An Environmental Sociological Approach to the Mechanism of Nature Being Destroyed and Its Implications
Leave a reply
Background
Pericardial disease resulting in a pericardial effusion is a common clinical finding with numerous etiologies identified including trauma, infection, neoplasm, autoimmune etiology, metabolic cause, or a drug-related process. Once the diagnosis of pericardial effusion has been made, it is important to determine whether the effusion is creating significant hemodynamic compromise resulting in cardiac tamponade. In addition, the timing of accumulation of the pericardial fluid significantly affects the presentation of each case. Typically, a rapid accumulation is seen in acute cases and a delayed accumulation in a subacute presentation. Distinguishing between the diagnoses of pericardial effusion and cardiac tamponade is vital in order to treat a patient appropriately. We report two cases of pericardial effusion with differing etiologies, both resulting in cardiac tamponade physiology and exhibiting components of Beck’s triad. Not only did the two cases differ in etiologies, but in the length of fluid accumulation and timeframe of presentation as one presented as a rapidly accumulating pericardial effusion with acute cardiac tamponade and the other as subacute. Despite these differences, both cases were managed similarly with the creation of a pericardial window and drainage of the pericardial fluid to restore normal hemodynamics.
Case series
Case #1: An 80 year-old Caucasian male with a past medical history of a non-ischemic cardiomyopathy with a left ventricular ejection fraction of 35% and New York Heart Association Class III, left bundle branch block, hypertension, hyperlipidemia, abdominal aortic aneurysm, and previous cerebrovascular accident presented for routine cardiac resynchronization therapy defibrillator (CRT-D) placement. The left pectoral area was sterilely prepped and the left subclavian vein accessed. A defibrillator lead was fixated with a screw-in technique in the apical septal location of the right ventricle (RV); the lead was repositioned twice due to inappropriate parameters. An atrial-pacing electrode was then advanced and fixed with a similar screw-in technique in the high right atrium. Next, a coronary sinus guiding catheter was advanced into the coronary sinus and into a posterolateral branch. A left ventricle (LV) pacing lead was then advanced to the posterolateral branch; both the guidewire and the lead terminated prematurely in the lateral wall, suggesting a suboptimal position for optimal CRT. The guide catheter was then advanced into a second lateral wall vessel, and then the pacing lead was successfully placed in the mid lateral wall of the LV. All three leads tested adequately and optimized without extracardiac stimulation noted. The leads were connected to a CRT-D generator, and then the pocket was closed. Thirty minutes postoperatively, the patient’s blood pressure dropped to 92/60mmHg with a heart rate of 88bpm. The patient was in no visible distress, but mild jugular venous distention and muffled heart sounds were noted on physical exam. Stat transthoracic echocardiogram (TTE) demonstrated a moderate pericardial effusion conferential to the heart, with RV diastolic collapse and respirophasic changes of less than 50% variation in the inferior vena cava, suggesting mild cardiac tamponade (Figure1).

Figure 1. Acute cardiac tamponade with a moderate pericardial effusion anterior and posterior to the heart, with partial right atrial and right ventricular collapse.
Cardiothoracic surgery took the patient directly to the operating room, and an emergent cardiac window for suspected RV perforation was completed. Although no clear perforation was seen interoperatively; 175mL of blood was evacuated with improvement in systolic blood pressure to over 150mmHg. A chest tube was placed and set to suction with an additional 500ml of blood removed over 48 hours. The patient recovered and was discharged with close cardiology follow up.
Case #2: A 66 year-old African American male with a past medical history of small cell lung cancer, COPD, tobacco use, and occupational exposure to asphalt presented with a one-day history of a new, tender right clavicular mass and worsening pleuritic chest pain and dyspnea with exertion. The patient was initially diagnosed with a small cell lung cancer in July 2018. He was initially treated with palliative chemotherapy including Etoposide and Cisplatin, and he achieved remission in October 2018. Unfortunately, he subsequently developed a recurrence in the left upper lobe in January 2019. The patient received palliative radiation until he was unable to tolerate treatments. Further mediastinal and osseous metastases were found after the chemotherapy and radiation were discontinued. Nine days prior to this presentation to the hospital, the patient underwent a therapeutic left thoracentesis due to a symptomatic, malignant pleural effusion. On primary assessment in the emergency room, the patient was found to be tachycardiac with a pulse of 121bpm and oxygen saturation of 94% breathing ambient air. The physical examination revealed a large, 7x6cm right clavicular mass extending into the neck. A cardiopulmonary exam revealed sinus tachycardia, jugular venous distention, and decreased breath sounds on the left. An EKG showed sinus tachycardia, a low voltage QRS, and no significant ischemic changes. A chest x-ray and then stat non-contrast CT neck/thorax revealed a new, large pericardial effusion and left greater than right bilateral pleural effusions (Figures 2, 3). Cardiology was consulted and a stat TTE demonstrated a large pericardial effusion, anterior and posterior to the heart, with features consistent with tamponade physiology (Figure 4).

Figure 2. Chest x-ray revealing a flask-shaped cardiac silhouette as evidenced in pericardial effusions, as well as a large, left-sided pleural effusion.
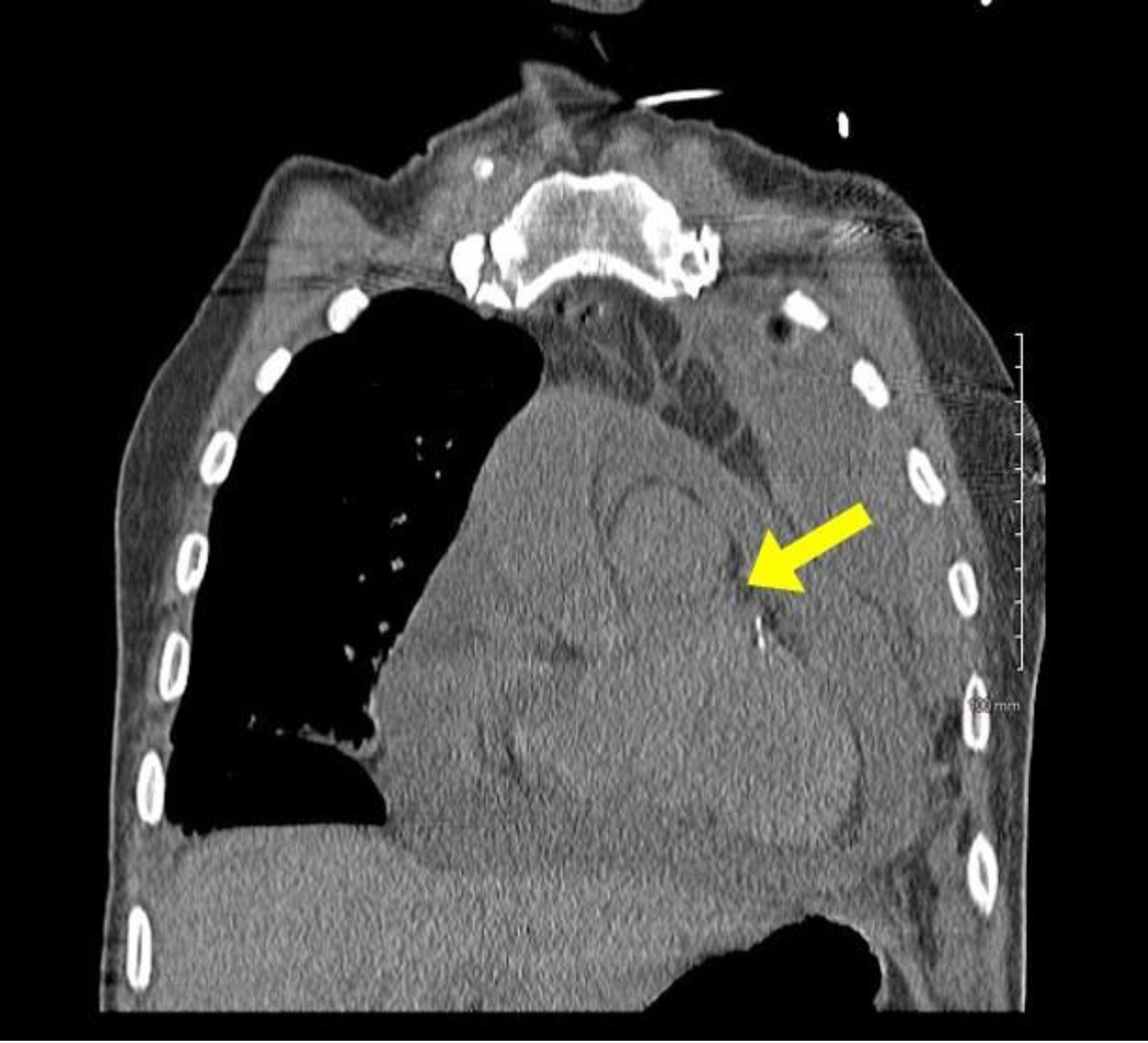
Figure 3. Stat CT chest with a coronal view demonstrating a large pericardial effusion.
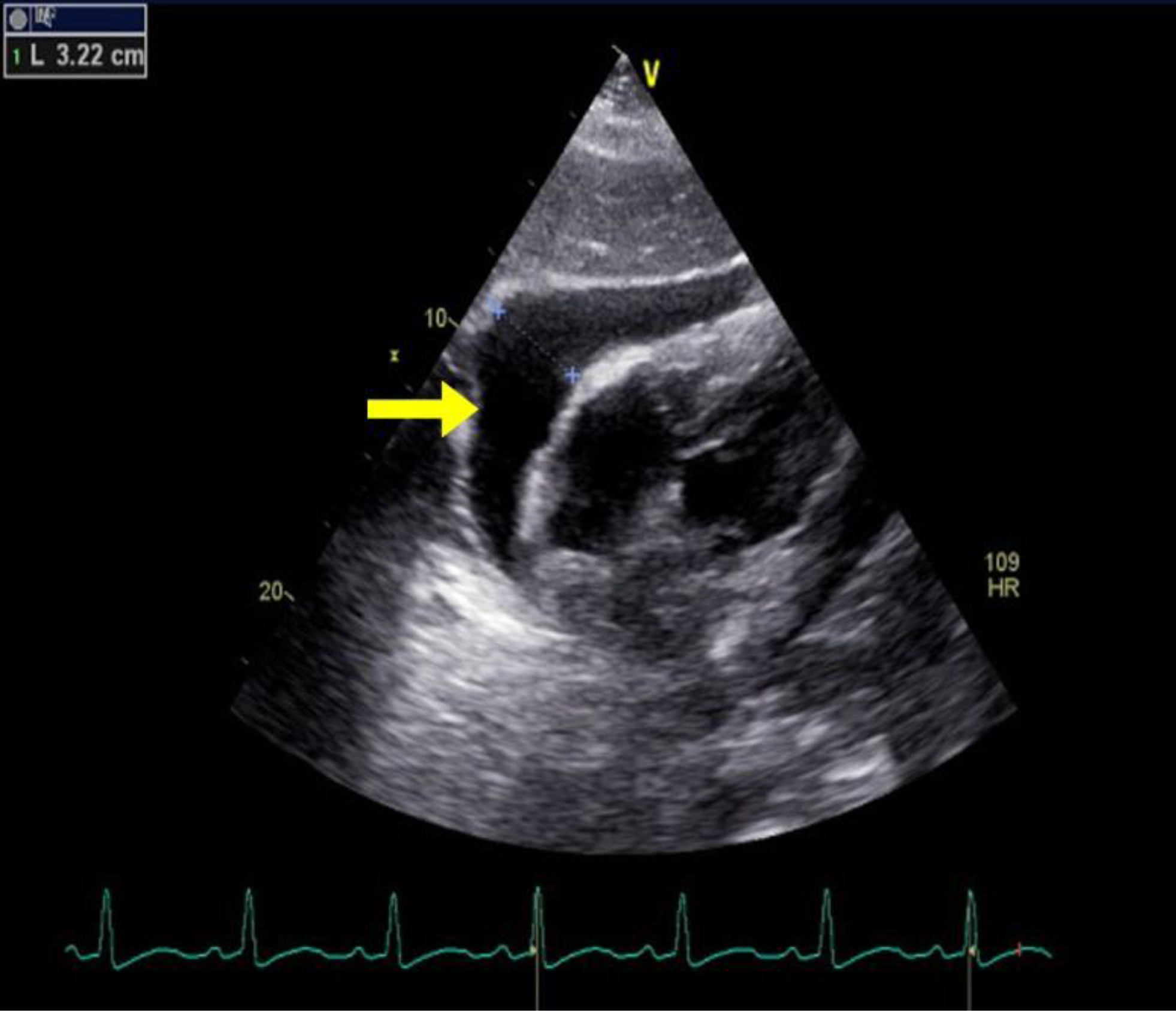
Figure 4. TTE with parasternal long axis view demonstrating large pericardial effusion measuring 3.22cm.
Cardiothoracic surgery was then consulted and a therapeutic pericardial window was performed with 700cc of bloody fluid drained. In addition, a portion of the pericardium was resected and sent to pathology. Cytology revealed a malignant pericardial effusion consistent with small cell carcinoma. In addition, the patient underwent left thoracentesis and placement of a chest tube intra-operatively. He tolerated the procedures well and was transferred out of the ICU to the medical-surgical floor the day following surgery. Two days later, he underwent a right thoracentesis for a symptomatic, right-sided pleural effusion. On post-operative day 5, the patient acutely decompensated and was transferred to the ICU. Vital signs upon transfer showed a blood pressure of 67/51mmHg, heart rate of 118bpm, respiratory rate of 45, and pulse oximetry of 60%. An arterial blood gas was obtained that showed pH of 7.153, pCO2 of 54.7, pO2 of 29, and bicarbonate of 19.2. A stat EKG and TTE were obtained, with the EKG revealing atrial fibrillation with rapid ventricular rate, premature ventricular or aberrantly conducted complexes, and a low voltage QRS. Bedside TTE revealed a recurrent, circumferential, small pericardial effusion without signs of tamponade or RV strain. In addition, no recurrence of left pleural effusion was identified. Due to the patient’s condition, the patient’s family made the decision to proceed with comfort measures only and further hospice care. Unfortunately, the patient passed away on post-operative day 7 due to complications related to the underlying small cell carcinoma and the associated malignant pleural and pericardial effusions.
Discussion
The presentation of cardiac tamponade depends on the timing over which the pericardial effusion accumulates. Acute cardiac tamponade occurs within minutes, and this physiology is seen in our first case. It resembles cardiogenic shock, and an emergent reduction in intrapericardial pressure (IPP) is required for treatment [1]. The second type, subacute cardiac tamponade, occurs over days to weeks. This is seen in our second case. Patients initially may be asymptomatic until the IPP reaches a critical limit, at which time symptoms such as chest pain or dyspnea ensue [1]. The pericardium is a fibroelastic sac that encases the heart and proximal great vessels [2]. It is composed visceral and fibrous parietal layers, typically containing 50ml or less of serous fluid which serves as a lubricant to reduce the friction on the epicardium [2,3]. Any processes causing this volume to exceed the typical amount, thus raising the IPP, is known as a pericardial effusion [2]. Pericardial effusions are classified based upon onset, size, location, hemodynamic changes, and composition [3]. Pericardial effusions can be loculated or circumferential and can be composed of transudative fluid, exudative fluid, pus, air, or blood [3]. Inflammatory causes can include viral, bacterial, fungal, or protozoal infections. A pericardial effusion can also be related to autoimmune disease, drug hypersensitivity, or post cardiac procedure syndromes as seen in our first case [2]. Non-inflammatory causes include hypothyroidism, trauma, or a reduction in lymphatic drainage from heart failure, cirrhosis, nephrotic syndrome, or malignancy [2] as seen in the second case.
Under normal physiologic conditions the pericardial pressures are low, and systolic and diastolic changes cause little interventricular interaction. Inspiration causes a decreased pulmonary vascular resistance, leading to an increase in venous return to the right ventricle and a small drop in the pulmonary capillary wedge and left ventricular end diastolic pressures. This leads to a decrease in systolic blood pressure of approximately 5mmHg [2]. An increase in the fluid collection in the pericardial space causes right and left ventricular pressures to increase and equalize. In addition, with the normal increasing pressure in the right ventricle with inspiration, the rigid pericardium prevents the free wall from expanding, leading to bulging of the interventricular septum into the left ventricle [2]. During inspiration in a patient with cardiac tamponade, the drop in pulmonary venous pressure leads to a drop in left atrial and pulmonary capillary wedge pressures. The left ventricular diastolic pressure remains elevated due to a leftward bowing of the interventricular septum and reduced left ventricular compliance. This exacerbates a decline in left ventricular filling pressures, and ultimately leads to a decrease in stroke volume [2].
Beck’s triad of hypotension, elevated jugular venous pressure, and muffled heart sounds are significant for severe cardiac tamponade, and components of this triad are seen on both our cases [4,5]. Patients often appear uncomfortable, with additional signs of cardiogenic shock including tachypnea, cool extremities, diaphoresis, and altered mental status [5]. Hypotension is typically present in acute tamponade, but some patients who initially present with subacute tamponade may be hypertensive on admission [5]. Tachycardia is frequent unless the patient is on a medication which may dampen this response [5]. Pulsus paradoxus is another hallmark of pericardial tamponade, defined by an inspiratory decrease in systolic blood pressure greater than 10mmHg due to a combination of a reduction in intrathoracic pressure, left ventricular stroke volume and pulse pressures [2,6,7]. A differential for these symptoms includes decompensated heart failure, pulmonary embolism, pulmonary hypertension, and a right ventricular myocardial infarction [5].
EKG abnormalities in cardiac tamponade include electrical alternans and reduced voltage, which we saw in the second case. Electrical alternans is more specific, but less sensitive, and is caused by the anterioposterior swinging of the heart during systole and diastole [5]. With larger pericardial effusions, a chest x-ray may show an enlarged cardiac silhouette with a flask-like appearance [5]. The standard non-invasive method for detecting a pericardial effusion is M-mode and two- dimensional Doppler TTE. Small pericardial effusions are typical seen over the posterobasal left ventricle, which with increasing size become circumferential [5]. These are graded in diastole as small (<10mm), moderate (10–20mm), and large (>20mm) [5,8]. Tamponade is distinguished first by early diastolic right ventricular and late diastolic or early systolic right atrial collapse when the IPP transiently exceeds the intracavitary pressures [5,8–10]. Exaggerated interventricular size variability can be appreciated throughout the cardiac cycle, with an interventricular septal bounce towards the left ventricle [8]. IVC plethora can be seen with dilation of the IVC greater than 20mm, and collapse with inspiration less than 50%, which has a 92% sensitivity for cardiac tamponade [8]. Changes in Doppler velocities across the mitral, tricuspid, right/left ventricular outflow tracks, and hepatic/pulmonary veins may add additional clues to this diagnosis [8]. A TTE provides better quality images, but is typically impractical to coordinate due to the need for urgent intervention. A CT or MRI may provide more details on loculated effusions and coexistent pleural effusions [5].
Definitive treatment of cardiac tamponade is through the reduction of IPP by removing pericardial fluid. In early cardiac tamponade where there is no hemodynamic compromise, conservative treatment with close hemodynamic monitoring and serial TTEs may be considered [11]. Acute cardiac tamponade is a medical emergency when hemodynamic compromise is present. Per the European Heart Journal 2015 guidelines [1,11], a pericardiocentesis is the treatment of choice, and the catheter is left in the pericardial space until the fluid return is less than 25ml per day [1,11]. A pericardial window is a surgical alternative requiring anesthesia, and it is used for loculated, malignant, or recurrent pericardial effusions [2,9]. An example of this procedure was seen during both of our cases. A pericardial window is also preferred if a biopsy is desired [2,9]. Intravenous hydration and rarely inotropic support or mechanical ventilation may be required depending on the clinical situation. Surgical drainage is preferred if a pericardial biopsy is needed for recurrent or loculated pleural effusions, or if a coagulopathy is present [1,11]. Pleural fluid studies can help identify the cause of the effusion. Post-operative monitoring includes telemetry for 24–48 hours, and a follow up TTE in 1–2 weeks and then in 6- 12 months [1].
Conclusion
Pericardial effusions can accumulate quickly resulting in acute cardiac tamponade, as seen in our first case, or in a subacute fashion with an insidious onset as evidenced by our second case. Beck’s triad of hypotension, elevated jugular venous pressure, and muffled heart sounds is the classic finding of acute tamponade; however, these clinical findings may not always be present. The diagnosis is typically made by physical findings and echocardiographic evidence. It is important to establish the size and hemodynamic effect of a pericardial effusion. The first line treatment for cardiac tamponade is pericardial drainage, either by pericardiocentesis or pericardial window.
Consent
Both patients provided informed consent.
Disclaimer
This research was supported (in whole or in part) by HCA and/or an HCA affiliated entity. The views expressed in this publication represent those of the author(s) do not necessarily represent the official views of HCA or any of its affiliated entities.
Acknowledgements
We would like to thank Dr. Hartmuth Bittner for his surgical expertise.
References
Abstract
Temporomandibular Disorders (TMD) are the most prevalent cause of facial pain without a clear etiopathogenesis and gold standard treatment. There is not an agreement on treatments which involve surgical or conservative interventions. Between the different types of conservative treatments the Fascial Manipulation® could be a promising therapy. Here we describe the case of a patient with orofacial pain that was treated successful with three single sessions of Fascial Manipulation®.
Keywords
TMJ, Fascial Manipulation®, Orofacial pain.
Introduction
Orofacial pain is a heterogeneous group of musculoskeletal and neuromuscular conditions involving the temporomandibular joint complex, surrounding musculature and osseous components [1]. Between these, Temporomandibular Disorders (TMD) are the most prevalent cause of orofacial pain. TMD are highly prevalent and debilitating conditions involving the head and face, with pain affecting the jaw, ears, eyes and frequently causing headache and neck pain [2]. The etiology of chronic TMD is multifactorial and include structural, functional, environmental, social and psychological factors [3]. The prevalence of orofacial pain is between 3% and 12% and is, at least, twice as prevalent in women as men [4]. Musculoskeletal structures disorders include myalgia, usually presents as a dull aching pain due to continued muscle tension, Myofascial Pain (MFP) also presents as a dull, continuous aching pain that varies in intensity. MFP produces pain upon palpation that is local and may refer to other sites, as mapped out by Simons [5]. MFP tends to be seen in muscle pain conditions of a more chronic nature, in which the tension is unremitting. Trigger points can often be seen in MFP and may be localized to a taut band of muscle.
In the literature, treatments for TMD include patient education, home care programs, physical therapy, musculoskeletal manual approach, pharmacotherapy, Non Steroidal Anti-Inflammatory drugs (NSAIDs), local anesthetics, intracapsular injection of corticosteroids, muscle relaxants, antidepressants, occlusal appliance therapy, occlusal adjustment. Surgical care is only indicated when non-surgical therapy has been ineffective [6]. However, the multifactorial pathophysiology of TMJ related pain is far from being completely understood and effective management of pain has not been established yet [7]. Unfortunately, despite the evidence of two systematic reviews that support manual therapy to produce favorable outcomes in TMD [8, 9] the real effectiveness of different types of manual therapy in TMD remains unclear. A manual therapy named Fascial Manipulation® is shown in a preliminary study to be effective in improving tmj disorder when compared to botulin toxin [10]. Here we present to case of a patient with chronic tmd disorder treated successfully treated with Fascial Manipulation.
Case report
A 65 years old woman, mixed race, Brazilian was assessed and treated at the TMD clinic of the Faculty of Dentistry, State University of Rio de Janeiro (UERJ). She complained of orofacial pain and difficulties chewing and eating for the last 25 months, with concomitant neck pain and an history of headache lasting more than 5 years. She referred a history of whiplash following a car accident that occurred 7 years ago.
The patient has undergone many months of physical therapy without significative improvement and she has been using an Oral Appliances (OAs) (also known as flat plane stabilization appliance, Michigan splint, muscle relaxation appliance or gnathologic splint) for the last 6 months. Pain was described as constant, burning sensation severe enough to affect sleeping. Perceived pain was assessed with the Visual Analogue Scale (Vas) and scored as 9 on a 0–10 scale (Table 1) The RDC/TMD was utilized as the gold-standard instrument and performed by a sole examiner, trained and calibrated according to specifications established by the International RDC/TMD Consortium. At the initial examination it was recorded the occurrence of TMJ clicking, crepitus, or jaw opening interferences with or without pain. The clinician viewed the patient’s opening and closing patterns to note any mandibular deviations. The evaluation of mandibular ROM consisted of measuring comfort opening, unassisted opening, assisted opening, with a millimeter ruler while noting the severity and location of pain with jaw movement (Table 2) The EMG evaluation of the temporalis and masseter muscles during maximum voluntary contraction (tooth clenching) were carried out using the New miotool (MiotecEquipamentosbiomédicosltda, Petrópolis, Porto Alegre, RS, Brasil) with 14-bit resolution and a sampling frequency of 2000 Hz, IRMC > 126 dB and signal noise rate < 2 LSB, Security insulation 3000 V(rms) (table 3). All procedures were performed three times, with a thirty seconds interval between isometric contractions to avoid muscle fatigue. After electromyography signal acquisition, all the data were processed in Miotec Suite (MiotecEquipamentosbiomédicosltda, Petrópolis, Porto Alegre, RS, Brasil) to analyse the root square mean (RMS) in µV. All the evalution were carried out before the Treatment (T0), after the treatment (T1) and at 3 months follow up (T2). On physical examination the range of motion of the neck (ROM) was limited in the sagittal plane (neck flexion) and on the frontal plane (lateral flexion). The palpatory verification of the CC and CF was carried out according to the Stecco’s method (reference) on the following segments: thorax (TH), Scapula (SC), Neck (CL), Head (CP2, CP3) to identify the densified points (Figure 1). The points are selected after a specific assessment process, guided by a specific chart (FM chart) [11] involving medical record, clinical examination of specific movements and palpatory verifications. Palpation evaluates patient pain rate, radiation and most important, the presence of tissue stiffness, call “densification” [12]. During the clinical history, the segments in dysfunction are identified with an emphasis on the chronology to permit the development of an hypothesis based on the current symptomatology of patients and previous musculoskeletal events, which may be causing compensations. In Fascial manipulation the therapist use the elbow and knuckles generating a deep friction for 3–5 minutes over each point.
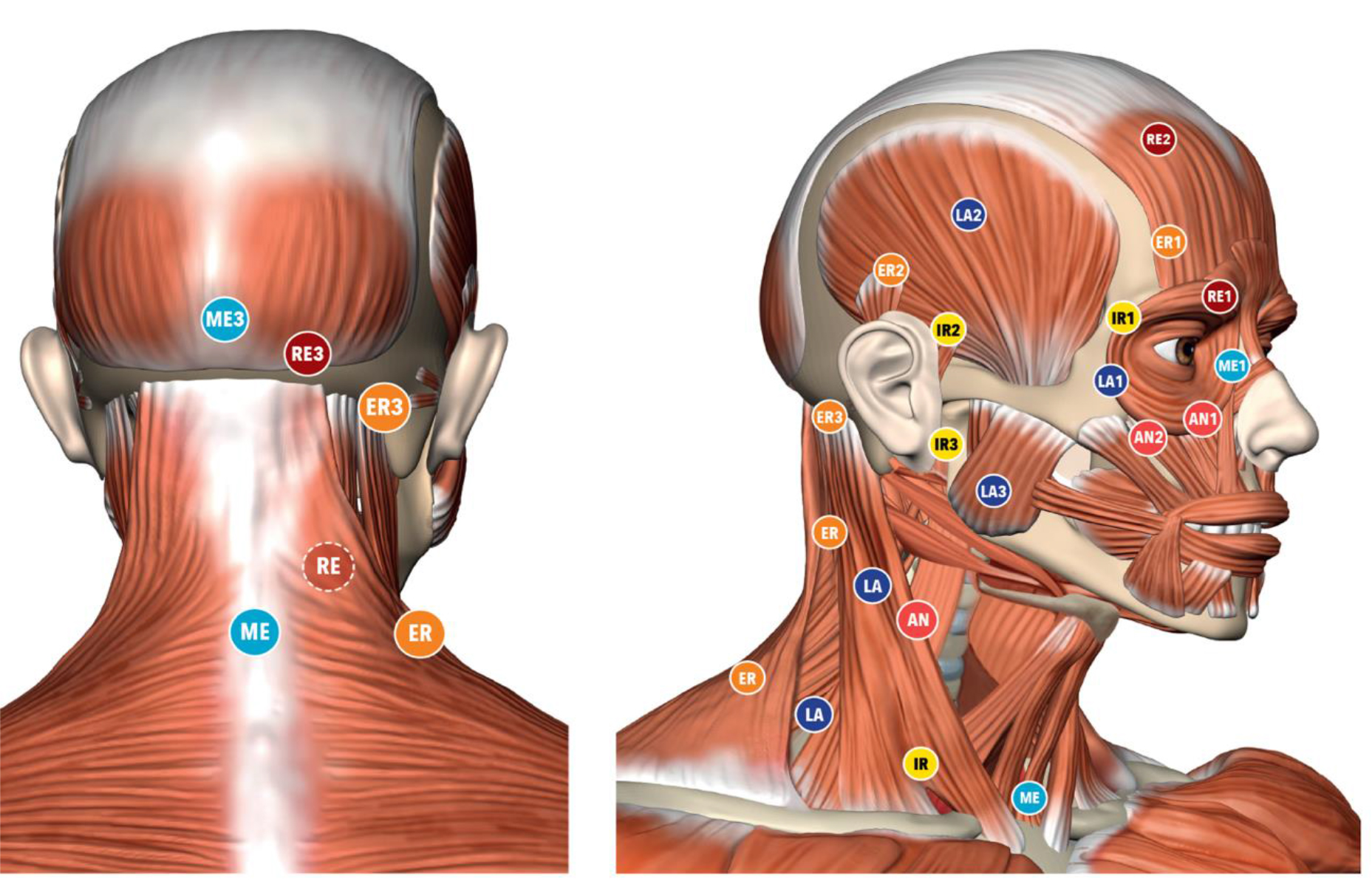
Figure 1. Location of the Center of Coordination points
The treatment are applied over specific points, call Center of Coordination (CCs) and Center of Fusion (CFs), that are anatomically safe because do not overlie major superficial nerves and veins. Additional guidance for point selection includes avoiding the patients’ excessively painful areas where inflammation, lesions or even fractures could be present. The patient underwent three weekly session of Fascial Manipulation® of 1 hour. The VAS scale, between initial condition (T0) and after the treatment (T1) was maintained at 3 month follow up (T2) (Table 1). The patients passed from the symptomatic condition (VAS 9) to asymptomatic (VAS 1) after the treatment. The comfortable without pain opening of the mounts improved (Table 2). Un-assistant and assistant opening improved after treatment, at T1 and T2 follow up. In the table 3 are presented the value of the isometric contraction which improved for the masseter and temporalis muscles bilaterally.
Table 1. VAS T0 = VAS before treatment; T1 = VAS after treatment; T2 = VRS after 3 months
|
|
VAS |
|
T0 |
136.56 |
|
T1 |
264.60 |
Discussion
In the light of our case report, Fascial Manipulation® can improve pain, function and myoelectrical activity in patient with orofacial pain. FM was able to diminish the articular loading on the TMJ which translate in a better mandibular kinematics with less muscle pain. Even if FM share some similarity with other techniques, it presents a different rationality and clinical approach. While the deep friction can be compared to other techniques, the reasoning behind the choice of points treated presents major differences. The points are selected after a specific assessment process involving clinical history taking, a clinical examination of specific movements as well as palpatory verifications [12, 11]. Apart from the use of clinical procedures (palpation, auscultation, measuring of active and passive mandibular mobility), FM requires additional orthopedic tests that implies a modern, biomedical approach, thanks to the knowledge of the human fascial system, but, at the same time, uses an individual approach to the patient as recommended by many Authors [13–15].
Table 2. Assisted: maximum opening with help, unassisted: maximum opening without help. T0 = before treatment; T1 = after treatment; T2 = 3 months;
|
|
Comfortable |
Unassisted opening |
Assisted opening |
|
T0 |
32,51 |
45,30 |
49,23 |
|
T1 |
42,33 |
51,14 |
54,08 |
|
T2 |
40.1 |
48,18 |
50,75 |
Table 3. EMG evaluations of the masticatory muscles in isometric contraction T0= before treatment; T1= after treatment; T2= 3 months
|
|
Right |
Left Masseter |
Right Temporal |
Left |
|
T0 |
136.56 |
176.27 |
154.45 |
127.50 |
|
T1 |
264.60 |
260.75 |
221.47 |
159.61 |
|
T2 |
411.61 |
427.30 |
279.65 |
215.82 |
Conclusion
FM could be used as an effective method for facial pain being a rapid, safe and cost effective approach to reduce pain and gain function and mouth opening that can be used before occlusion stabilization appliance. We suggest further studies that compare the combined treatment of FM with temporomandibular disorder treatment in patient with TMD in a Randomized Controlled Trial (RCT).
References
Abstract
Peri-operative environments are a hazardous setting for diabetes patients. A systematic review of literature regarding the management of diabetes patients across the peri-operative pathway has been undertaken to assess if the management of patients within this pathway is suitable and effective for patients.
Methods
A database search of Google Scholar, CINAHAL, Embase, OVID, Cochrane Library, Joanna Briggs institute and PUBMED was undertaken from 15th of March 2019 to 30th of March 2019. A total of 57 papers were found and reduced down to 11 final papers that answered the review question and met the inclusion and exclusion criteria. Inclusion criteria were: Full text, English language, human subjects, adult patients only and studies that focused on diabetes care in a section of the peri-operative pathway. Exclusion criteria: children or adults and children, studies that looked a one particular intervention or type of surgery. No date limit was set. PICO tool was used to frame the study question.
Results
Three main themes emerged from the literature. 1. Poor patient outcomes; 2. Longer length of stay (LOS); 3. Lack of adherence to guidance and or protocols and glycaemic control. Elective patients had advantageous outcomes compared to emergency surgical patients. Hyperglycaemia still remained a problem with an increase in other medical complications for diabetes patients. LOS in hospital was found to have increased due to medical complications. Adherence to protocols and guidance was found to be beneficial in monitoring and managing hyperglycaemia. However, this review found that best practice guidance and hospital protocol is not always adhered to. A liberal approach to glycaemic control is beneficial.
Conclusion
This systematic review investigated the management of diabetes patients across the peri-operative pathway. Three main themes emerged from the literature: poor patient outcomes; length of stay; and lack of adherence to guidance and or protocols and glycaemic control. We concluded the peri-operative environment is a hazardous setting for a diabetes patients. Elective patients had slightly more advantageous outcomes than emergency patients. Hyperglycaemia still remains a problem which leads to poor patient outcomes and longer LOS. Adherence to protocols and guidance was found to be beneficial in monitoring and managing hyperglycaemia.
Introduction
The Department of Health and Social Care (DOH) (2001) state that diabetes patients undergoing surgery carry a greater clinical risk than non-diabetes patients. This is due a number of complex factors such as reduced food intake due to a starvation period, and cessation of normal diabetes medications [1]. In addition, the body’s stress response and inhibition of insulin secretion increases the potential for hyperglycaemia [2]. The Association of Anaesthetists of Great Britain and Ireland [3] state that diabetes affects 10–15% of the surgical population, with these patients carrying a greater risk of complication rates, mortality rates and Length of stay (LOS).
Despite these findings, there is very little guidance and research surrounding diabetes management across the peri-operative pathway. There are currently no standardised worldwide guidelines for use by theatre or PACU practitioners [4] and globally, diabetes management during the peri-operative period is widely debated [5]. The aim of this systematic review was to investigate the management of diabetes patients across the peri-operative pathway.
Methodology
A systematic and comprehensive search of databases was carried out between the 15th of March 2019 and the 30th of July 2019. The search involved Google Scholar, CINAHAL, Embase, OVID, Cochrane Library, Joanna Briggs institute and PUBMED. Combinations of key words were inputted into each database. Further restrictions were then applied to reduce the number of papers, such as; English language, full text and used adult human patients as the participants. Studies which examined the care and management of diabetes patients across the peri-operative pathway were included. Studies into specific interventions or surgeries were excluded due to the broadness of the review question. Exclusion criteria: children participants and studies that looked a one particular intervention or type of surgery. No date limit was set.
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure systematic transparency of report [6]. After duplications were removed, 57 papers were read to determine their relevance to the review question.
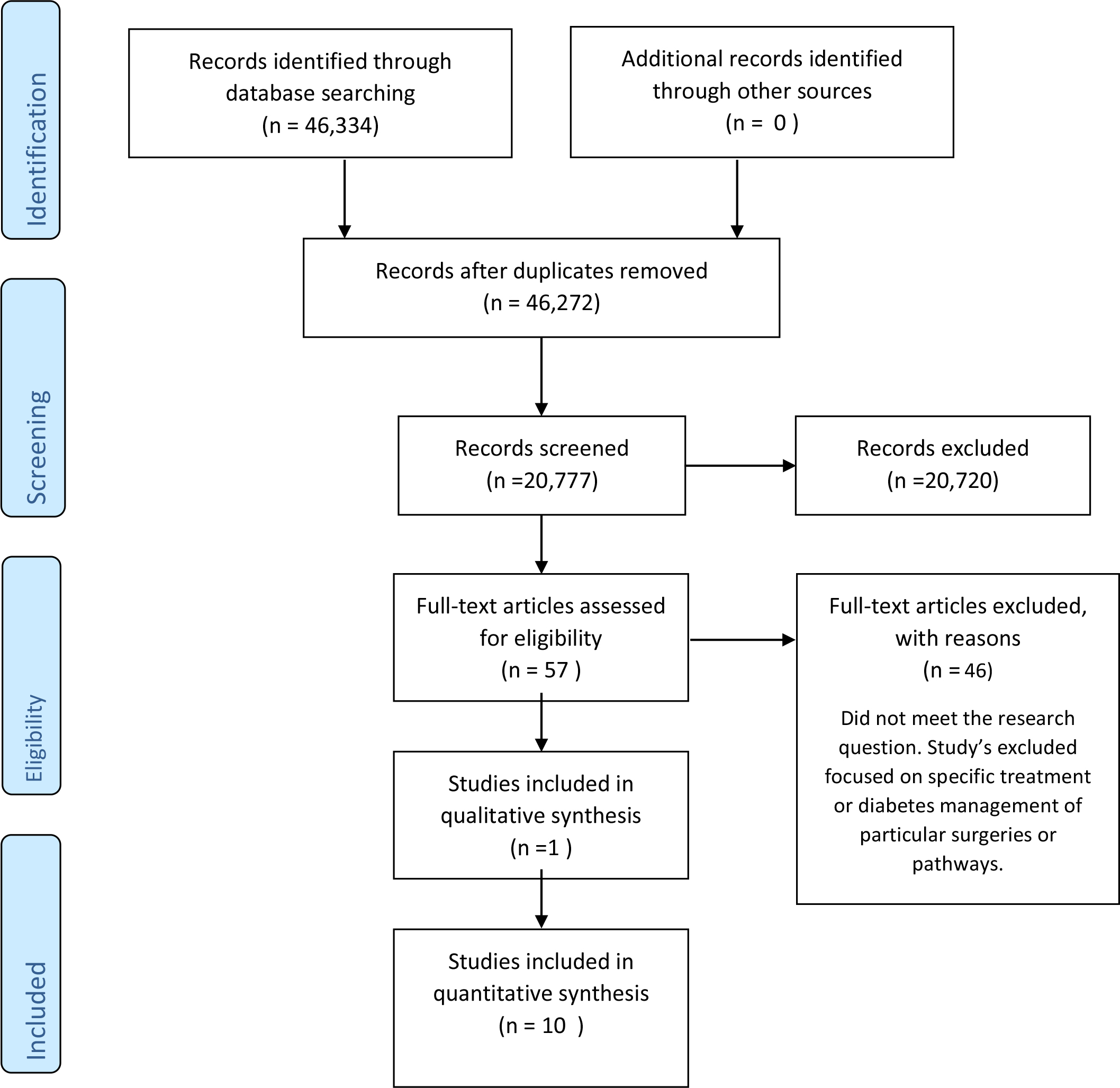
Figure 1. PRISMA flow diagram of Studies included in quantitative synthesis
The Cauldwell, Henshaw and Taylor (2011) framework was utilised for assessing the meaningfulness or generalisability of qualitative and quantitative research in contemporary nursing practice, which enabled a structured approach to the assessment of each study’s quality, validity and reliability (Clarke, 2011). The final 11 papers were RAG (red amber green) rated [7] to reflect the answer to each of the questions from the tool. Dates ranged from 1983- 2019 and included studies from various countries. 9 of the 11 studies focused on the peri-operative period. 1 study focused on intra-operative and post-operative diabetes management. 1 study looks at diabetes management in the pre-operative period. Full text was then read to extract the results from each paper for the formation of themes.
Results and discussion
A systematic review as undertaken to establish the management of diabetes patients across the peri-operative pathway. Three key themes emerged from the review: poor patient outcomes, length of stay (LOS) which were commonly reported jointly and adherence to guidance and or protocols and standards for glycaemic control.
Poor patient outcomes
8 out of 11 studies reported on the outcomes of patients with diabetes. Studies 2, 3,5,6,8,9,10 and 11 discussed surgical outcomes directly related to diabetes management. McCavert, Monem and Dooher, et al [8] found that best practice of glycaemic control, in-line with hospital protocols, saw a 25.4% reduction of peri-operative complications. Overall complications being 29% (out of 69 patients). Elective patients with T2DM were more prone to complications. 5 out of 17 (29.4%) of T2DM elective patients experienced complications; in contrast, only 4 out of 21 (19.0%) of elective patients with T1DM developed a complication such as wound infection or peritonitis. For emergency patients, the rate of complications was slightly higher for those with T1DM (5 out of 14; 35.7%) versus 6 out of 17 patients (35.3%) with T2DM. Complications such as; Wound dehiscence, septicaemia, wound infection, wound infection, confusion, deep vein thrombosis and lower respiratory tract infection were reported as a complication. Frisch, Chandra, Smiley, et al [9] similarly analysed outcomes of mobility contrasting both diabetes and non-diabetes patients. Outcomes such as pneumonia (12.1 vs 5.4%; p=0.001), wound and skin infections (5 vs 2.3%; p<0.001), systematic blood infection (3.6 vs 1.1%; p<0.001), urinary tract infections (4.5vs 1.4%, p<0.001) acute myocardial infarction (2.6 vs 1.2 %; p< 0.001) were reported. Patients who experienced complications had a strong affiliation with high blood glucose levels pre and post-operatively.
“Haemoglobin A1c, often abbreviated as A1C, is a form of haemoglobin (a blood pigment that carries oxygen) that is bound to glucose” [10]. Underwood, Askari, Hurwitz et al [11] linked to various A1C categories to patient outcomes. It showed that, like McCavert et al and Frisch et al, [8, 9] diabetes patients (specifically group A1C ≤6.5%) had a higher incidence of LOS, acute renal failure death within 30 days and wound class (dirty). Groups ≤6.5%, A1C> 8-10% and A1C > 10% was significantly longer compared with the control subjects (p<0.001,p<0.008, and p=0.002, respectively).
Wang, Chen, Li, et al (2019) found that patients over 65-years old, male, high mean post-operative blood glucose (BG), diabetes complications, abnormal kidney function and have underwent general surgery were the highest risk category for poor patient outcomes. The study compared surgery type and patient outcomes. Of the 301 (19.8%) of all patients with diabetes complications, 295, (98.0%) had major vascular complications, 8 (27. %) had diabetes nephropathy, 3 (0.7%) had diabetes retinopathy, 5 (1.7%) had diabetes foot post-operatively. Post-operative adverse events occurred in 118 (7.7%) including 43 (36.4%) delayed extubation caused by surgery-related respiratory failure or muscle weakness. 15 (12.7%) patients had circulatory disorders, 23 (19.5%) had respiratory and circulatory abnormalities. 11 (9.3%) had non-healing of the incision. 15 (12.7%) had infections at other sites. 8 (6.8%) patients with other complications. 3 (2.5%) patients died due to pulmonary embolism and two cases of septic shock. Kotgal, Symods, Hirsch, lrl, et al [12] did not correlate BG management with patient outcomes, but results showed that patients had a greater chance of poorer outcomes with any level of hyperglycaemia versus those who had better diabetes control.
In contrast, Sathya, Davis, Taveria, et al [13] found that stroke, atrial fibrillation and wound infection were the most significant complications from pooled results of 6 studies. Mixed results were noted; 2 pooled results found that the incidence of post-operative stroke was reduced by liberal glycaemic regimes, but pooled results from a further 3 studies suggested that there was no significant difference between the effect of moderate vs strict control on stroke outcomes (odds ratio, 18.5, 95% CI 0.72-4.74, p=0.020). Sathya et al [13] also examined the relationship between atrial fibrillation as a patient outcome and diabetes control. Again, pooled estimates from 2 pooled studies found that moderate versus liberal control had no direct effect on atrial fibrillation as an outcome (Odds ratio 0.54, 95% CI 0.17-1.76, p =0.31). In addition, pooled results from 3 other studies found that there was no significant difference between strict versus moderate control in relation to atrial fibrillation (odds ratio: 0.71, 95% CI0.39-1.30, p=0.27). Wound infection was also not found to have a significant link to the effects of moderate versus glycaemic control from the results of 2 pooled studies.
Length of stay
LOS was a significant finding in studies 2, 3, 6 and 8. Although not a complication in itself, LOS was linked to or reported alongside poor patient outcomes.
McCavert et al [8] found that Emergency patients had a significantly longer LOS in hospital than the elective groups. Frisch et al (2010) [9] also reports that diabetes patients had a higher rate of complications than non-diabetes counterparts (p=0.105). Patients with diabetes were found to have a greater LOS (and LOS in ICU) than non- diabetes patients. It was also noted that African American patients were not at an increased risk of mortality than other races. No other study compared likelihood of surgical outcomes and race.
Patients with diabetes were also more likely to have greater complications including LOS. Underwood et al, 2014 [11] however, reported that patients with A1C levels >6.5-8% had a similar LOS to the control group. Patients with higher A1C ≤6.5 up to greater than 10% had a significantly longer LOS compared to control subjects. This was the most significant difference of the various A1C groups compared in the study. Higher A1C level was more significant than any other variable such as a diabetes patient’s race, gender or type of surgery in relation to LOS. Longer LOS in the hospital was found by Hommel et al [14] to be associated with higher dissatisfaction of patients regarding patient centred-ness in their assessment of results.
Lack of adherence to guidance and or protocols and glycaemic control
The third key theme that emerged from the literature was adherence to guidance, such as hospital protocols and national guidelines and glycaemic control. This theme was disused in studies 1,2,5,7 and 10.
McCavert et al [8] studied both elective and emergency surgical patients. 60% of elective patients with T1DM were not treated according to hospital protocol. Elective patients who were treated according to protocol had a complication rate of 6.3 %. For emergency surgical patients, 7.3% of T1DM patients who were treated as per protocol developed a complication. 12.3% of scheduled blood glucose measurement were not completed. 11.1% of T1DM elective patients did not have their blood glucose checked, and 6.8% of emergency T1DM patients. For T2DM, blood glucose was not checked in 17.4% of elective patients and 12.7% in emergency cases.
Similarly, Coan, Schlinkert, Brandon et al [15] note that capillary BG was taken in 89% of cases in the pre-operative area, and only52% of patients had a HBA1C. Intra-operatively, 33% of patients had a BG check, and the post- operative figure was 87%. 90% of pre-operative BG was point of care (POC), and 4% was venous sampling. Intraoperatively, 10% of patients had POC BG values, 16% had POC blood gas sampling. In the PACU, 86% of BG were obtained by POC and 1% was venous. Similarly, Jackson, Patvardhan et al (2015) reported that only 71% of patients had a HBA1C recorded pre-operatively and 56% intra-operatively via CBG. 73% of patients had a CBG performed in recovery (PACU) contrary to national guidance. Hommel, Van Gurp, Tack et al’s [16] quality indicators suggest that best-practice involved measuring BG 4 hours pre-operatively, every 2 hours intra-operatively, and 1 hour post-operatively. Hommel et al [14] reported that in relation to patient satisfaction and person centeredness, 20% of 362 patients were not informed about intra-operative BG level and its effect. 15% were also not informed that insulin was administered during surgery. This correlated to overall low score from patients’ involvement in the survey. Sathya et al [13] report that patients undergoing a liberal target for glycaemic control had significantly better post-operative outcomes (less or no complications) than other groups. No difference with wound infection or atrial fibrillation were found. Bibble (1983) commented from the 3 case studies that protocols for glycaemic control were directed towards managing ‘average’ diabetes patients rather than complex ones, making guidance non-beneficial.
Future recommendations would be to undertake extensive quantitative and qualitative research across the peri-operative pathway with staff who have direct responsibility for diabetes patients undergoing surgery. The views and attitudes of staff members regarding diabetes management may shed light on the barriers as to why this is still a problem despite being highlighted by several studies seen in this review since 1983. Any further research conducted needs to be influential on practice in order to drive change.
Conclusion
This systematic review examined the management of diabetes patients across the peri-operative pathway. Three main themes emerged: poor patient outcomes; longer length of stay; and lack of adherence to guidance and or protocols and glycaemic control. We concluded the peri-operative environment can be a hazardous setting for diabetes patients. Elective patients had slightly more advantageous outcomes than emergency patients. Hyperglycaemia still remains a problem which leads to poor patient outcomes and longer LOS. Adherence to protocols and guidance was found to be beneficial in monitoring and managing hyperglycaemia.
Table 1. Characteristics of studies

References