Nurse Manager, S1). In site 2, education appeared to be self-driven, with nurses seeking out external opportunities: “…we don’t have as many formal training programmes, so we’ve had to find our own opportunities for development…it’s been challenging, but it’s also made us more proactive” (Interview, Senior Nurse, S2). These differing approaches highlight the need for more structured educational support at all sites to empower nurses in knowledge implementation.
Building Advocacy Through Education
Professional development not only improved knowledge but also empowered nurses to challenge outdated practices and advocate for EBPs. Nurses across both sites reported feeling more equipped to engage with physicians after receiving training. One of the nurses remarked: “…the EBP training gave me the tools I needed to confidently push for changes in the ward…now, I’m not afraid to challenge practices that don’t align with the evidence…” (Interview, Nurse, S1). Similarly, in site 2 “…the more I learn about the latest research, the more I feel I can make a real difference in care, even if it means going against established practices” (Interview, Senior Nurse, S2). These findings demonstrate how education enhances nurses’ capacity to advocate for evidence-based care and challenge traditional, less effective practices.
Transformative Impact of Nurse Led Knowledge Implementation
When nurses are empowered to implement EBPs, the results are transformative, both in terms of patient outcomes and the evolution of nursing practice. This theme explores the direct impact of nurse-led knowledge implementation on patient care and the professional development of nursing teams.
Improved Patient Outcomes
Both sites reported significant improvements in patient outcomes following the successful implementation of EBPs led by nursing teams. These improvements were particularly evident in infection control and wound care management. In site 1, a nurse shared: “…since we introduced the new infection control guidelines, we’ve seen a dramatic reduction in hospital-acquired infections…it’s been one of our biggest successes” (Interview, Infection Control Nurse, S1). In site 2, similar results were observed in post-operative care: “…the changes we made to wound care, based on the latest evidence, have reduced complications for our patients. It’s really shown how powerful EBPs can be” (Interview, Senior Nurse, S2). These success stories highlight the significant positive impact of nurse led EBP implementation on patient safety and care quality.
Transforming Nursing Practices
In addition to improving patient outcomes, nurse led EBP implementation has transformed nursing practices at both sites. Nurses reported feeling more empowered and respected within their teams, as their roles evolved from task-oriented responsibilities to research-driven care leadership. In site 1, a nurse reflects: “…implementing EBPs has changed how we work…it’s given us more credibility and made nursing more evidence-driven, which is how it should be” (Interview, Nurse Manager, S1). A similar sentiment was expressed in site 2: “…we’re no longer just following orders…we’re part of the decision-making process, and it’s changed how we see ourselves as professionals” (Interview, Senior Nurse, S2). These transformations underscore the critical role nurses play in leading the adoption of EBPs and improving the overall quality of care through evidence-driven practices.
Discussion
The findings of this study reveal complex interplays between interprofessional collaboration, hierarchical structures, and nurse-led initiatives in implementing EBPs within acute care settings. Key themes such as knowledge sharing, barriers due to professional silos, and the role of CPD emerged, all of which reinforce the necessity of a collaborative and empowering healthcare environment for EBP. These findings align with previous research while also highlighting unique challenges and opportunities within the study sites. The findings indicate that interprofessional collaboration significantly facilitates EBP adoption, a view supported by Reeves et al.., [8], who argue that interprofessional teamwork enhances knowledge exchange, ultimately leading to improved patient outcomes. Regular interdisciplinary meetings allowed nurses and physicians to share insights and align protocols, illustrating how formalised structures can improve communication, a point echoed by Grimshaw et al., [11]. However, the lack of formal collaboration structures slowed EBP adoption, suggesting that the absence of structured interactions may undermine the speed and efficacy of implementing evidence-based changes. Sullivan et al., [10] similarly argue that professional silos and the absence of regular interdisciplinary meetings can hinder EBP adoption, creating inefficiencies in decision-making. This comparative insight supports the notion that effective collaboration is contingent on formal structures that facilitate dialogue across professions, yet the findings also suggest that even informal collaboration, as observed at Site 2, can initiate positive change, albeit more slowly. Both study sites reported significant barriers due to professional silos, with nurses often excluded from decision-making processes. This aligns with the work of Dunn et al., [24-29] and Ominyi et al., [2], who found that hierarchical structures in healthcare often subordinate nursing perspectives to medical authority, limiting nurses’ capacity to advocate for EBPs effectively. The hierarchical barriers evident in this study exemplify how power dynamics in healthcare can stifle nurses’ evidence-based suggestions, even when such recommendations have the potential to improve patient outcomes. Brown et al., [15] also identified these silos as sources of frustration, as healthcare workers experienced delays in practice change implementation due to a lack of engagement and feedback from other professional groups. These barriers suggest that healthcare organisations must address hierarchical dynamics to facilitate a more inclusive decision-making process, enabling nurses to participate fully and contribute their insights into patient care practices.
Despite the hierarchical constraints, nurses at both sites demonstrated a proactive approach to EBP, using their clinical expertise to introduce evidence-based changes in infection control and wound care. This finding aligns with Harvey et al., [1], who highlight the critical role of nurses as change agents in direct patient care. Moreover, Gerrish et al., [6] found that empowering nurses to act independently often led to improved patient safety and care outcomes. Nurses in this study leveraged informal knowledge-sharing networks to drive improvements in practice, particularly when formal approval from physicians was not immediate. This self-driven initiative underscores the potential of nurse-led interventions in advancing EBP, even within restrictive organisational structures. The findings emphasise the importance of CPD in empowering nurses to implement EBPs confidently. Study findings reveal that structured CPD opportunities can boost nurses’ confidence in suggesting evidence-based changes, a result consistent with McCormack et al. [16], who argue that CPD enhances practitioners’ capacity to challenge outdated practices. However, Site 2’s reliance on self-driven educational pursuits illustrates the limitations of under-resourced environments, where formal CPD support is sparse. The disparity between the two sites reinforces Melnyk and Fineout-Overholt’s [4] argument that healthcare organisations must invest in continuous, structured professional development to support sustained EBP integration. Without organisational support for CPD, nurses may struggle to access the resources and training necessary to lead evidence-based improvements effectively. The study highlights the importance of interprofessional collaboration and nurse-led initiatives in effective EBP implementation. Formal interdisciplinary meetings enhance communication, decision-making, and reduce silos, thereby improving patient care. Additionally, investing in structured CPD for nurses builds confidence and strengthens their advocacy for evidence-based changes. Healthcare organisations should prioritise these areas to support sustained EBP integration and optimise healthcare delivery. For future research, examining ways to minimise hierarchical barriers and exploring the long-term impact of collaboration structures on EBP are essential. Research on structured CPD programmes, particularly in resource-limited settings, and identifying best practices in nurse-led EBP initiatives could further support patient care improvements.
Strengths and Limitation
This study’s strengths lie in its use of a collective qualitative case study design, providing an in-depth exploration of knowledge implementation across diverse acute care settings. Through triangulation of data from interviews, observations, and document analysis, the study ensures a comprehensive understanding of facilitators and barriers in EBP adoption. However, the study has limitations; the perspectives primarily represent staff nurses, nurse managers, and physicians, potentially overlooking insights from other key stakeholders, such as patients and policymakers, which could further enrich the understanding of interdisciplinary challenges in knowledge implementation.
Conclusion
This study highlights the importance of interprofessional collaboration, CPD, and nurse empowerment in implementing EBP within acute care settings. However, challenges persist, particularly regarding hierarchical barriers and inconsistent CPD support. Formal structures, such as interdisciplinary meetings, significantly enhance EBP adoption, though informal collaboration can still foster progress. Findings emphasise that nurses, even with limited formal support, can lead impactful EBP initiatives, illustrating their role in advancing patient outcomes. Further research should address strategies to reduce professional silos and support structured CPD, especially in resource-limited environments, to enable sustainable, nurse-led EBP integration in healthcare.
Acknowledgements
We wish would appreciate all nurses who participated in this study.
Author Contributions
JO and NA contributed to the conceptualisation and methodology of this study. JO and NA were involved in the investigation and validation of the results. JO and NA were responsible for data curation and formal analysis. JO contributed to the drafting of the manuscript, while NA reviewed and edited. JO supervised the study and provided necessary resources. All authors have read and approved the final version of the manuscript.
Funding
None received.
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declarations
Ethical Approval and Consent to Participate
This study received approval from the University of Northampton Research Ethics Committee. Each hospital’s management also granted permission for participant recruitment. Broader ethical approval was not required, as the study did not involve minors, clinical trials, or pose any risks to participants, per UK regulations. They were informed that they could refuse to answer any questions or withdraw from the study at any time. All recordings were securely stored in accordance with confidentiality principles.
Consent to Publish
Not Applicable.
Competing Interests
We declare no conflict of interest.
References
Abstract
Introduction: Information Technologies are currently essential elements for the improvement and development of a country, on the other hand, Cuba has identified from very early on the need to introduce Information and Communication Technologies in social practice and achieve a digital- technology culture as one of the crucial characteristics of the new man. Cuba is moving towards electronic-government, achieving digital technology and information literacy in the decisive processes, creating channels to increase citizen participation. How to contribute to the management of collaborative information to the citizen on health care issues in the areas of Pinar del Rio municipality?
Objective: to develop the Information Architecture for the Citizen Collaboration in the health care issues in the areas of Pinar del Rio municipality.
Methods: a Technological Innovation Research on information management in the health care areas of the municipality under study is carried out following the methodology of software development for Extreme Programming, and applying theoretical and empirical methods for the analysis, review and modeling of the processes under computerization.
Results: it was found that the proposal of information technology is based on managing the information of the different medical services, serving as a tool to help to the organization of the healthcare system and make it more efficient.
Conclusion: a computerized prototype was created that will avoid the gathering of people who come to the institutions in search of answers to questions directed to knowledge or orientation for a determined problematic on purpose of the community projection.
Keywords
Access to information, Software design, Software, Medical informatics applications, Information technology
Introduction
Information and Communication Technologies are currently fundamental elements for the improvement and development of a country [1]. In this sense, Cuba has identified from a very early stage the convenience and need to dominate and introduce social practice ICT and achieving a digital culture as one of the essential characteristics of the new man, which would facilitate society to get closer to the goal of sustainable development [2,3]. In the field of health, it offers a strength in technological progress that presents positive experiences worldwide [4,5]. The most optimistic projections in this regard suggest that a computerized and interconnected world not only ensures growth and development, but which also guarantees improvements in access to facilities that enhance the quality of life, and facilitate broad access to digital content and services for citizens [6,7]. The effort that the Cuban State has made to support the computerization of society is a fact. Concrete actions are developed throughout the country to conclude the initial stage of electronic government [8], it is not only to create the platforms, but also that they work with good practices, provide digital services to the population and interact with the people. In this way, digital and information literacy is achieved as the ability to locate, organize, understand, evaluate and analyze information through digital technology, create channels that allow increasing citizen participation [9,10]. The creation of a computer prototype [11], for the people of Pinar del Río who access the health areas of the main municipality of the province, allows the description of many useful processes to any citizen [12-14], and the possibility of having of them in a single and integrating platform [15,16]. This prototype is based on improving social welfare and the actions carried out by an informed population, in order to provide services and information to citizens, increase effectiveness and efficiency of public management [17], and increase the transparency of the sector with the participation of all communicators who require some information [18-20]. In the different health areas of the main municipality, several processes are developed, this research is immersed in the computerization of each of them, which are aimed at the satisfaction and knowledge of the citizen, maintaining the health of the population, with health promotion and community participation, with the planning, organization, monitoring and evaluation of the processes.
Whose objective is aimed at Electronic Government, where they can streamline, improve, adapt, socialize and reduce costs of the processes and/or activities of the public system, motivated by the use of advances in ICT, through channels that allow increasing participation citizen, with the aim of improving the health status of the population, increasing the quality and satisfaction of the people with the services provided, making the system efficient and sustainable and guaranteeing its development, through community projection. This will be achieved by bringing health services to the community, through the different medical specialties, and with the strengthening at all times of actions aimed at the well-being of citizens who require health services. In each polyclinic, health services are brought to the community with community projection where each specialty such as Surgery, Endocrine, Cardiology, Urology, Traumatology, Dermatology, Menstrual Regulation, Orthopedics, Adult and child Traumatology, Angiology, Nephrology, Gastroenterology, Rheumatology, Adult and child allergy, Optometry, ENT, Ophthalmology, Infertility Consultation, Driver’s License. They are carried out on different days of the week, when the patient is referred from the medical office to the area, or due to medical expenses, this arrives with the referral for the specialist to the admission department of the health unit, the Registration with the patient’s data, identity card, name and surname, doctor’s office, referred by, age, consultation date and time, and the patient is verbally notified of the day the consultation is scheduled. The patient goes to the polyclinic on the day scheduled with the specialist, without knowledge of the place or location of the consultation and the doctor who is going to attend him, as well as the regulations that are established, in addition to the different services that are provided in the institution. What results in a problem in terms of organization and rationalization of the services provided. The problem detected in the development of electronic government in the health sector justifies this research, developed with the participation of citizens who go to the different services. The work is the result of a research project of the master’s degree in Health Informatics, with the aim of developing the information architecture for citizen collaboration in health matters in the areas of the Pinar del Rio municipality.
Methods
The research is due to a technological innovation project for the development of a computer application for the management of Citizen Collaboration on health issues in the areas of the Pinar del Río municipality, in the period from 2019 to 2021, based on the study of the current needs and shortcomings of the population, in the four polyclinics of the Pinar del Rio municipality. The results presented correspond to the analysis and design stages of the project, and they used theoretical research methods such as historical-logical and induction-deduction, to capture functional and non-functional requirements, as well as modeling. of the information architecture on which the Citizen Collaboration management process in the areas of the municipality is based. Among the empirical methods, the following were used: the interview with citizens who require health services, as well as the bibliographic review during the analysis and design of the prototype of the computer application During the course of this research, periodic bibliographic reviews of articles in magazines, national newspapers, scientific publications, related to electronic government in Cuba, development and computerization of a society, literacy of the population regarding digitization of processes, web applications were carried out to manage information. The DeCS health descriptors were used as search strategies to determine keywords, databases such as SciELO, by indexing the terminologies from the common language to the permuted language. For the modeling of the prototype object of study and research, the following trends were used for its design and analysis: extreme XP programming, as an agile development methodology whose main objective is to increase productivity when developing a software project, to model, build and document the elements that make up a software product that responds to an object-oriented approach; the Unified Modeling Language (UML), for the capture of requirements, analysis, design and interoperability with other applications with a multiplatform support. ENTERPRISE ARCHITECT, one of the UML CASE tools, was also used. For the simulation of the behavior of the interfaces, the design of the wireframes and the basic prototype, Axure RP was used as a development tool.
Results
In the health sector of the Pinar del Rio municipality, several processes are developed in the admission area related to citizens who request medical appointments for the different consultations that are developed. Next, the relationship of the process to understand more clearly the aspects worked, starting from the citizen who refers his personal data to the worker who works in admission and in turn verifies if there are shifts for the required consultation, the reservation and notification of the same The research determined through the analysis of the process, the procedures, methods and techniques for solving the problem, based on the modeling of the collaborative management process with the citizen on health issues in the areas of the Pinar del Rio municipality, with the implementation of the following requirements that describe the functionality of the software. The functional requirements that the prototype must meet are nothing more than the capabilities of the product to satisfy both the customer and the end users.
Functional Requirements
R1. Authenticate User
R2. Change Password
R3. Manage Citizen Data
R3.1. Insert Citizen Data
R3.2. Modify Citizen Data
R3.3. Delete Citizen Data
R4. Manage Community Projection
R5. Show Reports
R5.1. Patient Consultations
R5.2. Patients by Date
R5.3. Query by Date
R5.4. Referred Patients
R5.5. Patients by Municipality
R6. Perform Searches
R6.1. Search Patient
R6.2. Search Patient Month
R6.3. Search Patient Office
R6.4. Search Patient by Sex
R6.5. Search Patient by Age Group
R7. Shift Notification
R8. Consult Help
The information architecture was designed, for which the analysis and design stages of the software development process were executed. The actors of the system are defined who constitute the entity that is in charge of the realization of one or more of the functionalities that must be executed. Two actors are defined in the proposed software: the citizen, who is the person who can only enter their personal data and the desired query, and receive notification of it. The admission staff is in charge of managing all the information in the application, that is, inserting, modifying and deleting, in addition to changing the password, and accessing all the consultation options, searches provided by the system and obtaining reports. The functionalities diagram based on the XP methodology is shown, with the relationship between the actors and the different processes of the proposed system.
Description of the System Functionalities
The tool is designed to satisfy the information management requirements of the Citizen Collaboration on health issues, by providing services to the community. With the implementation of the software, which is designed to work from the web, through the network of networks on any platform, which for Pinar del Río citizens who access the health areas of the head municipality of the province allows the description of many useful processes, and the possibility of having them in a single and inclusive platform and the actions carried out for the sake of an informed population, in order to provide services and information to citizens, increase the effectiveness and efficiency of public management. With an informed population, resources, development and knowledge are gained. At the same time, it allows the citizen from his home, work center, recreational area, through the technological development that the province has in terms of info-communications. This prototype manages information regarding health issues in terms of information from polyclinics on location, mission and vision, structural and organizational composition, in addition to the services provided, information related to primary health care, epidemiological alerts, programs specialized, and everything concerning the community projection.The system is designed so that any user can access its interface, select the health area and view the information options that it provides, the citizen must select the health area to which they belong in order to access it, obtain information on health issues and be able to request any consultation related to community outreach. The citizen presses on the community projection button, a window is displayed with the relationship of the consultations by specialty, with the time, day and frequency per week, as well as their location. It must be selected with a click on the query button to schedule a desired shift. The functionality for the Citizen Data management is essential for the beginning of each process, Once the health area has been selected, the citizen selects the consultation to which he was referred to program the doctor’s turn, the system refers you to a new window, to fill in the data requested by the form, name and surname, identity card, municipality, doctor’s office, age, sex, referred by, specialty. Once these data are entered, the citizen’s e_mail and contact telephone number is required so that he or she is notified of the turn for consultation. The citizen must fill in all the fields that present an asterisk (*), these data being mandatory. The system specifies the mandatory fields that must be filled in. When any field is left blank, the process does not end. The system sends you a message.
The system sends a message if when you are going to enter the identity card number you put letters instead of numbers and if any character is missing it returns a message specifying the error. When the citizen is going to enter the date for the consultation. Where the system specifies that only 24 appointments can be given per consultation and the 24 patients are already complete for that date. The system sends a message specifying that there are no available shifts for that date that you must select another and disables the remaining fields. If there are shifts for the selected date, it allows the introduction of the citizen’s email and contact telephone number, captcha the image provided by the system to make sure that it is not a robot and if a user. The citizen clicks on the save button where this information is stored in the Database and the fields are cleared. Once all the data has been entered correctly, click on the Send Notification button, the system sends a notification message of the shift via email with the confirmation of the requested medical shift. The admission staff for each health area enters the prototype through a form where they enter their Name and Password in the corresponding text boxes when pressing the Enter button. If the user is recognized by the application (he is registered in the database of users with access), it shows him the corresponding interface, according to his role in the application. If, on the other hand, the user is not recognized, the application displays an error message “Incorrect username and/or password” in which it warns the user that they do not have rights to access the management of the processes that are develop in the area. The functionality of the admission staff shows the data of the patients that were previously inserted by the citizen, and that are stored in the database; the Reports that the system allows, as well as the Searches to it. It also allows you to change the password periodically as a security measure, and consult the help of the application for any questions in this regard. The application shows the registry of all the patients who were introduced to the system by the citizen himself with his personal data, in addition to the community projection or consultation to which he was referred to be evaluated with the specialist. It allows the admission staff to modify some patient data or delete the unnecessary record. To modify the data of a patient or citizen in the system, the admission staff must select the name of the patient to be modified. As long as the patient has not been selected, the rest of the form data is disabled. Among the functionalities of the application are the Reports, which are aimed at providing information regarding the information management process with the citizen in relation to community projection. The event starts when it is necessary to know, according to a specific query, the patients that are registered. The system sends a message to select the consultation, and returns a list of all the patients that are registered for the selected consultation. In the same way, to know the patients who are registered for a previously selected date.
Discussion
The research carried out is due to a technological innovation project for the implementation of a computer application for citizen collaboration management in the health areas of the Pinar del Rio municipality. It is necessary to computerize the development of collaboration with the citizen on health issues in the different areas of the Pinar del Río municipality, which allows managing all the information of the different medical services, therefore it constitutes a tool to help organize the system and provide you with more efficiency. The absence of a computerized system for the management of information to the population results in disorganization, the accumulation of personnel who go to the institutions in search of answers about the consultations of a specialty, the time and location, the procedure to be followed in mind to be attended by trained personnel to provide quality service. As part of the study of the object of computerization, a review of health sites with related topics was carried out that provide information to citizens who interact with software used in the country. The website entitled, National and Foreign Health Sites, stands out, showing a compilation of links to sites on public health issues in Cuba Among them are the Provincial Nodes of Infomed, Health Specialties and Topics, Sites of Interest, Medical Societies, Health Legislation and Policies, Hospitals and Institutes, Faculties of Medical Sciences, as well as foreign sites on health in Spanish [15].)
The analysis carried out on similar sites that provide information to the population on health issues, allowed to shape the structure of the application according to the citizens of Pinar del Río, whether they refer to information of a general nature from the institutions, such as those related to health care properly with the community projection. Where it could be verified that, in the confronted sites, the information is very general and with the characteristics of each unit. In the province of Pinar del Rio there is El Portal del Ciudadano Pinareño [10], which is part of the strategy drawn up by the Government in the province of Pinar del Río to implement electronic governance. More than thirty entities subordinate to the Council of the Provincial Administration (CAP) and other organisms of the province participate in this project. In addition to showing the work of the Government, in favor of the well-being of citizens and society in general. Existing computer systems do not meet the expectations of the health sector because the population needs to be more documented, to know everything concerning community projection and how health services are brought to the community, through plans, services or programs than institutions. All with the aim of improving their living conditions and thereby stimulating support for the family.
Conclusions
With this research, the Information Architecture for Citizen Collaboration in Health matters was developed in the areas of the Pinar del Rio municipality. The results of the analysis and design stages of the information management software have been presented. In each stage, the required documentation has been prepared according to the development methodology, in addition, the implementation of the application prototype, as a conclusion of the design stage and its analysis. This software motivates the need to streamline, improve, adapt, socialize and reduce costs of the processes and/or activities of the public system and create channels that allow increasing citizen participation.
References
The availability and adoption of mobile money services have transformed financial inclusion and service delivery in many developing countries (Donovan, 2012). In Liberia, the immunization program post Ebola Virus Disease (EVD) has faced challenges in efficiently managing financial resources and making timely payments to vaccinators and other health workers, thereby hindering the effectiveness of immunization service delivery. Hence, this mixed- method study was conducted in November 2024 to assess the impact of integrating mobile money payment mechanisms into the financial management system of the Expanded Program on Immunization in Liberia. The review of existing literature suggests that mobile money has the potential to enhance financial inclusion and improve the efficiency of immunization service delivery and other health services in the health sector. Mobile money has been shown to facilitate risk-sharing and promote welfare, though the evidence on its direct economic impact is still limited. (Aron, 2018) The use of mobile money for immunization programs specifically has shown promising results in increasing vaccination coverage through SMS reminders and educational tools for health workers. (Oliver‐Williams et al., 2017). In the case of Liberia, the integration of mobile money into the immunization program’s financial management modalities has helped address the challenges of timely payments and better assurance that payments reach persons for which they are intended, thereby improving health worker motivation and the overall effectiveness of the program. Liberia is dealing with the aftermath of brutal civil wars, the last of which ended in 2003. The infrastructure challenges include poor road infrastructure and underfunded health sector. Gavi, the vaccine alliance is the main funder for routine immunization in the Liberia. An review by the funder’s auditors in 2018 recommended improvements in the financial management systems for the grants at the Ministry of Health. The actions put in place included assurances that payments that MOH/EPI made at community level reached their targeted beficiaries, with timely submission of accountability reports to the center in Monrovia. In 2019, in response to severe economic constraints, the government implemented a salary harmonization exercise which included a cap on personnel recruitments. Subsequently, the development partners provide funding for monthly stipends for recruited health workers.
Highlights from Liberia’s Routine Immunization Program
Despite being one of the world’s least developed countries with low health sector funding, having a health expenditure per capita of $112 in 2021, Liberia immunization coverage for DTP 3 / Penta 3 is 82% (WUENIC 2023 Report) of its targeted population between the ages of 0-23 months by December 2023, from 78% in 2022 thereby recording a percentage increase of 4%. The country relies on the support of international organizations like GAVI, The Vaccine Alliance, USAID, The World Bank, WHO and UNICEF to undertake activities which assure a high immunization coverage. The COVID-19 pandemic affected immunization seeking behaviours because of fear, hesitancy, and mistrust about vaccines, which resulted in a drop in immunization coverage rates for routine vaccines. However, the government of Liberia and its partners were strategic in making a substantial comeback through the development and implementation of an immunization recovery plan, which culminated in increased immunization coverage, as evidenced by the WUENIC 2023 report. It can be recorded that the use of a mobile money payment mechanism for timely and transparent payment of fit-for-purpose immunization workforce (vaccinators and other health workers) was one of the enablers for Liberia’s success in the attainment of 81% fully vaccinated coverage for COVID-19 vaccine. Based on the progress made in increasing the immunization coverage as measured by DTP3 and MCV1, Liberia has been consistent over the past two years with attaining the Millennium Challenge Corporation (MCC) indicator for immunization thereby setting the government on track for obtaining a new MCC Compact.
Trend in Routine Immunization Coverage Despite Low Spending
By 2023, Liberia achieved a notable increase in vaccination coverage. For instance, according to the WUENIC report, the DPT3 vaccine coverage will rise from 65% in 2020 to 82% by 2023. This improvement was largely due to intensified and targeted vaccination efforts (i.e., Outreach, Periodic Intensification of Routine Immunization-PIRI campaigns, etc.), timely payments of remunerations, supportive supervision and the strengthening of the immunization program and, by extension, the health system. Despite these gains, challenges remain, including reaching zero-dose children in remote and underserved areas and maintaining consistent vaccine supply chains. Continued efforts and support from global health partners will be crucial to sustain and further improve immunization coverage in Liberia (Figure 1).
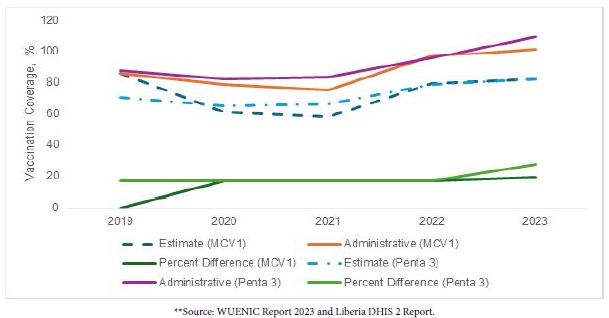
Figure 1: Efforts and support from global health partners.
A Key Lesson on the Use of Mobile Money Payment Mechanism in Enhancing Transparency, Accountability, and Improving Program Performance within the Liberia Expanded Program on Immunization
Mobile money has significantly transformed financial transactions of the Expanded Program on Immunization at the Ministry of Health, Republic of Liberia since its introduction in 2021. The Expanded Program on Immunization entered into contract with the two main mobile telecommunications services providers, MTN Lonestar and Orange. With the contracts, the mobile providers set up payment platforms at the Ministry of Health Office of Finance Management (OFM) and trained users. The EPI and OFM teams conducted a nationwide registration of vaccinators and their particulars including, health facilities assigned, county, names, phone number, and supervisor names. With this information, a payee master list was created and submitted to the mobile providers who validated the names and phone number. With this validated list, the Ministry of Health was able to make periodic payments to health workers. Liberia’s implementation of mobile money and significant advancements in routine vaccination coverage rates exemplify the impact of innovative digital solutions in enhancing the speed and efficiency of financial transactions, as well as in developing customized strategies for expanding coverage and addressing outbreaks of vaccine-preventable diseases. This situation illustrates the substantial outcomes that can be achieved through appropriate innovation and tailored strategies, even in constrained fiscal conditions. The accomplishments of Liberia’s Expanded Program on Immunization can be distilled into seven essential lessons.
National and Subnational Leadership
Based on one of the findings from Gavi’s Audit and Investigation in 2018, Gavi contracted a financial management firm to provide technical support and capacity building to the Expanded Program on Immunization and the Office of Financial Management (OFM). Said recommendation was embraced by the honorable minister and the senior management team of the ministry of health which play a crucial role in the effective implementation of mobile money for immunization programs in Liberia. At the national level, the honourable minister of health, the senior management team of the ministry, the EPI manager, the Office of Financial Management, the internal audit unit, and the compliance unit play pivotal roles in creating policy frameworks that facilitate the adoption and use of mobile money systems by the Expanded Program on Immunization (EPI) and other programs subsequently. This includes providing regulatory support and ensuring that the mobile money payment is secure and accessible to all immunization service providers (e.g., vaccinators and other health workers). For instance, a mobile money steering committee was established and headed by the honourable deputy minister for administration. By promoting public-private partnerships, national leaders encourage investment in mobile money infrastructure and ensure that the technology reaches even the most remote areas, thereby ensuring that other projects and programs adopt said payment mechanisms. At the sub-national level, county health officers, officers-in-charge, and community structures were essential in bridging the gap between national policies and community practices. At the community and health facilities levels, the community development committee and the health facility development committee were charged with the responsibility during their monthly sitting to leverage their close ties with community members in advocating and explaining the use of mobile money in health services, including immunization programs. Working directly with health workers and subnational leaders has helped in the effective implementation of mobile money systems that align with the specific needs and contexts of health facilities and their communities. Moreover, the collaboration between national and subnational leadership is crucial to enhancing the overall effectiveness of mobile money in immunization programs. National leaders can provide the necessary resources and policy support, while subnational leaders ensure that these policies are effectively implemented on the ground. By fostering a coordinated approach, leaders at all levels can address challenges such as technological literacy, network connectivity, and financial inclusion. Strong leadership ensures that the benefits of mobile money are maximized, leading to improved vaccination coverage rates and better health outcomes for the population. A key lesson learned is that strong leadership at the national and sub-national levels through collaborative effort is essential in transforming health service delivery, including immunization, and achieving broader public health goals in Liberia. The successful implementation of mobile money payments within the Expanded Program on Immunization is a glaring demonstration.
Vaccinators’ Satisfaction with Mobile Money Payment
Bringing payment directly to the payees is a transformative digital solution that has been a game changer within the immunization landscape because of its availability and the reduction of bureaucratic bottlenecks and logistics. Out of 252 fit-for-purpose vaccinators interviewed from 252 health facilities across nine counties from northwest, north-central, south-central, and south-eastern Liberia, 63.1% (n=159) said that they were satisfied with the use of the mobile money for immunization transaction which demonstrates increased financial inclusion, especially for those who previously had limited access to traditional banking services due to geographical location and struggle to receive their just remuneration after conducting immunization services. Additionally, they indicated that it has brought a sense of respect and dignity to them within their communities. Table one provides a detailed breakdown of respondents’ reactions to the use of mobile money payment mechanisms for immunization operations. Several key lessons have been learned from mobile money platform use as an innovation in financial management, particularly in Liberia. These lessons include but are not limited to the following (Table 1):
Table 1: How satisfied are you with receiving your payments through mobile money?
| Frequency | Per cent |
Valid Percent |
||
|
Valid |
Very satisfied |
89 |
35.3 | 35.3 |
|
Satisfied |
159 | 63.1 |
63.1 |
|
| Neutral |
4 |
1.6 | 1.6 | |
|
Total |
252 | 100.0 |
100.0 |
|
Transactional Time: How Long Does it Usually Take for Vaccinators to Receive Payment after the Outreach Vaccination Campaign?
Payment of vaccinators for an outreach and/or vaccination campaign can vary widely based on several factors. Ideally, a well- structured mobile money system should be able to effect payment within 24 to 48 hours after the conduct of a health facility outreach and/ or vaccination campaign has ended. However, out of 252 vaccinators interviewed, 54.4% (n=137) stated that they received payments for health facilities outreach within one to two days upon completion. At the same time, 45.6% (n=115) indicated that it takes more than five days. A key lesson learned is that the system is effective to an extent because more than fifty per cent of the participants attest to receiving their payment within one to two days. However, it is noteworthy that there are some situations in which payment may not come so quickly. For instance, administrative inefficiencies, verification processes, loss of network and/or technical issues related to the mobile money platform can further delay the payment period. In some instances, delays for vaccinators might last for days or even weeks to receive the requirements for payment due. Indefinite delays could lead to considerable inconvenience and dissatisfaction among vaccinators, which will negatively impact their morale and the effectiveness of the program. Hence, having a well-structured system for resolving issues in a timely manner will also help to enhance mobile money payments’ reliability and efficiency for this fit-for-purpose immunization workforce and other health workers.
What is Your Overall Experience with Mobile Money Payments Compared to Traditional Payment Methods for Vaccinators?
The use of mobile money platforms as cashless payments has greatly improved the payment process for vaccinators when compared to the traditional system (e.g., hauling cash around) as payments are sent directly to their mobile phones, vaccinators no longer must spend long hours travelling to collect their salary. Out of 252 vaccinators interviewed about their experience with the use of mobile money platforms compared to the traditional system, 59.9% (n=151) indicated that they had a better experience with the use of mobile money as opposed to the traditional system, citing bureaucratic bottlenecks and logistics as major challenges associated with the traditional system as shown in table 2. It was highlighted that mobile money saves time and minimizes the risk involved with transporting cash. Finally, the instantaneous nature of mobile money transactions means that vaccinators are paid quickly, boosting their finances and morale in an immediate fashion. That said, mobile money payments come with their challenges. However, remote areas may experience network issues that could result in delayed transactions, while some vaccinators may not be digitally inclined and thus could face challenges in using mobile money platforms. While mobile money is deemed efficient, some vaccinators expressed concern about abuse and/or other lingering concerns, as the threat of fraud or unauthorized access to accounts is ever-present. Nonetheless, mobile money has generally been a positive change, providing both greater efficiency and greater access over traditional banking and cash-based systems (Table 2).
Table 2: What is the overall experience with mobile money payments compared to traditional payment methods for vaccinators?
|
Frequency |
Per cent | Valid Percent | ||
|
Valid |
Much better |
70 | 27.8 |
27.8 |
| Better |
151 |
59.9 | 59.9 | |
|
About the same |
26 | 10.3 |
10.3 |
|
| Worse |
5 |
2.0 | 2.0 | |
|
Total |
252 | 100.0 |
100.0 |
|
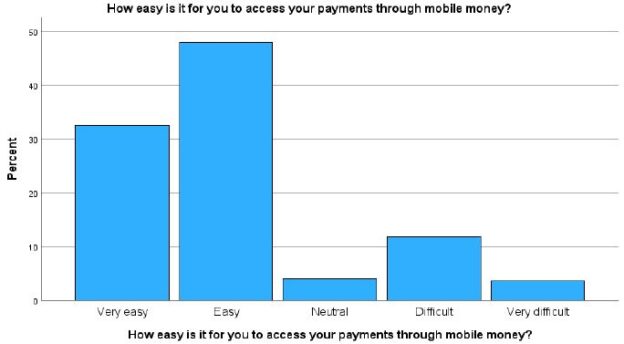
How Would You Rate Challenges Associated with Accessing Payments through Mobile Money Platforms for Immunization Activities?
Out of 252 vaccinators interviewed, the majority (48%, n=121) indicated that accessing mobile money is easy when compared to the traditional system because their incentives and/or salary are paid directly on their mobile phone, meaning that they (e.g., vaccinators) no longer need to journey long distances to collect their wages. This payment method has enhanced the time spent on financial transactions while minimizing the risk of carrying cash. The real- time characteristic of mobile money payments is that vaccinators receive their payments immediately, allowing them greater financial stability – and, with that, motivation. However, there are still issues being faced when using mobile money payments. For instance, network challenges are one of the key challenges highlighted by vaccinators working in rural and underserved areas. Transforming immunization financial landscape using mobile money platforms, however, has been a journey that while positive overall, has not been without some bumps along the way, such as sub-optimal network coverage, therefore it is imperative to have a cross-sectoral approach to improving telecommunications access and digitial payments in the more remote areas of the country (Figure 2).
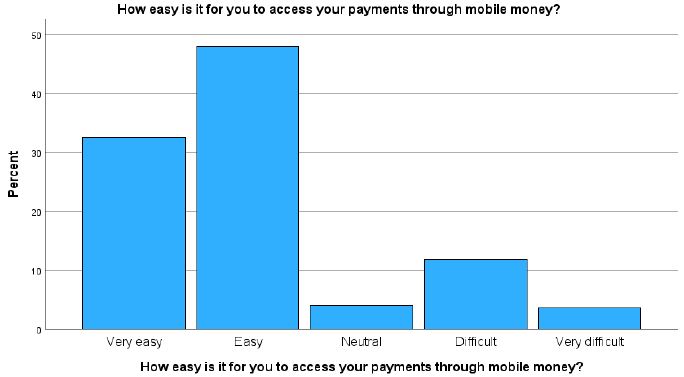
Figure 2: Cross-sectoral approach to improving telecommunications access and digitial payments in the more remote areas of the country.
Leveraging Data, Tracking Performance and Payments, and Course Correction
To ensure efficient immunization spending, data-driven strategies like health facility microplanning, mobile money payment reconciliation, and community profiling have been essential in identifying, monitoring, and improving vaccination efforts. By mapping and profiling communities, the immunization program can develop tailored service delivery interventions to reach zero-dose children, missed children, and underserved communities. This targeted approach allows districts and counties to use health microplanning to pinpoint areas with low vaccination coverage rates effectively. By doing so, their efforts were concentrated on specific areas, enabling them to apply targeted interventions and adjust strategies in real- time. The use of data ensured that no community was overlooked and that corrective measures were both timely and effective. A key lesson learned is that understanding the target population and their locations is crucial to achieving successful immunization outcomes.
Hence, it is imperative to underscore the need for high-quality data to implement targeted interventions effectively. Therefore, investing in data quality is therefore critical for both routine immunization programs, financial decisions, and outbreak response efforts.
Immunization Supply Chain and Logistics Management Information System
In Liberia, the use of mobile money services has significantly enhanced communication on the immunization supply chain and logistics management information system by ensuring the conduct of monthly health facilities outreach and averting potential and/or reducing stockouts of vaccines and vaccine supplies. 70% (n=176) of respondents indicated that with the timely payment of outreach support and monthly incentives, they could transport their vaccines to avoid stockouts and maintain the health facility’s integrity with the communities. A key lesson learned is the importance of local leadership at the health facility level to avert stockouts of vaccines and supplies, especially in hard-to-reach areas, where delivering multiple vaccines is challenging due to geographical accessibility.
Association Between Outreach Payment and Increased DTP3/Penta3 Immunization Coverage
A study was conducted to determine the association between outreach payment and increased DTP3 / Penta3 immunization coverage. Out of 252 vaccinators interviewed, a chi-square test analysis was run to determine the likelihood of an association. However, the findings revealed that a value of 0.282 with 1 degree of freedom (df) and an asymptotic significance (p-value) of 0.595 were observed. This indicates that the observed data are not significantly different from what would be expected under the null hypothesis. Hence, the observed data reveals that there is no association between outreach payment and an increase in DTP3/ Penta 3 coverage (Table 3).
Table 3: Chi-Square Tests
|
Value |
df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) |
Exact Sig. (1-sided) |
|
| Pearson Chi-Square |
.282a |
1 | .595 | ||
|
Continuity Correction |
.141 | 1 |
.708 |
||
| Likelihood Ratio |
.286 |
1 | .593 | ||
|
Fisher’s Exact Test |
.642 |
.357 |
|||
| Linear-by-Linear Association |
.281 |
1 |
.596 |
||
| N of Valid Cases |
252 |
Resumo: No Brasil, é determinado pela Constituição Federal de 1988, que o direito à saúde seja viabilizado por meio do Sistema Único de Saúde (SUS) e que o acesso deverá ser universal, integral e gratuito, esse acesso é realizado através da ações das políticas públicas, que representam um conjunto de programas, ações e decisões tomadas pelos governos (federal, estadual ou municipal) com a participação, direta ou indireta, de entes públicos ou privados, essas políticas têm como objetivo garantir a cidadania e o bem-estar social. É de responsabilidade do Estado o desenvolvimento da política de saúde mental, a assistência e a promoção de ações de saúde às pessoas em condições de transtornos mentais, com a devida participação da sociedade e da família. A literatura científica apresenta que estudantes universitários estão fortemente sujeitos ao esgotamento mental e ao desenvolvimento de Transtornos Mentais Comuns (TMC), pois enfrentam, em seu cotidiano, diversas mudanças e adaptações com o início da vida acadêmica que trazem além da mudança do ensino médio para acadêmico, outras transformações que vão desde a saída do lar parental e organização financeira ao planejamento de excedentes horas de estudo. Essa tensão se estende ao longo do curso com as cobranças acadêmicas. Este ensaio teórico teve por objetivo refletir sobre as diversas questões do cotidiano acadêmico e o impacto na saúde mental de estudantes universitários durante o processo de formação. Foi realizada uma busca exaustiva pela literatura científica dentro da temática de saúde mental universitária, que identificou a população jovem adulta como grupo risco para o desenvolvimento de TMC, apresentado problemas relacionados como a ansiedade, depressão e suicídio. Estudos têm apontado que o jovem quando inserido na universidade tem mais chances de adoecimento do que os outros jovens da mesma idade que não cursam a universidade. O Censo de Educação Superior de 2019 apresentou que 8,6 milhões de jovens brasileiros estão matriculados na universidade. Esse ingresso na universidade é uma grande conquista, mas envolve mudanças, desafios e, também, adoecimento. Em todo o mundo várias pesquisas envolvendo estudantes universitários são realizadas, motivadas por situações psicossociais, econômicas, políticas e até mesmo questões referentes ao próprio ensino. Há diversos fatores associados ao sofrimento psíquico de estudantes universitários, maior vulnerabilidade do sexo feminino e uma variância da prevalência de depressão de 9,3% a 85% de acordo com a localidade, aspectos socioculturais e econômicos. É preciso que haja discussões entre gestores de saúde e as instituições de ensino superior sobre necessidades de saúde, singularidades de diversos grupos específicos, população jovem e estudantes universitários para implementação de programas e políticas de saúde mental com vistas à promoção da saúde, prevenção de riscos ao adoecimento mental, com participação e proatividade de todos, efetividade das ações de diagnóstico, acompanhamento e controle, assegurando aos universitários a conquista de uma nova profissão e o direito ao acesso universal à saúde e à educação com qualidade e como princípio fundamental para o desenvolvimento da cidadania.
Palavras-chave
Estudantes Universitários; Políticas Públicas; Saúde Mental; Sofrimento Psíquico; Universidade
REFERÊNCIAS
Abstract
Ninety-nine young respondents evaluated different combinations of messages about the effects of substance abuse and sleep issues. The test stimuli were messages developed by generative AI (ChatGPT 3.5). The research followed the process established by the emerging science of Mind Genomics. The study investigated four elements (messages) each about four topics related to drug use: dangers and negative consequences, health alternatives to drug use, in depth consequences when one uses drugs, how poor sleep affects mood, energy levels, and ability to focus. The 16 elements were combined by experimental design, the specific combinations of elements (messages) differing for all respondents. The rating was “Describes Me.” Analysis by ordinary least squares regression showed that no single message strongly applied to the entire panel of 99 respondents. Clustering to generate three mind-sets showed three distinct groups, easy-to-interpret response patterns. These are Leisure Enthusiasts who do not respond to the negative elements (n=44), Serious Behavioral Problems (n=31), and Emotion Issues with Impaired Judgment (n=24). AI summarized the mind-sets clearly at two levels, first in terms of strong messages and suggestions for new ideas, and then at a more global level. The paper shows the feasibility of creating databases of the mind at low cost, within a day, with powerful insights and direction for communication emerging from the process.
Keywords
Adolescent sleep issues, Adolescent substance abuse, Generative AI, Mind genomics
Introduction
The growing problem of drug use leading to sleep disorders among adolescents is becoming increasingly relevant to medicine specifically, but to society in general. According to current research, misuse of drugs made for children and adults may, in some cases, negatively affect sleep patterns, leading to a variety of health problems and cognitive deficits [1-3]. A conventional approach by practitioners provides targeted treatments and therapies to address both the drug misuse problem and the sleep disorders, considered as two different indications. Problems frequently occur when teenagers resist therapy or do not cooperate with prescribed measures, either or both making it difficult for healthcare professionals to effectively address the problem. The result is that adolescents suffering from drug use and sleep issues may express themselves in a number of ways, using language indicative of bewilderment, frustration, and pessimism. Emerging societal difficulties associated with drug use that cause sleep problems in teens include increasing rates of scholastic underachievement, social isolation, and mental health illnesses. In turn, parents of these adolescents may report feelings of shame, powerlessness, and concern for their child’s well-being, exacerbating the issue [4-6].
Parents may go to considerable measures to address this issue— these include obtaining help from mental health specialists, attending therapy sessions with their child, and adopting tougher regulations and monitoring to handle substance addiction and sleep problems. However, the complexities of drug use and sleep issues in teens coupled with other behavioral issues involved in maturation make long-term remedies hard to achieve [7,8]. When addressing the growing problem of drug use resulting in sleep disorders among teenagers, a key issue is how drug use affects the brain and interrupts young people’s normal sleep habits. Adolescent sleep patterns may also be influenced by external variables such as drug usage, which can cause increased anxiety, restlessness, and interrupted sleep cycles, as well as the social determinant of drug use. Certain medicines such as stimulants and depressants have been reported to interfere with the synthesis of neurotransmitters which govern sleep, making it harder to fall and remain asleep. Other factors to consider which lead to teenage drug use are social and environmental situations. For example, peer pressure, stress, and a lack of parental monitoring may all contribute to young people commencing and continuing drug misuse habits [9].
Helping the Young Medical Professional to Understand the Adolescent Mind
Medical professionals play a vital role in understanding the minds of their adolescent patients, especially when it comes to identifying and addressing substance abuse issues. Experience can be a valuable asset in this regard. Seasoned doctors may have encountered a wider range of cases and developed a deeper understanding of adolescent behavior and mental health. However, not all doctors have extensive experience with adolescent patients [10,11]. One standard way to learn about a patient’s mind is to use questionnaires. At the time of this writing, fall of 2024, the practice of surveys is well-established in many domains, whether medical, commercial, and even recreational. The interested professional focuses on the topic and attempts to generate a set of questions about that topic, with these questions requiring simple answers. The common practice is to present these surveys, either or person, or more frequently on the internet. The survey-taker, known as the respondent, completes the questionnaire [12].
Questionnaires are powerful tools to gather information about adolescent patients, their experiences with substance abuse, as well as their sleep problems. By asking targeted questions about drug use, sleep patterns, and related behaviors, medical professionals can gain a better understanding of the factors contributing to these issues. Various questionnaires have been developed for use with teens, providing valuable data that can inform treatment plans and interventions aimed at addressing substance abuse and sleep disturbances in young people.One of the interesting sidebars of the “survey business” is the biases that the survey creator, viz., the “researcher” encounters. Biases range from non-response (refused to participate) to indifferent (assigned random responses), and all too often attempt to “outsmart” the researcher by guessing what are appropriate, socially acceptable answers, rather than real answers [13].
Creating a system that allows medical professionals to understand the minds of adolescents poses a significant challenge when the doctor lacks experience or the patient is non-communicative. Traditional methods of patient assessment may not always be effective with younger populations, who may struggle to express their thoughts and feelings verbally. In such cases, innovative approaches—such as using targeted questionnaires or assessments specifically designed for teens—could offer valuable insights into substance abuse and sleep-related issues. One metaphor for understanding the minds of adolescent patients is the concept of taking a patient’s blood at the start of the patient-doctor interaction. Just as a blood test can provide valuable insights into a patient’s physical health, a metaphorical “phlebotomy of the mind” could help medical professionals assess the mental and emotional well-being of their adolescent patients. By developing a systematic approach to understanding the minds of young people, doctors may be better equipped to address issues such as drug use and sleep problems [2,14,15].
The Mind Genomics Set up Process — AI Generated/ Human Edited Questions and Answers, Human Generated Classification and Rating Scale
An alternative approach to asking single, disconnected questions about a topic is to present people with combinations of ideas or messages, and instruct these respondents (viz., our survey-takers) to read the combination and to rate the entire combination. Furthermore, these combinations are comprised of single messages, simple phrases, seemingly thrown together in a haphazard manner, although later we will show that this seemingly haphazard manner is far from the case. The combinations are structured according to an underlying experimental design [16]. The task is rather easy, although boring. The respondent sits in front of a computer screen. The respondent sees combinations of messages emerge. The respondent simply rates the combination. The average person simply goes through these combinations in almost an indifferent fashion, feeling like some how they are guessing. The reality is that there is an underlying structure, the ratings make sense, and the results show how people think.
The process presents people with ordinary “slices of life” created in a way that the respondent cannot “game the system.” Rather, after a moment of surprise, most respondents sit down and do the task. The respondent ends up “grazing”, looking at the vignette and then assign a rating. The system invokes what the late Nobel economist called System 1 thinking, where the responses are virtually automatic. The process works very well with motivated as well as unmotivated respondents. There is no requirement that the respondent think about the topic. Rather, it suffices that the respondent pays some attention to the material, and not just type the same answer again and again [17]. Mind Genomics requires four questions and four answers to each question. If that is done, the rest of the exercise is simple. But how does the researcher come up with these questions? The early history of Mind Genomics revealed a major block to the successful use of the approach. Many people, including professionals, ended up ‘freezing’ when instructed to provide four questions. It was simple enough to name the study, but the creation of questions posed problems— generally emotional ones. As an example, consider Figure 1: Panel A shows the screen as presented to the user. Figure 1, Panel B shows a completed screen. Often the requirement to create a set of four questions which “tells a story” becomes a daunting task, an obstacle to be overcome in the research process [18,19].
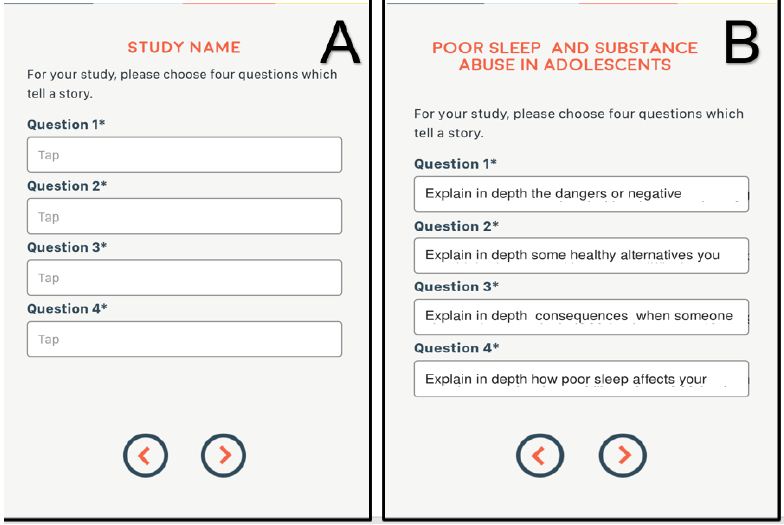
Figure 1: Panel A shows the screen as presented to the user. Panel B shows a completed screen
Recent enhancement of the Mind Genomics platform has incorporated AI in the form of LLM, large language models (here ChatGPT 3.5). The access to the AI is by means of Idea Coach, a small rectangle in which the user can type the request. Table 1 (top) shows the query as provided to the AI, and Table 1B shows the 15 questions generated from this first iteration. The query is simple, stressing simplicity and understandability. Once the user is satisfied with a question, it is a simple matter to select that question. The selection of a question results in the insertion of the question into the study. When the question has been selected, it is straightforward for the researcher to edit the question, polishing and formatting it so that the subsequent AI effort to “answer” this question will generate meaningful answers, rather than just questions which end up with yes/no answers. The same process is used to select four answers for each question. Idea Coach maintains the selected questions, allowing the user to iterate to find answers and then polish them before inserting the answers into the template [20,21].
In the use of the LLM, the questions and answers usually require some editing. The questions should be edited to encourage expansive answers, using words like “explain in detail”. This embellishment is important because the AI will use the questions themselves to drive the creation of answers. The research requires answers which paint a word picture. The only way to get those answers painting a word picture is to instruct the AI to “explain” or “embellish,” or “describe how”. These are words which generate meaningful phrases painting the word picture.
The next step creates the self-profiling classification questionnaire which enables the researcher to gain more information about the respondent. Two questions are automatically asked—age and gender. The researcher can ask up to eight additional self-profiling questions, each with a possible eight answers. Table 2 shows the self-profiling classification created specifically for this study by the researcher.
Table 1: The instruction to AI to create the questions (top), and the 15 questions created in this iteration.
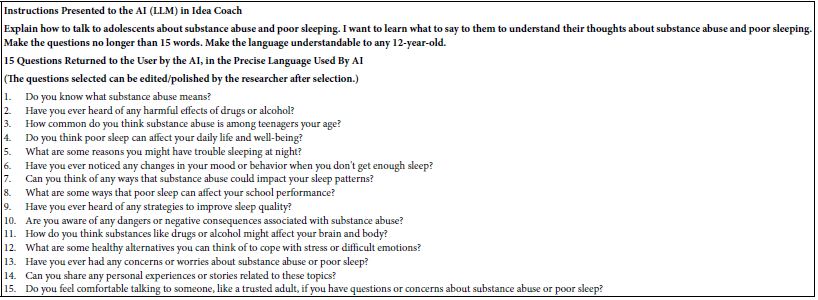
Table 2: The self-profiling questions and answers, completed at the start of the evaluation, before any vignettes are rated.
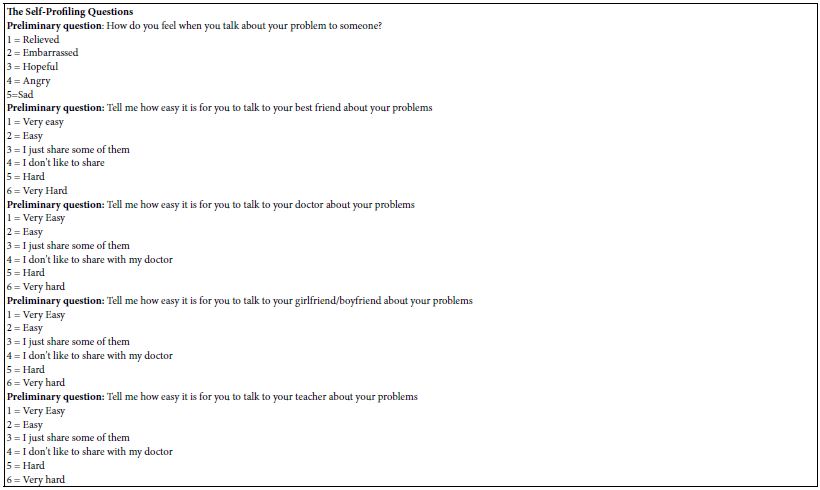
Creating Vignettes by Combining “Elements” (Answers)
Table 3 shows the four questions generated by the combination of the human researchers and AI. Under each question are the four answers. Each edited/polished question generated 15 answers. The researcher selected four answers, inserting the answers into the study after polishing them. As a consequence, the questions and answers in Table 4 are usually better than what would be generated even by an experienced professional. The user can run many iterations for questions and for answers, as well as polishing them to make them more precise.
Table 3: The “raw” material, comprising questions and answers
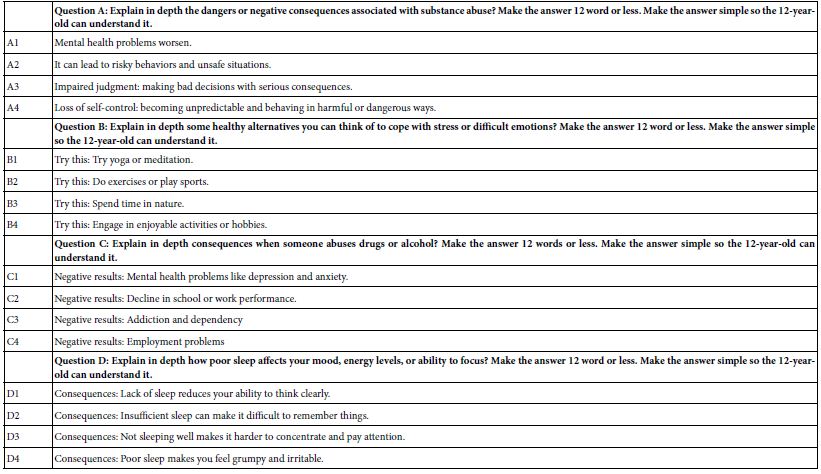
If this study was run as a typical study, then each of the 16 elements (A1-D4) would be presented as a single question, and the respondent (survey-taker) would evaluate each element independently. Of course, the researcher would randomize the order of the elements to reduce order bias. The biggest problem of these one-at-a-time evaluations is that they have no context—or at least the context may change depending upon the element.
The Experimental Design Underlying the Construction of the Vignettes
A better way might be to create combinations of these elements, doing so in a structured manner, so that the combinations, the vignettes, tell a story, albeit a story which has few connectives. Figure 2 shows an example of what the respondent might see.
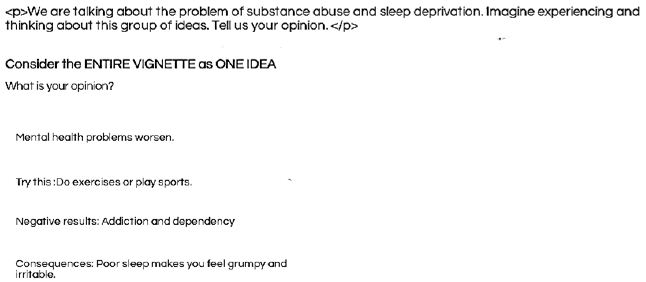
Figure 2: Example of what the respondent might see
Figure 2 looks disconnected but the respondent evaluating the vignette ends up with a sense of what is being communicated. After evaluating the first two or so vignettes, most respondents stop fidgeting and simply look at the vignette, and rate it on the scale shown in Table 4. It is important to note that Figure 1 does not attempt to present a polished paragraph to the respondent, one which reads well, with all the connectives. Although one might be tempted to “pretty up” the vignette, the reality is that the respondent has an easier time “grazing through” the sparse structure presented by the vignette. Less effort is required to identify the information in the vignette, and consequently the respondent can quickly evaluate each vignette. The happy consequence is that the respondent can go through the 24 vignettes quite quickly without incurring much fatigue.
The vignette is rated by the respondent on a simple 5-point scale shown in Table 4. The scale has two sides. The left side, the first part read, has the respondent decide whether the description in the vignette describes or does not describe them. The right-hand side has the respondent decide whether the description is typical or not typical. The rating question captures two aspects of the vignette, fit to the person, and typicality of the statements. These are not explained to the respondents. Most respondents end up having an intuitive sense of what the rating scale means. Their answers suggest that this intuitive sense of its meaning operates in the interview, as we will see below.
Table 4: Five-point rating scale
Experimental Design to Create Vignettes Which Represent “Slices of Life”
The Mind Genomics effort allows exploratory research rather than requiring confirmatory research. As such, the studies need not be based on theory, with the goal of confirming or disconfirming a hypothesis. Rather, the Mind Genomics studies end up encouraging exploration, intuition, and iteration. It is easy to react to combinations of messages, vignettes. We do it all day long, as we react at an almost automatic level to the world around us. Rather than asking ourselves “what is important about this vignette” or this particular situation, a task requiring thought, we simply react to what is around us. In colloquial terms we “go with the flow”.
By presenting respondents with combinations of messages, i.e., mixture of messages such as the answers (elements) shown in Table 3, we put the respondent into a more natural situation, one which resembles daily experience. All the respondent has to do is react. The structure of the vignette allows the researcher to present slices of life to the respondent, have the respondent rate the combinations of these slices of life, and when done, properly enables the researcher to numerically estimate the driving power of each of the 16 elements, even when the respondent themselves cannot do so. The experimental design will enable us to determine the degree to which each of the 16 elements fits the respondent. The key to success here is to present the “right” combinations of elements, the “right” slices of life.
The experimental design for Mind Genomics comprises one basic specified set of combinations, which is permitted into several hundred variations. Each variation differs in the specific combinations, but the mathematical structure is maintained, and the design is tested to ensure that it runs in the statistical analysis.
Fielding the Study with a Panel Provider (Or with One’s Own Patients)
Once those bookkeeping steps are done, the user contacts the panel provider—in this case Lucid Inc., a panel aggregator with access to tens of millions of people around the world. The actual panelists are the appropriate group, adolescents, who have agreed to participate in these studies. They receive rewards. To the authors, these respondents, these survey-takers, are totally anonymized. We have no idea who they are, no idea the reward that they get. Typically, to run 99 people as respondents requires approximately an hour or two from the time the email invitation is mailed out until the respondents complete the 3–4-minute survey There is a tremendous benefit of having a panel of paid, motivated people. Otherwise, it might take weeks and months to get the same number of respondents.
The panel provider is contacted, and the request is made for a specific age group, market, etc. The age range requested was 15 to 21 years old. No two respondents evaluated the same set of combinations. The result is that the study allowed us to explore a wide variety of combinations. As noted above, a key benefit is that there is no need to know the topic at the start of the project.
Transforming the Data and Creating Models Relating Elements to the Newly Transformed Binary Variable
Each rating generated a rating on the 5-point scale. A rating of 1, 2 or 3 was converted to 0. A rating of 4 or 5 was converted to 100. A vanishingly small random number was added to each newly created binary variable, the aforementioned 0 or 100. The reason for that is purely prophylactic. With the vanishingly small random number (<10- 2), one does not influence the analysis through ordinary least squares regression, but one guarantees that every one of the respondents will have variability in their newly created binary variables. The analysis is straightforward, whether we do it at the level of a group such as the total panel of 99 respondents, by groups defined by who the respondent claims to be based on the self-profiling classification, or even by individuals.
Recall that the dependent variable, the newly created binary variable, takes on 0 or 100, and each of the 16 elements has the value 0 when absent from the vignette, and 1 when present in the vignette. We create a simple equation of the form listed below:
Dependent variable= k1A1 + k2A2 + k3A3… k16D4. The magnitudes of the coefficients, k1 – k16, tells us the degree to which the appearance of the element in a vignette drive the respondent to say, “that is me.”
Recall that our respondents were just sitting there being exposed to a variety of messages embedded or combined in these vignettes. They had no idea what was going on. It was a “blooming, buzzing confusion” to them, in the words of Harvard psychologist William James. But throughout the effort, the respondents just simply sat there, grazed, as we said, through the vignettes, and assigned a number. Most of the adolescents, had we asked them, would have said they were guessing and would shrug their shoulders.
Table 5 shows the coefficients. The coefficients show the degree to which the element is perceived as saying “this is me.” We can consider the coefficients as conditional percentages. Thus, a coefficient of 10 means that 10% of the answers would be “that describes me”, were the element to be put into the vignette. From many of these studies, it would appear that a coefficient around 20 would be considered statistically significant. The rationale for this number is that the coefficients estimated with an additive constant show that a coefficient around 10 is statistically significant based upon a simple T test of coefficients. A model without an additive constant would show that same value of 10 to be 20. Thus, we create a simple operational rule that we should look for high coefficients of 21 or higher in models estimated without an additive constant, viz., models that are said to go through the origin.
With the following in mind, Table 5 suggests that no elements can be said to read our operational criterion of 21 or higher.
Table 5: Coefficients for the total panel for each of the 16 elements. Coefficients of 21 or higher denote very strong performing elements. The elements are presented in descending order of magnitude for each question.
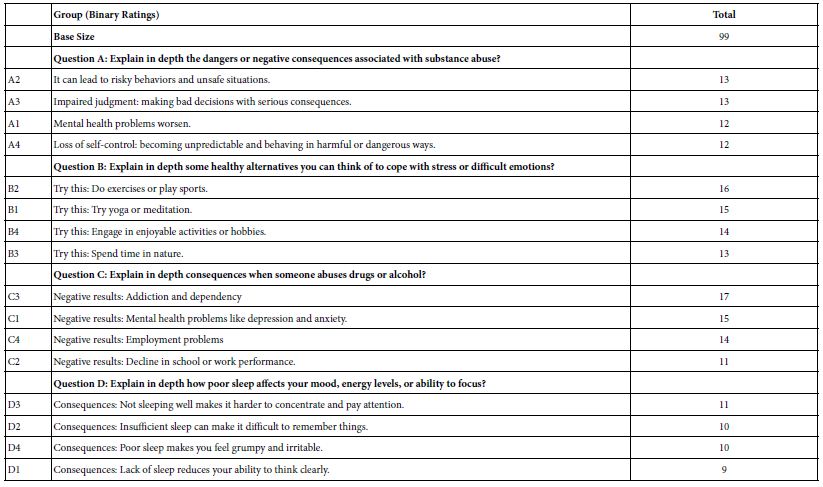
Mind-Sets: Moving to ‘Deducing how a Person Thinks’ by the Pattern of the Coefficients
Individuals vary in their preferences, coping mechanisms, and interactions with medical professionals. We are also aware that individuals may or may not be capable of identifying what they consider to be essential. With the aid of Mind Genomics, researchers are able to comprehend emergent groups of individuals whose decision-making processes adhere to distinct sets of criteria. Mind Genomics enables the researcher to identify different mind-sets. Mind-sets are defined as people thinking the same way about a topic. The important contribution of Mind Genomics is its ability to create these mind-sets at the level of the granular, at the level of the problem and its specificities. By having a bottom-up approach, one can create mind-sets for any specific problem, such as the one we are dealing with right now. One does not need mental gymnastics to translate macro mind-sets to specific topics, an issue often calling for creative re-thinking, with the mind-set data reworked and analyzed to produce an answer for a specific granular problem.
To create the mind-sets, one uses k-means clustering, a well- recognized statistical approach [22]. In our specific case of 16 elements, each respondent has 16 coefficients. We compute the distance between all pairs of the 99 respondents—a simple statistic. That statistic is called D, for distance, and is defined as (1 – Pearson correlation). The Pearson correlation quantifies the strength of the linear relation between two sets of data. A Pearson correlation of +1 means a perfect linear relation, whereas a Pearson correlation of -1 means a perfect inverse relation. Respondents with high values of D, near 2 are always in the same mind-set or cluster. Respondents with low values of D near 0 are generally in different mind-sets or clusters.
Once the respondents are assigned to either two clusters or mind- sets or separately three clusters or mind-sets, it is simple to create new groups for OLS regression, which we saw above for the Total Panel in Table 6. This time we run five regressions, first for the two mind-sets, and then for the three mind-sets.
Table 6 shows us the coefficients for the two mind-sets and then for the three mind-sets. The sum of the number of respondents is always 99. Each respondent fits into only one of the three mind- sets. There are empty cells in Table 6, corresponding to the elements whose coefficients are 5 or lower. Finally, Table 6 is sorted by the mind-sets, with all elements failing to score strongly in at least of the mind-sets put at the bottom of the Table. The mind-sets for the three- cluster segmentation by k-means make intuitive sense. The mind- sets are coherent, even though the entire analysis was done strictly by mathematical principles without any appeal whatsoever to the meaning of the elements. The mind-sets emerge quite clearly.
Table 6: How the elements performed when the 99 respondents were separately divided into two mind-sets, and then into three mind-sets respectively. Strong performing coefficients of 21 or higher are shaded. The table is sorted by the coefficients for the three mind-sets to highlight the differences among the mind-sets.
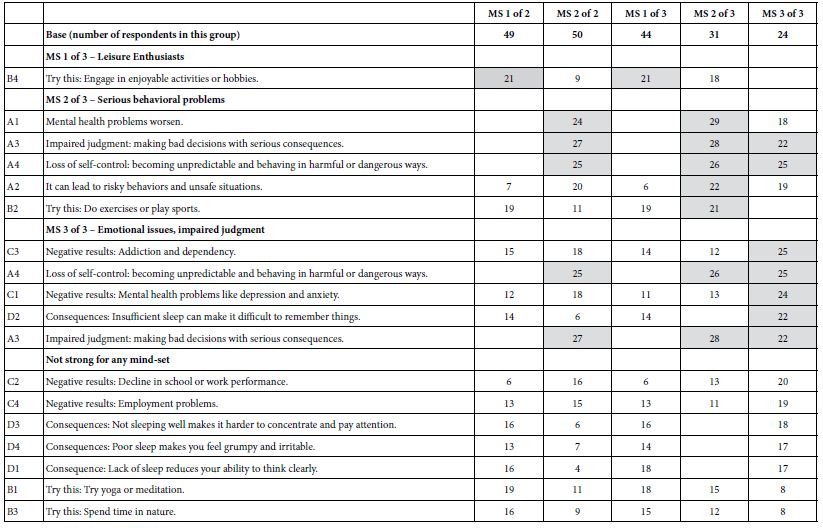
Table 7 shows the distribution of the selected answers for the three mind-sets, and for total panel. The distribution of the self-profiling answers by mind-set is unclear, in contrast to the clarity emerging from strong performing elements for each mind-set. There are some differences among the mind-sets, but the patterns are hard to discern, even though one might have expected to see more pronounced differences among the segments. It is this interpretability of mind-sets based upon very strong performing elements which enables Mind Genomics to create easy-to-understand “new knowledge.”
Table 7: The distribution of answers by mind-set and total for the self-profiling classification
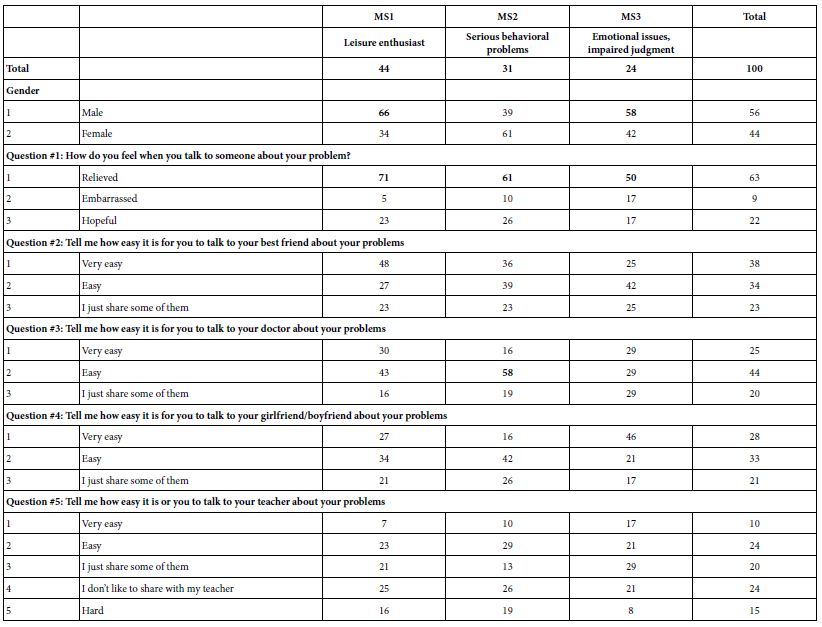
Putting AI to the Task of Adding Insights to the Mind-Sets
The last part of our analytics from the study itself is the interpretation of the findings through artificial intelligence. The automated re-analysis looks at the results from each mind-set, considering only those elements in the mind-set which generated a coefficient of 21 or higher. Through generative AI (ChatGPT 3.5) the AI answers a fixed set of questions as shown in Table 8. The results for each mind-set and to answer a variety of prompts. AI looks only at the strong performing elements, previously defined as elements which have coefficients of 21 or higher. Therefore, if a mind-set does not have any elements of 21 or higher, it does not appear in this AI analysis.
Table 8 shows the analysis. The prompts shown in Table 8 give a sense of some of the deeper information and insights that might emerge from the data. We might characterize the material in Table 8 as preliminary material for additional insights. Or, to take a phrase from the late Professor of Computer Science at Havard University, Anthony Gervin Oettinger, the material in Table 6 could be considered TACT, Technical Aids to Creative Thought [23].
Table 8: AI summarization and deeper analysis of the strong performing elements for each of the three mind-sets
Instructing AI to Provide a Simple Overview
Final analysis is based on the need to simplify the results. We can take all of the information provided by AI detailed analysis in Table 8 and summarize it through one simple query as shown in Table 9. The artificial intelligence does a very good job of taking the material that it itself has generated and summarizing it. The bottom of Table 9 shows the summarization in terms of what the mind-sets are, in what aspects they differ, and what innovations can AI suggest. The important thing here is that we can have artificial intelligence summarize and summarize more. Here is a situation where less is more.
Table 9: AI summarization of the results previously presented in Table 8
Discussion and Conclusions
Mind Genomics studies offer a unique approach to understanding human behavior and decision-making, unlike traditional questionnaires. By presenting respondents with descriptions and scenarios, researchers can tap into their instinctual responses and emotions, providing a more accurate representation of their feelings about a topic or product. This method often involves experiments where participants are presented with varying descriptions or messages, making it difficult for them to guess the “right” answer. This allows researchers to capture genuine gut-level reactions, revealing hidden insights that may not be apparent through traditional questioning methods.
Mind Genomics studies offer a practical and efficient way to gather data, as they focus on individuals’ reactions to descriptions or messages, allowing researchers to quickly compile large databases of knowledge. Dividing people into groups based on their responses to different messages and descriptions allows for a deeper understanding of how individuals process information and make decisions. By identifying patterns in how different groups respond, researchers can tailor messaging and communication strategies to better reach and engage specific audiences.
The study presented here is an example of the effort put in versus the output emerging. The time to create the questionnaires can be measured in hours, certainly less than half a day. The time to set up the study itself and launch was another hour or two. The time to obtain the fully analyzed data was an hour or two, with the fully analyzed data emerging in the form of a user-friendly Excel file. Finally, the time to summarize the data a second time through AI was less than an hour. Altogether, the project could have been completed within 24 hours. The time to write the paper is, of course, longer, at least for the current iteration of Mind Genomics, but that time will “collapse” in future iterations.
Acknowledgment
The authors would like to thank Vanessa Marie B. Arcenas, Angela Louise C. Aton, and Isabelle Porat for helping to produce this manuscript.
References
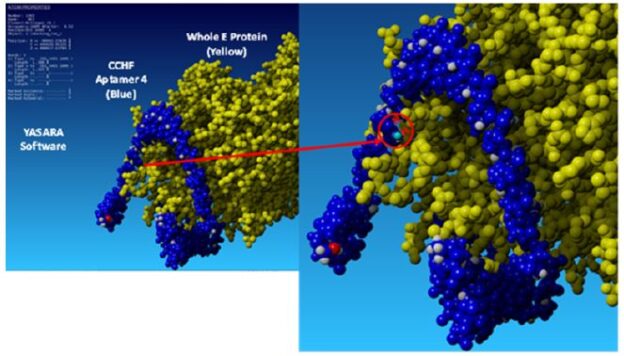
DOI: 10.31038/IDT.2024522
Abstract
The top five candidate DNA aptamer sequences developed and published previously by Bruno et al. (BMC Research Notes 5: 633, 2012) against Crimean- Congo Hemorrhagic Fever virus envelope glycoprotein precursor peptides were screened for plaque reduction activity against viable CCHF Oman virus in a BSL-4 laboratory. Statistically significant reductions in plaque forming unit (pfu) counts for CCHF using SW-13 cell cultures were obtained when pretreated with these aptamer DNA sequences which demonstrated much greater efficacy versus a polyadenine 49mer control oligonucleotide at the same concentrations.
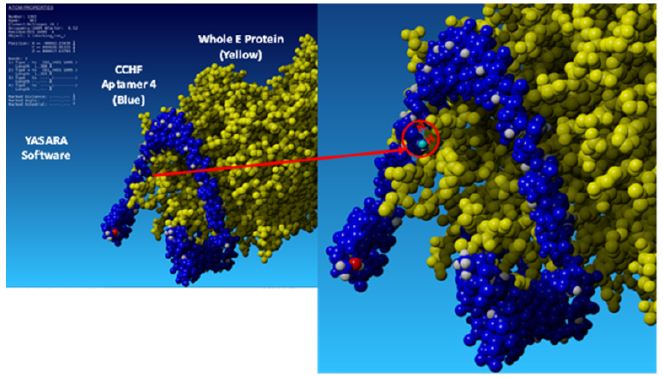
Keywords
Aptamer, Crimean-Congo hemorrhagic fever, Glycoprotein, Plaque, Virus
Introduction
Passive immunity for lethal hemorrhagic viruses such as Ebola has been demonstrated using convalescent antiserum [1-4]. Similarly, humanized monoclonal antibodies produced by Eli Lilly and Regeneron proved effective as passive immunity agents to protect patients suffering severe COVID during the pandemic [5].
Unfortunately, convalescent human antisera and humanized monoclonal antibodies are difficult and rather expensive to develop and mass produce. Nucleic acid aptamers present a much less expensive and more facile development alternative to humanized antibodies for industrial scale up of biologics to bind and block or inhibit progression of deadly viruses. A number of successful in vitro experiments exist reporting reductions in the number plaque forming units (pfu) or blockage of infections when viruses are pretreated with specific cognate aptamers and then added to cultures of mammalian host cells [6-9].
Crimean-Congo Hemorrhagic Fever (CCHF) virus is a widespread tick-borne virus member of the Nairoviridae with mortality reported as high as 30% in affected humans primarily across Europe and Africa [10]. As such, this virus is the subject of intense research [10-13]. While small molecule viral inhibitors have demonstrated significant efficacy against CCHF [12], humanized monoclonal antibodies are a prime target for the development of therapeutic medical countermeasures as well [10,13]. Human antibodies are known to synergistically neutralize the virus when bound to the envelope glycoprotein precursor [10]. In this work, one of the top 5 aptamers was shown to cause up to a 92.2% reduction in plaque forming units (pfu) and the other four aptamer DNA sequences also appear to exhibit significant efficacy as passive immunity pretreatment agents at least thus far in vitro.
Materials and Methods
Aptamer Development and DNA Sequencing
The SELEX aptamer development process against synthetic peptides derived from the CCHF envelope glycoprotein precursor (GenBank AHL45281.1) attached to magnetic microbeads was previously described by Bruno et al. [14]. All DNA aptamers or control oligonucleotides were synthesized by Integrated DNA Technologies (Coralville, IA).
SW-13 Plaque Reduction Assay
The traditional pfu reduction assay did not work well with Vero cells in initial experiments for unknown reasons. Therefore, the method of Paragas et al. [11] was used with human SW-13 adrenal cortex epithelial cells (ATCC CCL-105) except that crystal violet dye was used instead of neutral red. SW-13 cells were cultured in the BSL- 4 4 laboratory of the Texas Biomedical Research Institute (TBRI; San Antonio, TX, USA) to a confluent monolayer in Dulbecco’s minimum essential medium (DMEM) plus 10% fetal calf serum (FCS) in 6-well plates at 37˚C with 5% CO2. The culture medium was replaced with a 1:2,500 dilution of stock CCHF Oman strain in 0.5 ml of DMEM plus 2% FCS with or without the aptamer levels indicated in the figures (0 to 1,900 nanomoles of aptamers) for 60 min at 37˚C with gentle rocking. Culture medium was removed from the wells and 5 ml of DMEM plus 1% penicillin-streptomycin-L-glutamine mixture and 16% methylcellulose overlay was added to each well. Thereafter, 6-well plates were incubated in a humidified incubator at 37° with 5% CO2 for 7-8 days. At the end of this week-long incubation period, the DMEM and methylcellulose overlays were removed and 5 ml of room temperature 10% neutral buffered formalin was added to each well as a fixative. Plates were refrigerated between 2°C to 8°C overnight (12 h minimum). The following day, the formalin was removed and wells were washed with Phosphate Buffered Saline (PBS). Plaque counts were performed manually by two technicians in agreement about the numbers of pfus following staining of each well in 1 ml of crystal violet, followed by removal of the dye, a gentle rinse with fresh tap water and air drying. Plaque counts were subjected to ANOVA statistical testing and found to show statistically significant differences for all of the aptamer-pretreated groups versus the blanks and ploy-A controls with p values <0.01.
Results
Figure 1 shows the results of initial plaque reduction studies in which the means of triplicate well readings with 2X standard deviation bars appeared to produce a >50% reduction in the mean number of pfu per well from pretreatment of the Oman CCHF virus with 47 nmoles of aptamer 2 versus the >120 pfu for the blank control without any aptamer pretreatment additive. The blank in this initial experiment was comparable in number of pfu versus the poly-A 49mer control wells. The other aptamers in this first experiment did not reduce plaque formation >50%, but also demonstrated statistically significant reductions in plaque formation.
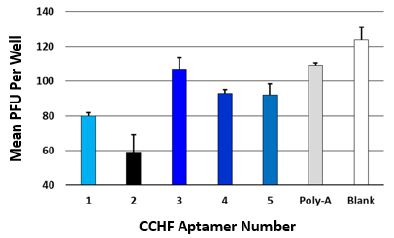
Figure 1: Initial plaque reduction screening experimental results for the top 5 aptamers and a poly-adenine 49mer all at 47 nmole of DNA per well except for the zero aptamer added blank. The averages and 2X standard deviation bars for 3 measurements are shown for each group.
In the second set of higher dose studies (Figure 2) with only aptamers 1 and 2, the aptamers exhibited a >90% reduction (up to 92.2% for aptamer 1 at 1,900 nmoles of aptamer) which was dose- dependent. Although the poly-A control exhibited some dose- dependent reduction in plaque formation as well in Figure 2, it was not nearly as effective at plaque reduction versus the more specific CCHF aptamers (~50% reduction versus >90%) at the 1,900 nmole concentration level.
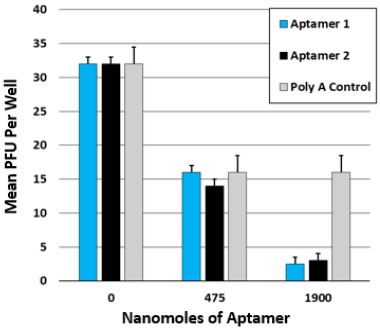
Figure 2: Dose-dependence plaque reduction results for aptamers 1 and 2 versus the poly-A 49mer and the blank group at the higher DNA concentrations indicated. The averages and 2X standard deviation bars for 3 measurements are shown for each group.
Discussion
Jalali et al. developed numerous aptamers against the conserved internal nucleoprotein (NP) of CCHF which produced excellent reagents for sensitive detection [15] of many different variants of lysed CCHF viruses. However, anti-NP aptamers are not very useful as therapeutics or prophylactics for passive immunity since they do not bind the viral surface or prevent viral fusion with the host cell [6]. Here the author describes the first in vitro testing of aptamers developed against the CCHF envelope glycoprotein precursor complex [14] which could inhibit or prevent CCHF viral fusion and host cell entry as demonstrated by the present data (Figures 1 and 2). The top 5 aptamer DNA sequences reported here (Table 1) were mostly generated against synthetic peptides in the Gc region of the CCHF envelope glycoprotein precursor [14] (amino acids 1041 through 1684) which form spikes on the viral surface involved in viral host cell entry [16]. The author has previously reported 3-D molecular models of the top 5 aptamers docked with the CCHF envelope glycoprotein precursor [17] which bear some resemblance to the precursor domain II regions bound by the antibodies Mishra et al. have reported [10] making the results reported here quite plausible.
Table 1: Aptamer DNA sequences.
|
Aptamer No. |
DNA Sequence 5’-3’ |
|
1 |
ACA GTT AGA GCT TGC CGT ATG CCT TTG TTA ACA TAA |
|
2 |
ACT AAC CGA ATG GCA GTT TCC CCC TTA TCC ATC TAT |
|
3 |
GGG ATA GGG TCT CGT GCT AGA TG |
|
4 |
CGC TGA AGC AAG ACA TTA TCG GGA CAT TGC CGT GA |
|
5 |
TGA CAC GCG TAC GGG TCC GGA CAT GTC ATA ACG GAC |
Conclusions
In this preliminary in vitro study, the top 5 aptamer candidates from Bruno et al.’s previous publication [14] demonstrated solid in vitro potential to act as passive immunity biologics. CCHF aptamers 1 and 2 in particular demonstrated strong dose dependence in vitro with >90% efficacy at the 1,900 nmole dose and deserve further research attention as possible alternatives to antibodies for the passive therapy of CCHF. The biggest issues with using aptamers in vivo is their small size making them subject to rapid kidney clearance and susceptibility to serum nucleases. However, aptamer pharmacokinetics can be greatly enhanced by covalent addition of heavier inert blocking agents such as polyethylene glycol or some proteins to the 3’ end [18-20].
Acknowledgments
Funding was provided by a U.S. Defense Department SBIR Contract No. W911SR22P0007. The author thanks Dr. Ricardo Carrion and Dr. Michal Gazi of the Texas Biomedical Research Institute (TBRI) in San Antonio, TX for maintaining the SW13 host cell cultures and conducting plaque assays in the BSL-4 laboratory.
References
A almost laughable to ponder upon where it all started and nearly grim and shameful when we realise as humans that we are reckless, careless, and foolish (Santosh Kalwar).
Looking back upon Covid’s entry into our lives, in the following narative we remove the wrapping of fraudulent news, to reveal how the spectre of a pandemic was used to coerce society into submission. To thank for all this we note the co-ordinated forces of a greedy pharmaceutical industry, shadowy governmental control plus an over-trusting population compliant in their own ruination. Not to mention the related pandemics of bankruptcies, depressions and suicides subsequently fermented. Ongoing are the results of ineffective vaccinations [1] causing more hospitalisations than the original virus (dones 2022); growing cases of autoimmunity [2]; nor is this yet over for the consequences are with us still [3,4]. Many vaccine effects are being covered-up by the term long-covid, where the guilty blame the disease rather than the longer term effects of vaccination. If this weren’t enough, and especially pertinent to modern times, are long-lasting effects steming from destruction of human rights and desecration of the human soul. As psychotherapists we see it in our clients plus those upon the streets. At the last, through complience, we all played a part in this all too real-life horror story. Many who previously believed in a more humane, just, compassionate and democratic society, now realise they were hood-winked into allowing all that’s best in us be destroyed. It’s not entirely our fault we fell for the prevailing chronicle, were we not primed to believe that politicians and medical experts, for all their personal flaws were trying to do the best they can? But to enhance compliance, governments used mass psychology and orchestrated fear [5], plus censored news [6] to keep us malleable. These ploys worked excellently and on far too many are working still. But now, finally, we perceive a wind of change blowing in the air (Mandavilli New York Times 202@. Indeed, the public’s belief in vaccination, since Covid, remains still at an all time low [7].
From the jig-saw of information arrayed below, drawn from multiple research studies, social and statistical surveys, news leaks and the accounts of ex-insiders at tbe time, we invite you to build your own picture, very different from the one officially broadcast by government, news media and big pharma – all guilty agencies who had a vested interest to supress the truth. Personally, although we would love to believe otherwise, reading between the lines it appears likely a group of powerful people regard the ordinary members of the public as surplus to their requirements. We, the public, don’t see through all this because evil makes us feel bad, sad, desturbed and deeply uncomfortable; so we resist accepting the world could work this way, for denial of unpleasant reality is part of our everyday coping mechanism. Nevertheless, uncomfortable facts must be faced if we are to awake fully to what’s before us. With Covid, even if we accept pharmaceutical bribes, commercial corruption and medical incompetence, there has to be another over-arching agenda for conspiracy of this proportion to thrive? How could blunders of such magnitude have been tolerated, condoned and succesful without large scale subterfuge sanctioned by our appointed guardians and rulers? There are few nurturing parents in our story, but many controlling and power-hungry ones. Are we then ‘Lost Children’? Regards the criminal reasons behind the Covid pandemic, the following are most widely circulated in public fokelore:
Sadly, there is some confirmation these were designed to work hand-in-hand.
Everyhing ofcourse remains unproven to the uninformed public eye, but disturbing enough data nevertheless keeps pumping out via litigation within law courts, whistle blowers jumping ship and courageous individuals like J. F. Kennedy Jr [8] for us to consider some pretty shocking accusations, which we survey under the following headings:
Suspicions of a Plan-demic…
Bribes and inflated figures of pandemic deaths…
Formally denied side-effects of vaccinations now emerging…. The ineffectiveness of vaccination…
Culpability of Big Pharma…
Draconian intentions of governments and WHO… Press and News Supression…
Over-estimation of vaccine take-up…
Under the above we share factual reportage prior to a brief synopsis, and at the close share a summary of our findings and personal impressions.
We hope the information herein will bring you upto speed and initiate you into the ranks of the ‘informed public’.
Looking back at our earlier reflective studies listing lethal side-effects and the ineffectiveness of vaccines, bribery in high places and corruption plus propoganderisation of the news [9,10] are all too sadly proving true. After reading this article you will have to hand sufficient data to make up your own mind.
What a story to tell the world how Coronavirus has become impotent and Triendless to reward ultra rich with more rights (Qamar RaTiq).
Suspicions ofa PlanQemic
“Each wave of terrorizing creates its effects more easily — añer a breathing spell — than the one that preceded it because people are still disturbed by their previous experience. Morality becomes lower and lower, and the psychological effects of each new propaganda campaign become strongep it reaches a public already soñened up” (doost Meerloo).
The Research and Evidential base:
In 2017 and 2018 every nation on earth started buying and selling millions upon millions of virus test kits labelled ‘Covid19 Test Kits’, you can still see this on the website of the World Integrated Trade Solution! How could so much be prepared and so many nations be in ‘the know’ so early on? What is more, only five months before the coronavirus outbreak WHO instructed all the nations to immediately prepare for an imminent World influenza pandemic. Similar foresight caused the Australian government to publish a manual for a coronavirus pandemic, a few months before it even surfaced.
Authors Comments: The conspiratorial nature of Covid was picked up early [14,15] and its man-made origins confirmed in records from The Patents Office January 2000 to June 2008, firstly addressing investigation of canine coronavirus gene uses on Jan 28th 2000) by Pfizer Inc (https.fff patents.justia.comfpatentf6372224);in the subsequent isolation of Corona virus from humans on April 12th 2004, also by Pfizer (https.fffpatents.justia.comfpatentf7220852);plus in the ongoing investigation into antiviral agents for the treatment, control and prevention of infections by coronaviruses on Apr 28th 2004 by Sequoia Pharmaceuticals Inc (https.fffpatents.justia.comfpatentf7151 163); finally, and most incriminating of all, by the investigation of amino acid sequences directed against envelope proteins of a virus and polypeptides for the treatment of viral diseases upon Jun Sth 2009 by Ablynx N.V (https.fff patents.justia.comfpatentf919378). It all becomes very difficult to believe that Coronavirus came from any other than a lab or that it was ever a new or novel strain. Sceptics amongst you please click any one of the above patent references to see for yourself. WHO, appear to have very powerful political ambitions on a world wide scale, not forgetting a principle funder in vaccine multimillionaire Bill Gates. Personal and comercial interests, we suggest, may have corrupted WHO’s stated purpose. We all tend to forget how large commercial enterprises have more wealth than many countries and wield much more power than most nation states, enabling their wealthy owners to force ‘their version of reality’ on us. Add to all this Patent Office records extending back to 2000, military involvement, leakage from public meetings and overlap of warnings from whistle-blowers, plus preparation of the public mind-set by pandemic films and dramas, and the notion of a Plan-demic, to our minds, is much more than merely circumstantial What is more, WHO in trying to push through Monkeypox as an International Emergency, even though US Government data agrees it is impossible to distinguish between Monkeypox, chickenpox and shingles, all appear highly invested in repeating their earlier Covid success! More tellingly, as the Covid-1 9 vaccination increases the risk of singles by a shocking 4925Oó (The Ezpose 2022Ç, they would appear to have set the conditions for a further pandemic? Unsurprisingly the main clusters of Monkeypox (vaccine induced shingles) are emerging in areas where Pfizer vaccinations predominated! Intriguingly, when I clicked on Dr. Reiner Fuellmich’s website and sites relating to his legal legal actions against Covid, most were rapidly blocked or otherwise made impossible to access! A host of attacks on the validity of his inquiry also litter the net. This is common practice I find when ‘the authorities’ and Google do not want discomforting facts to energe!
“Menticide (brainwashing) is an old crime against the human mind and spirit but systematized anew. It is an organized system of psychological intervention andjudicial perversion through which a fruling class can imprint their own opportunistic thoughts upon the minds of those they plan to use and destroy” (doost Meerloo).
Bribes and Inflated Figures
“We’ve seen repeated cases of corruption, and that is the second pandemic in many ways” (dohnathan Cushing Transparany International Global Health Team)..
The Research and Evidential base:
One of the informants for our earlier articles was an Orthodox Priest who was asked to confirm a Covid death for a road traffic accident victim. He refused and went public on TV! Also consider, death from any cause within 28 days of a positive test for SARS-CoV-2 was recorded in several countries as a “Covid death”. With case-rates and Covid deaths highest among the Triple Vaccinated many governments are now asking where did the ‘Science’ of the pandemic go wrong? The hype and the statistical facts don’t add up!
There are literally scores of viruses, even common cold viruses, which infect the human airway in elderly and infirm people to give rise to severe illness. But these appear to have been intentionally or accidently re-coded as Covid-19 – how else can we account for the disappearance of the common cold and seasonal influenzer during our Covid years? Least we forget about prior conditions contributing to Covid deaths, of 29,135 Covid deaths registered in Romania until April 2021 (Statistica, 2021), only 227 were admitted by the Minister of Health to have died of Covid alone, without severe aggravating prior conditions! Thus proving a massive exaggeration of figures to the tune of 28,908 excess deaths! A similar over estimation of deaths was similarly reported in the UK and USA. Please ask yourself why was it so important to lie to us by official bodies?
Authors Comments. Obviously, there was a concerted effort from many quarters to inflate and escalate Covid figures to glorify the pandemics potency. Bribes were also paid to this end and health policies modified. Why was it important for us to be deceived? We mentioned in an earlier article that if you once test positive in the UK, you can end up being registered ‘Covid positive for life’, to later be attributed ‘a Covid death’ statistically. In this way viral deaths soar frighteningly and swell existing figures. Not surprisingly, in this fear inducing context, no figures for recovery from Covid were ever circulated thus magnifying its potential as an imagined death sentence in public eyes. As we have evidence of the UK weaponising fear [17], we shouldn’t be too surprised by this petty dramatisation. More peturbingly, is money the main reason for all this? Or is there something more sinister afoot? De- populatuon perhaps? So does Covid and its vaccination shade into this? The argument politicians like Kissenger [18] and philosophers such as Yuval Noah Harari [19] espouse, is “we need to depopulate the planet out of necessity or we won’t survive as a species”. It’s an old cover story. Evil always believes itself to be doing good. Over-population and the burden of an aging populance have been live issues for many decades. The older we get the more pressure we put on state pensions, health services and public spending. Should a man of my age of 76 in light of such logic then be let live?
°The masses have never thirsted añer truth. They turn aside from evidence that is not to their taste, preferring to deity error, it error seduce them. Whoever can supply them with illusions is easily their master; whoever attempts to destroy their illusions is always their victim”(Gustav Le Bon)
Formally Denied Side-effects of Vaccinations Now Emerging
“Maybe it is not COVID-19, but the government should come out and explain what’s causing these deaths. We don’t have the freedom or the Tacts to say iT it is COVID-19” (AdoIT Mkono).
The Research and Evidential base:
Authors Comments: Panic appears to be growing in many governments as the Fully Vaccinated have a higher Covid Hospitalisation-Rate than the Unvaccinated. Growing figures also testify to the inefficiency of masks, lockdowns, vaccinations, Covid passports, thus opening the door for litigation! The more so as AIDS; as viral authorities predicted is still showing-up as a fact of full vaccination. Is it not time we stopped calling the pandemic of heart attacks in the young ‘Sudden Death Syndrome’ and give them their real name, ‘Death by Covid Vaccination’? This is after all the true cause, as most governments well know. But why should governments support the truth when it means political suicide? Understandably, medical doctors who supported vaccination and advised their community accordingly, are also reluctant to share statistics which make clear that Vaccinated Young Adults have a 92Oó higher mortality rate (per 1 00,000) than Unvaccinated Young Adults. Combine all this with ambulance call-outs for heart illness having doubled since the beginning of the Covid-1 9 Vaccination Campaign, and orthodox medicine, it would appear, has hung itself by its own petard! But the wall is crumbling, for even a World Health Organization study [23] concludes risk of suffering Serious Injury due to COVID Vaccination is 339Oó higher than the risk was of being hospitalised with COVID-1 9! It is interesting timing for WHO to now expose the inefficiency of vaccines, the very things they pushed – are they changing sides in order to survive the incoming tide turning against them? When WHO and the BMJ agree on a point, it can’t be ignored. Will Big Pharma do the same and fess up we wonder? Insurance companies, who have no reason to lie, in reports from 201 9 (the last normal year before the pandemic) to 2020 (the year of the Covid-1 9 virus) report an increase in Group Death Benefits of only 9 percent; but group death benefits in 2021 when vaccine was introduced, increased 164 percent. Indeed the precise numbers for Group Death Benefits taken from Lincoln National’s annual statements for these years are 201 9: 8500,888,808; 2020: 8547,940,260; 2021: 81,445,350,949 [24]. Please read these figures again. When commerce is God, all else, morals and Christain virtues it seems become expendable. There is also another area we need consider, assisted deaths. It is now being suggested in several quarters, somewhat cynically, that we gave up two years of our life because Midazolam was used prematurely to end the lives of thousands of over 70’s in care homes (Telegraph 2021), though relatives were told their next of kin had died of Covid-1 9. Legalised murder no less! Looking at the bigger picture, we were conned by health and government alike into believing Covid was so very very lethal! So the alternative motive? Euthanasia or an experiment in mass population control? Such notions as these we deemed unbelievable prior to Covid, but many now believe they are are worth considering – so low is civic trust! Lastly, regarding the prospect of vaccine induced AIDS, this was prophesied by an official German Government study in January 2022 [25], it came right on cue explaining many of the associated peaks of illness earlier described and is with us still. The amazing thing is, some people thrive following triple vaccination, so research is acutely needed to identify catalysts that counter the effects of vaccination; but here’s the catch, grants for remedial research can’t be allocated until vaccine damage is openly accepted – and there remain forces at work hell bent on preventing this!
“Logic can be met with logic, while illogic cannot – it confuses those who think straight. The Big Lie and monotonously repeated nonsense have more emotional appeal… than logic and reason. While the fpeople are still searching for a reasonable counter-argument to the Tirst lie, the totalitarians can assault fthemj with another” (doost Meerloo).
The Ineffectiveness of Vaccination
“Success belongs to those who accept mistakes as stepping stones” (Hermann d Steinherr)
The Research and Evidential base:
Authors Comments: We wish to appologise to our readers that some of our quotes cannot be fully referenced, especially in this section, as they were taken off the website before we had time to formally record them! When we returned to many sites challenging vaccination, we also found these had also mysteriously disappeared, and in their place we found a plethora of pro-vaccination messages rubbishing earlier claims. Having said this, enough sites remain to support that the fully Vaccinated are nearly 3 times more likely to die of Covid-1 9 than the Unvaccinated. How do you feel about having been coned into considering, if not indeed having a proven useless Covid injection with life threatening side-effects? Not forgetting ever more follow up boosters where you are asked to willingly accept an even greater risk to your health? We personally know of too many local cases where vaccination has heralded cerebral changes, cardio-vascular problems and autoimmune reactions, for us to doubt the above statistics. Small blood vessels in the eye, brain and heart seem especially to suffer. As we speak ever more variants are being conjured up and we”re being offered further vaccinations for vaccination induced diseases! A brilliant commercial plan for Big Pharma yet again! It is no small wonder that statistics are causing government concern, with the fully vaccinated, on the international scene still having a higher Covid hospitalisation rate than the unvaccinated, and the triple vaccinated now up to 5 times more likely to be infected with Covid-1 9 than the unvaccinated. But this is small wonder when vaccine effectiveness has fallen as low as minus 391 Oó! A recent scientific study confirmed COVID vaccines were causing severe Autoimmune-Hepatitis days after WHO issued a ‘Global Alert’ about new Severe Hepatitis strain among Children! Was WHO offering a cover story for vaccine side effect? And why when we Google for ‘Covid vaccination side effects’ do we get sore arms and headaches but nothing about serious side effects?
Governments, through mis-information fostered by Big Pharma have damaged those they were appointed to protect, yet so many of us still turn a blind eye? An extensive wide ranging study by several universites, plus the editor of the BMJ, report via the Social Science Research Network (SSRN), have reported that Covid vaccines are more likely to put you in hospital than keep you out [26]. We rest our case.
“Totalitarianism is man’s escape from the fearful realities of Iife into the virtual womb of the leaders. The individual’s actions are directed from this womb — from the inner sanctum man need no longer assume responsibility for his own Iite. The order and logic of the prenatal world reign. There is peace and silence, the peace of utter submission” (doost Meerloo,).
Culpability oF Big Pharma…
“Medicine being a compendium of the successive and contradictory mistakes of medical practitioners, when we summon the wisest of them to our aid, the chances are that we may be relying on a scientific truth the error of which will be recognized in a few years time” (Marcel Proust).
The Research and Evidential base:
Authors Comments : Big Pharma got itself quite a business plan! Working first with WHO to dilute the definition of ‘pandemic’; spending billions cosying-up medico-political support via free lunches and cash incentives; pouring money into viral research and when a suitable candidate came along declaring it with WHO’S blessing a ’pandemic’. They even committed the worst virological sin of all – vaccinating at the height of a pandemic forcing the virus to mutate to survive! Even first year student nurses know this is dangerous and eeckless! How did they bring in previously prepared vaccinations? By coercing goverments into signing-off their culpability for side-effects, thus allowing them to offer lame experimental vaccinations over-and-above existing legal safeguards and law. And when these untested vaccines produced varients such as Alpha, Amicron, Delta, and Monkeypox they sought to vaccinate againt these also! Grand plan don’t you think? Commercially sound, ethically barren. We must also note the concerted effort to suppress the following alternative treatments: HYDROXYCHLOROQUINE – Used by tens of thousands of physicians worldwide, FDA approved for over 65 years, hydroxychloroquine is considered a safe and virtually 100Oó effective medicine for Covid-1 9. BUDESONIDE – Discovered as a 100Oó effective cure for Covid-1 9 by Dr. Richard Bartlett, who saw over 500 covid patients recover after treating them with this asthma medicine. As his randomised control study proved. IVERMECTIN – Dr Pierre Kory treated numerous corona patients to discover that Ivermectin is a true miracle drug for Covid1 9. A more recent study by ten medical experts reviewed the evidence and concluded that Ivermectin both prevents and cures Covid-1 9. CHLORINE DIOXIDE – Biophysicist Andreas Kalcker was reported as bringing down the covid daily death rate in Bolívia from 1 00 deaths a day to almost zero, with this substance he has researched for over 13 years. Even now alternative treatments to vaccination are being rubbished upon the net. So why were alternative treatments not investigated more? Rather than quashed so quickly – follow the money line and ask who has most to gain? It all boils down, yet again, to money before human lives! And when ‘ mass formation’ cum collective hysteria was cited to explain the populations sheep-like behaviour, Gates and big pharma likewise rubbished the work of all scholars associated with mass hysteria from Gustave le Bon to Mattias Desmet. Bill Gates even put out media message to say it was a made up term with no value! From Nazies to Covid and back again! Lies from the powerful masquerade as shining truths.
The world is in the grips of mass formation—a dangerous, collective type of hypnosis—as we bear witness to loneliness, free-floating anxiety, and fear giving way to censorship, loss of privacy, and surrendered freedoms (Mattias Desmet).
Draconian Intentions of Governments and WHO
“The worrying issue is that all levels of government — not only Federal — are abusing the emergency decree to continue with direct awards without any restrictions” (Eduardo Bohârquez director of Transparency International).
The Research and Evidential Base
Authors Comments. The handling of Covid 19 has been cited as preparation for ‘Agenda 2030’, a UN initiative whose shadow intentions, if not its press hand-out, have been said to support a system of total, worldwide centralization of power, influencing everything from governments to free market economy, with the goal of full centralization to allow a handful of people to micro-manage every aspect of trade and business. WHO ardently backs Agenda 2030 and seems to be working towards a like goal. Covid is seen by some as an initial experiment serving the creation of this economic empire, where a concept called the “sharing economy” is created in which people own less property and have less privacy. Sounds far fetched, but a lot of material is on the net re banking reset geared towards ensuring the security of existing power holders! Worryingly, Obama, Zuckerberg and Gates have acknowledged adopting the philosophy of Yuval Noah Harari, a Jewish philosopher who states the role of culture is to forbid (Harari 2018) He acknowledges that if governments and corporations succeed in hacking the human animal the easiest people to manipulate will be those “who believe in free will”. Harari observes: “We now have the technology to hack humanity and let everyone think and feel what we want. Tyrants always wanted to do thai but now for the first time we have the ability to do this. We will eradicate faith in God, end all free will, and make sure that humans think exactly what we want them to think”. His book,”21 Thoughts for the 21 st Century,” which supports the political lobby for population reduction was promoted extensively by Bill Gates, who wrote a foreword upon the cover. More desturbing is that Harari is being promoted massively by the United Nations, the World Economic Forum, the World Health Organization – hence Agenda 2030 cited above. The spectre of de-population seemingly won’t go away. 5G, was cited earlier as linked to depopulation, was referred to by the president of Chile who threatened on national TV: “5G will not only read your thoughts, it will inseW thoughts and feelings. And we will make sure it reaches every home in the country.”’What a charming fellow – not! The Jury is out whether this is rhetoric or fact. The military, Big Tech and various governments have all been implemented as playing their part in 2030, now said to be in its final stages. Ten years ago we would have laughed at such notions – now we seriously consider them. Lastly we must with great sadness note that many sources, both governmental and pharmaceutical, are now suspecting that the Covid-19 vaccination may lead to mass depopulation. These suspicions, further backed up by mounting evidence from research studies and confidential Pfizer documents the U.S. Food & Drug Administration has released by court order, confirm a similar scenario.
One can but remember a Kessinger memo leaked out from the US Government in 2014 seriously considering depopulation as a viable way forward! Something unimaginable was seemingly being held in mind prior to Covid.
“Modern technology teaches man to take for granted the world he is looking at; he takes no time to retreat and reflect. Technology lures him on, dropping him into its wheels and movements. No rest no meditation, no reflection, no conversation — the senses are continually overloaded with stimuli. Man doesn’t learn to question his world anymore; the screen of fears him answers-ready-made” (doost Meerloo).
Press and News Supression…
*‘It is a Turore of disinformation and attacks — one in which credible journalists are subjected to online violence with impunity; where Tacts wither and democracies teeter”(dulie Posetti).
The Research and Evidential base:
The new black is obvously white! And truth is as ever decreed by those in power – are they not the ones to re-write history?
Authors Comments: The UK government, while professing to be democratic, uses public money to bribe a publically funded news media – the BBC, to fear bombard the public with government approved propaganda furthering its own political agenda (HART 2021)/. They are also reported as paying experts in mass psychological manipulation to preserve their standpoint as the one and only way (Dodsworth 2021). There really is no room left for us to doubt press censorship. We personally have lost all faith in politicians and governments and consider the national news services a sick joke. Journalists themselves are likewise very concerned [33]. In terms of the impact COVID-1 9 is having on media there has been a renewed closure of civil space, especially in more authoritarian countries. In Egypt, for instance, there are new laws to suppress reporting, and leading journalists have been arrested. In Myanmar, under the cloak of COVID-1 9/fake news, independent media has been shut down (Ibid). All of which is deeply worrying. Sadly, the UK can’t report its own governmental censorship or abuses of the home press for fear of governmental and Ofcom fines and reprisals! Hypocritical or what?
“The social transformation that unfolds under totalitarianism is built upon, and sustained by, delusions. For only deluded men and women regress to the childlike status of obedient and submissive subjects and hand over complete control of their lives to politicians and bureaucrats” (doost Meerloo).
Over-estimation of Vaccine Take-up
Mis-information is a virus unto itselT (Brianna Keilar).
The Research and Evidential base:
Authors Comments
In an earlier report we mentioned if you once test positive in the UK you can end up being registered ’Covid positive for life’, to sooner or later be attributed ’a Covid death’! Such ploys as this cause Covid deaths to soar frighteningly. One could easily be led to believe no one recovers from Covid! But almost all recover unless with serious medical pre-conditions, or if incubated or otherwise harmed by medical intervention. So much stistical subterfuge! Hopefully the recent refusal of vaccination is evidence of the masses waking up to the harm inflicted upon us? But sometimes it’s much harder to admit our mistakes than to make them – so this may take some time!
“But the order of a totalitarian world is a pathological order. By enforcing a strict conformity, and requiring a blind obedience from the citizenry, totalitarianism rids the world of the spontaneity that produces many of Iife’s joys and the creativity that drives society forward” (doost Meerloo).[34-50]
Concluding Summary
“Historically, pandemics have forced humans to break with the past and imagine their world anew. This one is no different. It is a portal, a gateway between one world and the next. We can choose to walk through i¿ dragging the carcasses of our prejudice and hatred, our avarice, our data banks and dead ideas, our dead rivers and smoky skies behind us. Or we can walk through lightly, with little luggage, ready to imagine another world. And ready to fight for it” (Arundhati Roy).
When you join up the dots of the information we have arrayed before you where does your reasoning take you?
For ourselves, reluctantly, we believe there is just too much data coming out to believe that Covid was a simple virus. Military path lab involvenent and patent office records, plus WHO macinations produce too much evidence of fore-knowledge and fore-preparation from such wide ranging sources, to suggest, Covid was manufactured and planned, and on a massive co-ordinated scale. Mass corruption from state governments and State suppliers of health, pharmaceuticals and WHO are all evidenced as keeping it going. Bribes of a very high calibre oiled the workings and governments silenced the press and TV. Though in the UK the public facing puppets kept it going almost seamlessly, here, in our home-base of Romania we saw through the cracks much sooner, as public facing systems were more flakey and politicians were thankfully less organised than elsewhere.
We wish there was more data that a straight forward virus was merely mis-handled and more proof that our conclusions are faulty. For there are no winners here! But such reliable sources as the British Medical Journal, Data Science Association, Health Advisory and Recovery Team, International Freedom of Expression Exchange, Social Science Research Network, UK Office for National Statistics, UK Statistics Authority and far too many university led research studies, plus records of The Patents Office back-up our findings. Deep down, we sincerely wish we were wrong, but we can’t find the verification for it. So we end up believing governments, spurred on by Covid, have ridden rough-shod over common good, human dignity and human rights, while exiziling humanitarianism, research and empirical observation to the wastelands. Consequently personal liberty has been restricted, justice and rationality suspended, and social responsibility all but forgot. The very things that make life the more enjoyable. In this light, as humanists, we feel morally compelled to write, as to sit idly by as moral cowards is not a self respecting option. Is silence during public atrocity not complience?
It took us some time to catch up with the Covid farce. Sinziana comes from a medical family and my first career was as a nurse and nurse teacher. Until Covid came along we both believed in vaccination. We were reluctant dissenters though ardent researchers, so research won us over in the end. In our earlier articles we were genuinely perplexed, now we have lost faith in government and medicine in general. At the last, the vaccinated are the ones paying the price. Prospectively, we fear they have a life vexed by possible auto-immunity and cardio-vacular problems ahead, not to mention a shortened life expectancy. This is a very hard reality to face, and we are past anger on the issue.
We know most people feed off the telly and news papers for their shot of truth, taking all other sources as suspect, so we will likely be enthroned further by writing this article as conspiracy theorists. But please, at least, survey the headlines of the references below to glean something of what propoganderised news is denying you. Feel free to shoot us down as the messangers but we beg of you – awake!
“It’s easier to fool people than to convince them that they have been Tooled” (Mark Twain).
References
Abstract
Tissue engineering technology has demonstrated significant potential for tissue repair, enabling the restoration of damaged tissues or organs in terms of both structure and function. The utilization of digital light processing (DLP)-based 3D printing has gained significant traction in tissue repair due to its remarkable advantages in terms of printing resolution and efficiency, as well as mild printing conditions. Gelatin methacryloyl (GelMA) has emerged as a commonly utilized ink for DLP-based 3D printing due to its unique photoinduced crosslinking properties, controllable mechanical properties, degradation characteristics, and excellent biocompatibility. This paper primarily presents state-of-the-art technologies and applications involving DLP- based 3D printed GelMA constructs for bone repair, skin repair, and peripheral nerve repair. It aims to highlight the promising potential of DLP-based 3D printed GelMA constructs in regenerative medicine.
Keywords
Digital light processing, 3D printing, Gelatin methacryloyl, Tissue repair
Introduction
The repair and functional reconstruction of tissue and organ defects pose significant challenges in the field of regenerative medicine. Currently, autologous or heterologous tissue and organ transplantation are the most commonly used treatments; however, they are hindered by limitations such as traumatic trauma treatment, insufficient donor availability, and immune rejection. Tissue engineering research focuses on three core elements: cells, biomaterials, and tissue construction technology [1,2]. The realization of tissue and organ reconstruction relies on obtaining an adequate number of seed cells with specific biological activities, combining them with suitable biological scaffold materials, and employing precise construction techniques to create personalized physiological structures and functional organs or tissues in vitro. Therefore, personalized tissue engineering holds immense potential for advancements in the field of tissue repair and replacement. 3D printing technology offers rapid personalized manufacturing capabilities that can greatly contribute to tissue repair [3-5].Digital light processing (DLP)-based 3D printing utilizes a digital microscope device (DMD) to project images onto photosensitive liquid resin or bioink through surface exposure, enabling layer-by-layer solidification for printing purposes. DLP- based 3D printing technology enables the creation of personalized biological structures with precisely designable geometries, effectively bridging the structural disparities between engineered and natural tissues. It has found extensive applications in fabricating constructs such as artificial skin, bone implants, and nerve conduits. In comparison to other printing methods such as extruded and inkjet 3D printing, DLP-based 3D printing offers significant advantages in terms of resolution, efficiency, and working conditions. Its non-direct contact approach provides relatively gentle conditions for cell printing.
The development and application of printing ink is an important research connotation of dlp-based 3D printing technology. Conducting research and developing innovative bioinks that strike a balance between printability, biocompatibility, and mechanical performance is crucial for the advancement of bioprinting applications. GelMA, a photocrosslinkable hydrogel derived from gelatin modified with methacrylic anhydride, exhibits exceptional biocompatibility, visible light curing capabilities, and controllable mechanical properties, rendering it a versatile ink for printing purposes. During the printing process, GelMA is typically combined with cells, growth factors, and other bioactive substances to leverage 3D printing in fabricating tissue engineering models with specific structures and functionalities. This paper primarily presents state-of-the-art technologies and applications involving DLP-based 3D printed GelMA constructs for bone repair, skin repair, and peripheral nerve repair (Figure 1).
Figure 1: Application of DLP printing technology in tissue repair
DLP-Based 3D Printing
Based on the continuous application of DLP-based 3D printing in tissue engineering, higher printing accuracy and faster printing speed are required for practical implementation of DLP technology. Constant advancements in new printing technologies based on DLP technology are being made [6,7].
John et al. have designed a rapid continuous printing process based on DLP technology, which creates an oxygen-containing “dead zone” between the forming section and liquid precursors to enable continuous exposure printing and significantly enhance DLP printing speed [8]. Callum et al. have developed a dynamic interface printing technique based on DLP that utilizes sound modulation and restricted gas-liquid boundaries to generate centimeter-scale 3D structures within tens of seconds. This approach does not require complex feedback systems, specialized chemical reagents, or intricate optical elements while maintaining rapid printing speed and exhibiting immense potential for high-resolution and biocompatible applications {Vidler, 2024 #6}. Brett et al., on the other hand, have developed Computed Axial Lithographic (CAL) printing technology based on DLP where materials can achieve volumetric polymerization of arbitrary geometric shapes. Compared to traditional layer-by-layer printing methods, CAL’s polymerization approach eliminates the need for support structures, is suitable for high-viscosity fluids as well as solids, and significantly enhances print speed{Kelly, 2019 #4}. Regehly et al. employed dual-color photopolymerization in DLP-based 3D printing, wherein photoswitchable photoinitiators were developed. This technique utilizes two intersecting light beams of different wavelengths to achieve complete object fabrication by inducing localized polymerization within a confined monomer volume, resulting in enhanced speed and resolution for 3D printing. Recent advancements in DLP-based 3D printing have primarily focused on improving print speed, with various novel techniques offering additional technological approaches for bioprinting applications. In the realm of biological 3D printing technology, the choice of bioink plays a crucial role; currently, commonly utilized bioinks include alginate series bioinks, collagen bioinks, and GelMA materials [9]. CAL technologies introduce a printing paradigm shift because they are able to create entire objects at a time, rather than by adding basic building blocks in sequence. The study of Bernal et al. introduced the concept of volume bioprinting (VBP), which can manufacture an entire carrier cell structure of arbitrary size and structure in a time range of several seconds to tens of seconds. Using GelMA as printing material, bone scaffold and meniscus containing were constructed by volume printing technology. The rapid manufacturing advantage of CAL technology in bioprinting is verified [10].
GelMA
GelMA exhibits excellent biocompatibility and promotes cell adhesion and proliferation through its biological motifs, particularly the RGD sequences on gelatin molecules. The crosslinked network structure of GelMA not only serves as a scaffold for cells but also facilitates material exchange{Yue, 2015 #56} [11-13]. By adjusting the substitution degree of MA in GelMA, its mechanical properties such as viscosity, compressive strength, and tensile strength can be tailored to meet specific printing requirements. Additionally, for tissue repair applications, it is crucial that bioprinted structures are biodegradable. GelMA’s matrix metalloproteinase (MMP) site allows it to serve as an enzymatic degradation site recognized by injured organism cells [14]. As native cells fill the GelMA construct, they initiate its degradation while simultaneously repairing the area with their own cells to achieve tissue regeneration. With its exceptional biocompatibility, tunable mechanical properties, degradability, and photoinduced cross- linking capability, GelMA holds great potential for personalized and customized engineered living tissues or scaffolds for tissue repair [15- 18].
Applications of DLP-based 3D Printing Using GelMA
Tissue engineering aims to enhance or replace biological functions for the purpose of repairing damaged tissues and organs. DLP bioprinting enables precise distribution of cells, materials, and biological factors, offering a novel approach for fabricating artificial tissues. DLP-based 3D printing exhibits remarkable advantages in terms of resolution, efficiency, and operational conditions; moreover, its indirect contact formation method provides relatively mild conditions for cell printing. GelMA and its composite hydrogel system are exceptional biomaterials for tissue engineering due to their excellent biocompatibility, tunable mechanical properties, and degradability. The utilization of GelMA in DLP-based 3D printing holds great promise in various tissue repair applications including bone regeneration, skin reconstruction, as well as peripheral nerve restoration.
Bone Repair
The incidence of bone defects caused by trauma, infection, tumors, and congenital or metabolic diseases has significantly increased. These defects often result in functional disabilities and deformities, posing a clinical challenge for treatment. Traditional autologous and allogeneic bone transplantation methods have several limitations including inadequate tissue supply, donor site damage, immune rejection risks, and potential infections. Therefore, the development of new strategies for bone defect repair has become an urgent problem to be addressed [19]. On one hand, 3D printing enables personalized customization for individualized precision treatment; on the other hand, it reduces the cost associated with large-scale preparation [20]. The architecture of the bone repair scaffold can affect the effect of cell-induced regeneration of damaged bone. Song et al. combined bionic microporous GelMA/SilMA with hydroxyapatite (HAp) to prepare a bionic microporous GelMA/SilMA/HAp ink. By utilizing DLP-based 3D printing, they fabricated layered bionic microporous GelMA/SilMA/HAp (M-GSH) scaffolds. Animal experiments demonstrated that these bionic microporous scaffolds significantly enhanced tissue integration and bone regeneration after 12 weeks of implantation. Tissue engineering scaffolds for repair require not only adequate structural stability, but also good biocompatibility [21]. Gao et al. successfully developed GelMA/PEGDA/F127DA composite hydrogel scaffolds by DLP-based 3D printing, which not only facilitated cell adhesion and proliferation but also effectively promoted osteogenic differentiation of mesenchymal stem cells in osteogenic inductive environments. Intramembranous ossification and endochondral ossification are two ways of bone regeneration, in which hypoxia-inducing factor-1 α (HIF-1 α) signaling pathway can promote endochondral ossification and angiogenesis [22]. Gao et al. DLP-based 3D printing to fabricate structurally robust and biocompatible GelMA/PMAA hydrogel scaffolds, capable of chelating iron ions and continuously activating the hypoxia-inducible factor- 1α (HIF-1α) signaling pathway, thereby promoting endochondral ossification and angiogenesis processes as well as late-stage vascular formation and bone remodeling. The balance between cell survival environment and hydrogel cross-linking density is crucial for light sensitivity to achieve high intensity and good cell viability in cell- borne cartilage repair materials [23]. Shen et al., employing GelMA/ SG as bioink, created high-precision networked DLP printed scaffolds with superior shape retention compared to GelMA alone. In vitro experiments exhibited significant chondrocyte proliferation, while ectopic cartilage formation was evaluated by subcutaneously implanting the GelMA/SG scaffolds in nude mice. The utilization of these scaffold materials along with their manufacturing strategy offers potential solutions for future clinical challenges in cartilage repair. “Sr” is a potent anti-osteoporotic agent with anti-resorptive and anabolic properties, but with side effects when applying systemic administration. GelMA-SR doped nanosized hydroxyapatite (SrHA) composite hydrogel scaffold with controllable Sr delivery capability [24]. Cosmin et al. DLP-based 3D printing developed a novel GelMA- strontium-doped nanohydroxyapatite (SrHA) composite scaffold for bone tissue regeneration featuring controllable strontium (Sr) release capabilities. They investigated the biocompatibility of the composite hydrogel scaffold. In vitro cell culture demonstrated that osteoblasts could adhere and proliferate on the surface of the hydrogel. The DLP- prepared GelMA composite hydrogel tissue engineering scaffolds offer innovative avenues for research in bone loss repair [25].
Skin Repair
The prevalence of burn and skin ulcer patients is significant, with chronic skin ulcers having a severe impact on their quality of life. Therefore, there is a great need for the development of scaffolds or biomimetic skin through tissue engineering. By utilizing 3D printing techniques that combine human keratinocytes, fibroblasts, and endothelial cells, rapid preparation of vascularized microstructures and perfused skin grafts can be achieved. DLP-based 3D printing provides a rapid manufacturing method to curing human skin fibroblast (HSF) and human umbilical vein endothelial cell (HUVEC) hydrogel material to form biomimetic skin. Zhou et al. utilized a biomimetic bioink (GelMA/HA-NB/LAP) and DLP-based 3D printing to fabricate functional living skin (FLS). FLS possesses interconnected microchannels that facilitate cell migration, proliferation, and new tissue formation. By mimicking the physiological structure of natural skin, FLS promotes skin regeneration and neovascularization. The three-dimensional (3D) artificial skin model provides a variety of platforms for testing skin transplantation, disease mechanisms and skin tissue. However, achieving physiological complexes in such hierarchical structures, such as the neurovasculature with living cells, is extremely difficult [26]. Choi et al. DLP-based 3D printing printed a full-thickness skin model by employing methacryloyl-modified silk fibroin (SFMA) and GelMA, incorporating multiple cell types. They evaluated the printability, mechanical properties, and cell viability of SFMA/GelMA construct at various concentrations in order to determine the optimal printing concentration for artificial skin models. The simulation model confirmed that epidermal growth factor could enhance wound healing in both epidermal and dermal layers [27].
Peripheral Nerve Repair
Peripheral nerve injury is a significant cause of disability, often resulting in motor and sensory impairments. Treating peripheral nerve injuries poses a major technical challenge in the fields of reconstructive surgery and regenerative medicine. Utilizing DLP-based 3D printing, the rapid fabrication of personalized nerve conduit shows promise as an effective method to enhance peripheral nerve healing.The nerve conduit is a promising treatment for long-gap peripheral nerve injury, but with limited efficacy. Drug-releasable scaffolds may provide a reliable platform to construct a regenerative microenvironment for neural recovery. Tao et al. A functional nanoparticle-enhanced nerve conduit for promoting peripheral nerve regeneration was prepared by DLP-Based 3D Printing. The conduit consists of a gelatin-methylacryanyl (GelMA) hydrogel and drug-loaded poly (ethylene glycol) -poly (3-caprolactone) (MPEG-PCL) nanoparticles dispersed in the hydrogel matrix. Such nanoparticles in the conduit can release Hippo pathway inhibitors to promote nerve regeneration and functional recovery [28]. Zhang et al. fabricated a biodegradable self-adhesive bandage by utilizing a series of clickable functionalized monomers, including azide-modified gelatin methacryloyl and dibenzylcyclooctyne-modified GelMA. This bandage possesses the capability to envelop injured nerves and selectively release drugs for neural repair purposes. Through electrophysiological assessment and histological examination using a rat sciatic nerve transection model, it was confirmed that the drug-loaded self-adhesive bandage developed by Zhang et al. effectively promotes peripheral nerve regeneration and facilitates recovery [29]. Zhang et al. A double-branched GelMA neural conduit was constructed by DLP-based 3D printing .The efficacy of the double-branch nerve conduit was evaluated by the transfer of the rat tibial nerve to the peroneal nerve. The results of functional and histological evaluation showed that the double-branch nerve conduit could not only promote the regeneration and functional recovery of the peroneal nerve in the injury, but also retain the function of the donor nerve, demonstrating the potential application of this conduit in nerve transfer [30]. Wu et al. successfully employed continuous DLP printing to manufacture elastic hydrogel conduits encapsulating nanodrugs, utilizing GelMA/methacryloyl-modified silk fibroin (SFMA) composite hydrogels. This material exhibited favorable effects on cell adhesion, proliferation, and migration. Electrophysiological, morphological, and histological evaluations conducted through animal experiments demonstrated that the conduit effectively promoted axonal regeneration, myelin sheath regeneration, and functional recovery by providing an optimal microenvironment. Peripheral nerve injury is a common condition that often causes disability and poses challenges to the surgeon. Drug-releasable biomaterials provide a reliable tool for regulating the nerve healing-related neurorepair microenvironment. A self-adhesive bandage was designed to form parcels around the injured nerve to promote nerve regeneration and recovery [31].
Conclusion
DLP-based 3D printing technology offers significant advantages in resolution, efficiency, and working conditions. Its non-direct contact forming method provides relatively gentle conditions for cell printing, making it a promising construction technology for tissue engineering. GelMA composite hydrogels possess excellent biocompatibility, adjustable mechanical properties, and good formability, presenting enormous application prospects in tissue repair. By adjusting GelMA’s substitution rate and compositing with other materials, hydrogel systems can be prepared to meet different application requirements. However, prior to the clinical implementation of GelMA construct, it is imperative to address concerns such as standardizing GelMA synthesis methods and ensuring the safety of photoinitiators and hydrogel materials. Additionally, material properties should be expanded to meet more complex clinical demands such as controlled degradability of GelMA materials. For DLP printing technology and equipment to fully realize its personalized advantages in 3D printing applications like bedside printing technologies need further development.
References
DOI: 10.31038/AFS.2024613
Introduction
With global warming, the shortage of water resources is aggravated, and a large amount of oily wastewater produced by the petroleum industry poses a threat to the ecological environment. The traditional oil-water separation methods have some problems, such as low efficiency, long cycle, complicated operation and secondary pollution. The appearance of ultra-wetting materials has brought new hope for solving these problems. This paper focuses on the application of ultra-wetting materials in the field of oil and water separation, introduces the limitations of traditional separation methods, expounds the research progress of ultra-wetting materials, wetting theory, and discusses various types of ultra-wetting materials in detail, and finally summarizes the shortcomings of existing materials and looks forward to the future.
Superwetting Oil-Water Separation Material
Super Hydrophobic – Super Oil Wet Material
Summarizing this type of material, compared with the previous two, its three-dimensional structure is equivalent to a random stacking of multi-level two-dimensional materials, which significantly enhances separation efficiency. Additionally, small oil droplets undergo demulsification, coalescence, and separation within the internal space, thereby achieving emulsion separation and efficient “dewatering”. However, for most non-metallic substrates, further research is needed to explore and improve their mechanical stability, reusability, and durability.
Super Hydrophilic – Underwater Super Oil Phobic Material
In summary, in the realm of superhydrophilic–underwater superoleophobic three-dimensional materials, there still exist a series of application issues such as structural instability, poor overall wear resistance, and susceptibility to contamination in complex environments. These issues serve as inspirations for targeted solutions in subsequent development efforts. Additionally, practical applications of the material are often limited by factors such as synthetic preparation methods. Nevertheless, overall, these “oil-removing” type three- dimensional wetting materials exhibit higher emulsion separation performance compared with two-dimensional materials.
Superhydrophobic – Superoleophobic Materials
According to the previous discussion, three-dimensional materials can utilize porous nickel foam substrates, directly forming micro-nano rough structures on the three-dimensional framework. Compared with two-dimensional materials where particles adhere to the surface and are combined with binders, this approach offers superior performance and a more efficient preparation process. For non-metallic substrate materials, the three-dimensional structure provides sufficient space to accommodate inorganic hybrid polymers, forming a unique porous structure and significantly enhancing their mechanical strength.
“Special” Ultra-Wetting Materials
Compared with two-dimensional materials, three-dimensional “special” superwetting materials exhibit enhanced water absorption capabilities. Additionally, the selection of these materials increasingly considers the application of green, biodegradable materials. To address common oil–water separation clogging issues, porous superamphiphilic materials offer a fundamental solution, with aerogel materials selectively capturing the water phase to improve separation performance.
Smart Switchable Superwetting Material
Two-dimensional switchable superwetting materials focus on reusability and recyclability while conserving energy. They achieve on-demand emulsion separation under external stimuli, effectively addressing the single-use issue of one dimensional materials. Additionally, the in situ growth method overcomes the stability problems common in most superwetting materials.
Summary and Outlook
In the future, green and biodegradable base materials have enormous development potential and prospects. The green recycling of materials for renewable use is a key direction for future research. However, current recycled materials still exhibit some apparent disadvantages: cumbersome and complex recycling processes, high energy input, poor durability, and a short lifespan during use. The future aims to combine repairability, self-cleaning, high corrosion resistance, and material recycling to form a completely new industrial chain and breakthrough direction in technology development.