Abstract
During pregnancy, it is very common for women to make changes in the choice of foods they eat and often experience cravings and aversions to certain foods. The purpose of this narrative review is to describe the current state of knowledge about the different hypotheses that try to explain the presence of food cravings and aversions during pregnancy and to know the occurrence of these phenomena in different geographical contexts.
The most studied hypothesis relates to food aversions to maternal-fetal protection mechanisms; others with less sustenance link them as preventive of the metabolic syndrome, as a consequence of shortage of resources or compensatory of placental growth. The hypotheses that explain the appearance of food cravings relate them as a consequence of a search for nutrients or active compounds present in the foods craved for, or as a consequence of the hormonal fluctuations that are special to pregnancy.
The prevalence with which cravings and aversions occur varies from 38 to 79%, being less frequent in European populations and more common in the African continent. In general terms, foods craved by pregnant women in Western cultures are chocolate, fruits and fruit juices, sweet foods and, to a lesser extent, meats and dairy products. In geographical contexts of socio-economic vulnerability, foods of animal origin such as meat, cheese and milk, followed to a lesser extent by vegetables, fruits and grains, emerge as usually cravings.
Protein-rich foods of animal origin are largely rejected by pregnant women in Western countries, while cereals and vegetables are frequently avoided by pregnant women in Africa and Asia.
Keywords
Pregnancy, Cravings, Aversions, Food Choice
Introduction
Pregnancy is a complex and vitally important period and its physiology is of great biological and nutritional importance since the contribution of nutrients must be adequate in quantity, quality and distribution so that both the process of embryogenesis and development of the fetus and health of the mother are adequate [1, 2].
It is common for pregnant women to make changes in the choice of foods they eat, which are the result of a complex set of biological and cultural interactions that have implications for maternal and child health [3–6]. Within these food variations appear phenomena that pregnant women frequently experience: cravings and aversions to certain foods. These phenomena, in which causes and consequences are little known, are usually considered as anecdotal and marginal [7].
Several conceptualizations and definitions have been used in relation to the terms “cravings” [4,6,8–11] and “aversions”[4,6,8,10–12], among them the one used by Weigel, who points out that they are phenomena with the following characteristics: sudden appearance, strong intensity and absence prior to pregnancy [11].
It is important to distinguish food cravings during the pregnancy from pica, a condition characterized by the persistent and compulsive consumption of non-nutritive substances such as earth and clay (geophagia), ice (pagophagia), among others [13, 14]. In the case of aversions, it is necessary to differentiate them from food taboos, in which certain foods are not culturally accepted as suitable for consumption in particular phases of the life cycle, such as pregnancy. Taboos in most cases seem to be meaningless since the characterizations of food vary from one population group to another [15, 16].
The important physiological changes of pregnancy, especially hormonal ones, could in part give an answer to understand the complex plot of possible causes that cause food cravings and aversions in the pregnant woman [17–20]. (Graph 1) outlines the hormonal interactions that could influence on the appearance of food cravings and aversions.
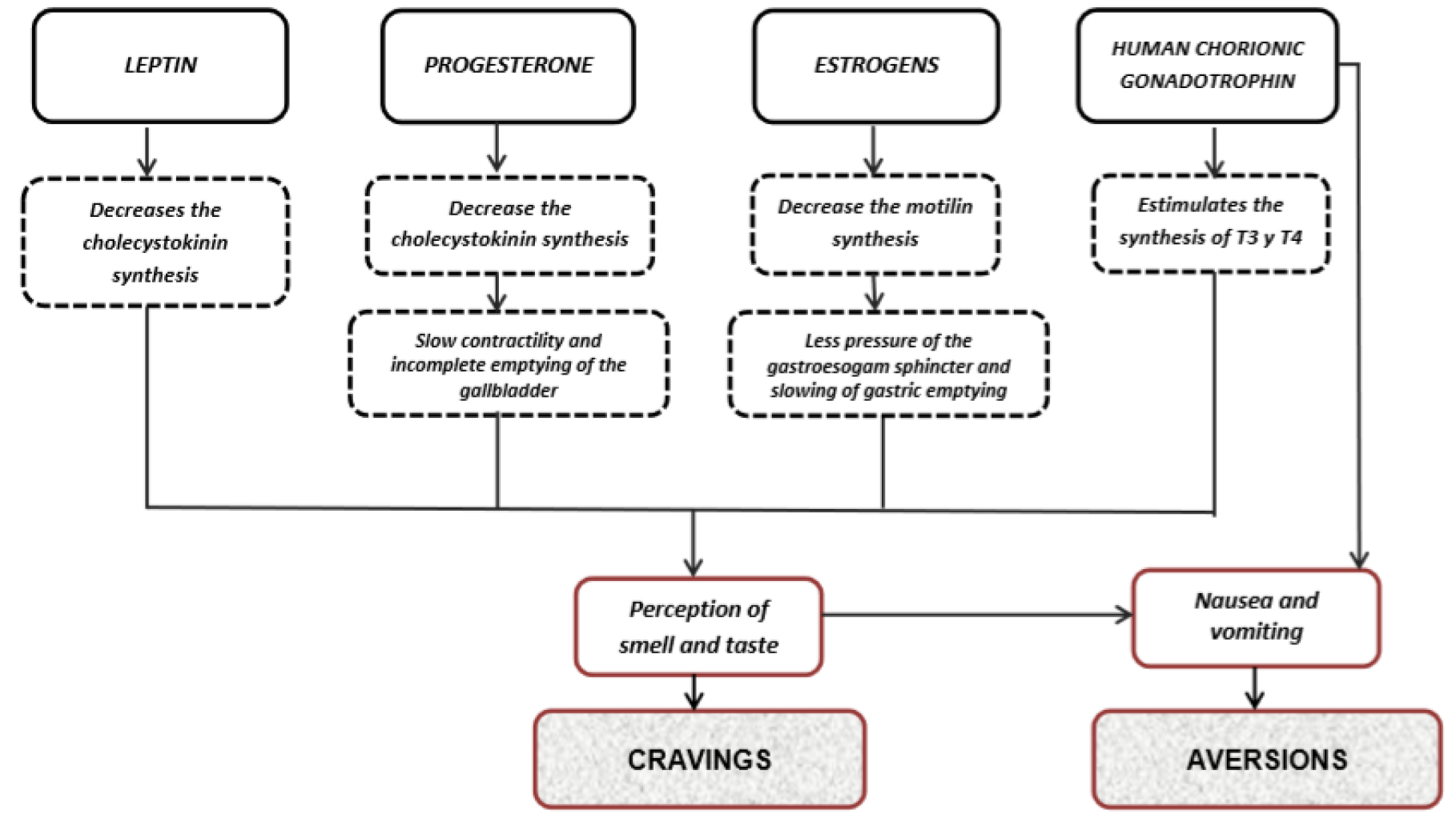
Graph 1. Possible hormonal influence on food cravings and aversions.
The rabbi, physician and philosopher Maimonides (1138–1204) was one of the first to take into account changes in maternal physiology to describe food cravings, and proposed the theory that they were the result of an imbalance in body fluids, caused by the accumulation of “bad liquids” in the stomach folds of pregnant women, due to their inability to release menstrual blood during conception. When these liquids penetrated the stomach, a woman craved sour and spicy things until these unpleasant juices were eliminated by the vomit. As the pregnancy progressed and the growing fetus reduced the penetration of these fluids, women would be less susceptible to cravings and nausea [21].
Since then and until now, food cravings and aversions during pregnancy have been the focus of research and debate among anthropologists, nutritionists and public health professionals.
The present work consists of a narrative review that aims at describing the current state of knowledge about the different hypotheses that try to explain the presence of food cravings and aversions during pregnancy and to know the occurrence of these phenomena in different geographical contexts.
Hypothesis about the Presence of Food Aversions
Several hypotheses centered on a biological perspective have been postulated in order to understand why some pregnant women present food aversions; possibly the hypothesis of maternal-fetal protection has been the most studied. Other explanations with less bibliographic support link dietary aversions as preventive of the metabolic syndrome during pregnancy, or related to shortage of resources, or as a compensation mechanism for placental growth.
“Maternal-fetal protection hypothesis”
This theory is based on the fact that food aversions could protect the embryo or fetus against certain toxins at a moment of extreme vulnerability: organogenesis. Of the approximately 280 days that gestation lasts, embryonic tissues are more susceptible to teratogenic damage during certain well-defined critical periods, when cell division and differentiation and the morphogenesis of various systems and organs reach a simultaneous peak, produced between weeks 6 and 18. [10]. If the presence of food aversions occurs mostly during these periods, the pregnant woman could have developed different adaptive mechanisms to face the challenges of pregnancy.
This hypothesis is based on the year 1940, when Irving, in a study from Boston, observed that pregnant women with gravid hyperemesis had fewer spontaneous abortions than the usual expectation for that moment, postulating a possible association between nausea and vomiting with positive results during pregnancy [10, 22, 23].
Thirty-six years later, Ernest Hook resumed this observation and raised the “embryo protection hypothesis”, suggesting that in early pregnancy nausea, vomiting, food aversions, together with anatomical and sensory changes evolved as a complex set of symptoms that would make pregnant women avoid or expel foods with strong smells or flavors that could be potentially toxic and / or teratogenic. Their observations were based on the decrease in alcohol consumption, caffeine and the desire to smoke that women presented during pregnancy, which were explained by sensory changes and by nausea and vomiting, symptoms that could act as fetusprotectors [24].
Later in 1988, this hypothesis is extended by Margie Profet [25, 26], who proposes that nausea, vomiting and food aversions would be an evolutionary adaptation mediated by the modification of taste and olfactory sensibility to protect the embryo against the maternal ingestion of “toxins” present in some foods. Certain “toxic” plants that supposedly contain high levels of potentially abortive or teratogenic phytochemicals should be avoided. While humans commonly ingest phytochemicals naturally present in vegetables, and also selectively use phytochemicals in the preparation of food (spices), some of them could be potentially harmful during pregnancy, such as those present in bitter-tasting vegetables and spicy foods with strong flavor. Profet also suggests that the methods of cooking by frying, roasting or toasting would be the frequently aversive or avoided because their strong smells would indicate the presence of potentially mutagenic compounds, as well as decaying animal foods that emit suggestive smells due to the presence of parasites and / or bacteria that cause deterioration and produce toxins. On the other hand, it could be predicted that the best tolerated foods would be those that have mild smells and flavors and that do not decompose easily, such as breads, cereals and processed grains.
Later on, other authors deepened this hypothesis by renaming it “maternal-embryo protection hypothesis”, theorizing that pregnant women learn to avoid and / or expel through vomit potentially dangerous foods, not only for their embryos in development but also for themselves [8,11,12,27,28]. As part of this adaptation that evolved, in a coordinated way, the vomit would expel the noxious substance, while the nausea would be produced by an experience of aversion [27].
Hypothesis about “dietary aversions as preventive of the metabolic syndrome during pregnancy”
This proposal suggests that aversions during pregnancy may have evolved, in part, to motivate women to avoid eating foods that increase the risk of developing certain chronic non communicable diseases, particularly gestational diabetes mellitus [28–30].
Following this line of reasoning, dietary aversions would be an evolutionary tactic in populations without a long history of cereal cultivation to avoid the metabolic syndrome. This idea is based on evidences that come from populations in which, historically; the sugar necessary for fetal growth was not available due to a shortage of cereals, grains and starches or due to intense and regular cycles of hunger. In these cases, aversions to these carbohydrate-rich foods were possibly a mechanism to prevent the gestational metabolic syndrome [28, 29].
Hypothesis about “Scarcity of resources”
From the evolutionary biology, certain authors support that a decrease of the alimentary aversions during pregnancy in vulnerable populations could be predicted, with an important load of infectious diseases, with alimentary insecurity and anthropometric indexes that indicate a deficient maternal nutrition. However, studies in which all these associated factors were evaluated could not demonstrate their relationship with the food aversions of pregnant women [12, 31, 32].
Hypothesis about “Compensation of placental growth”
This hypothesis suggests that dietary aversions in the early stages of pregnancy would improve the growth of the placenta; thus, the fetus would exert a “manipulation” upon the maternal physiology, in such a way that mothers are motivated to avoid highly energetic meals. The restriction of maternal energy would benefit the fetus because, according to this hypothesis, mothers with restricted energy intake will prioritize the destiny of any resource that they have available for the development of the placenta and the embryo [28,33]. This position was based on observations of the severe hunger that affected the West of the Netherlands between the years 1944–1945 and its relationship with the weight of the placenta and neonate [28]. It was observed that when the period of maternal malnutrition occurs only during the first trimester, moment that coincides with the highest prevalence of food aversions, the neonates have weights within the normal range and greater weight of the placenta, effects that are not observed in undernourished mothers in the second half of pregnancy. This finding, which is also observed in animals, suggests that malnutrition in the first trimester would lead to a compensatory placental growth [33–35].
Hypothesis about the presence of food cravings
Different statements try to explain the reasons that could be responsible for the presence of cravings during pregnancy. The hypotheses found are: the search for nutrients or cravings in response to nutritional deficiencies; cravings in relation to the presence of active compounds in the desired foods and cravings as a result of hormonal fluctuations.
Hypothesis: “Cravings as a search for nutrients” or “In response to nutritional deficiencies”
From a biological perspective, it was postulated that cravings could serve to provide depleted nutrients in maternal diets, [9, 28]. This position considers craving as a mechanism to ensure adequate and balanced nutrition during pregnancy, which would motivate pregnant women to seek and consume foods rich in energy and micronutrients essential for fetal development.
Some authors consider that taking into account that the nutritional needs of the fetus increase as their development progresses, the intensity of the cravings should follow the same upward trajectory [9,28,36].
In 2002, the anthropologist Daniel Fessler, from an evolutionary perspective, also suggests that pregnant women may have a particular predisposition to seek through cravings, missing nutrients from their diets due to losses caused by aversions and vomiting; that is, there would be a functional link between cravings and food aversions [27]. These interactions were observed in pregnant women who had aversions to certain foods and they were more likely to have cravings compared to those who did not have food rejections [3]. However, this synergy between aversions and food cravings still remains a controversial issue that requires greater evidence from different geographical, social or cultural contexts [10].
Hypothesis: “Cravings are due to the presence of active compounds in the desired foods”
It is suggested that cravings could be due to the presence of active compounds (phytonutrients) in the desired foods [9]. The benefits of potentially bioactive ingredients are due to the possible ability to alleviate physical and perhaps psychological symptoms associated with pregnancy, such as fatigue, irritability and cramps, among others [9]. Chocolate being one of the foods most desired by pregnant women in some contexts, it is pointed out that women’s inclination to it could be cyclical and hormone dependent [9]. The biologically active components of chocolate such as methylxanthines, biogenic amines and cannabinoid-like fatty acids can trigger transient feelings of well-being during pregnancy [37]. However, this relationship is also questioned because the potentially active ingredients of chocolate are present in small quantities, which would make their potential benefits unlikely [9].
Hypothesis: “Cravings are due to hormonal fluctuations”
This hypothesis relates the presence of cravings with the sensory modifications resulting from the hormonal changes that occur during pregnancy. Several hormones such as estrogen, progesterone, leptin, ghrelin and neropeptide Y, among others, change significantly in this period affecting sensory perception with an increase in sensitivity to smells, taste and smell and indirectly being able to influence the selection pattern of the food. [9, 37, 39]. Despite these observations, there is an information gap that relates the exact nature of the link between hormonal fluctuations during pregnancy and food cravings [9].
(Table 1) summarizes the most relevant hypotheses and their foundations on the possible causes of the appearance of food aversions and cravings during pregnancy.
Table 1. Most relevant hypotheses and their foundations upon the possible causes of the appearance of food aversions and cravings during pregnancy.
|
Hypotheses |
Authors, year (Reference) |
Foundations |
|
AVERSIONS |
||
|
Maternal-fetal protection
|
Hook, 1978 (23) |
Nausea and vomiting work to protect the embryo by expelling dangerous chemicals transmitted by food and resulting in subsequent aversion. At first, the possible relationship between nausea, vomiting and aversions to alcohol, coffee and tobacco is explored. Then, this hypothesis is extended to certain “toxic” potentially abortive or teratogenic plants. After this, the presence of nausea and vomiting is linked to the development of food aversions and it is theorized that pregnant women learn to avoid and / or expel through vomit potentially dangerous foods not only for the developing embryo, but also for themselves. |
|
Preventive of the metabolic syndrome during pregnancy |
Haig, 1996 (44) |
The aversions during pregnancy may have evolved, in part, to motivate women to avoid eating foods that increase the risk of developing metabolic syndrome and / or gestational diabetes mellitus.
|
|
Scarcity of resources |
Holland, 2003 (45) |
Food insecurity and anthropometric indices that indicate poor maternal nutritional status could predict a decrease in dietary aversions during pregnancy. |
|
Compensation of placental growth |
Huxley, 2000 (30). |
Malnutrition in the first trimester of pregnancy, a period that coincides with food aversions, would lead to compensatory placental growth. |
|
CRAVINGS |
||
|
Search for nutrients or in Response to nutritional deficiencies |
Tierson, 1985 (33) |
They consider craving as a mechanism to ensure adequate and balanced nutrition during pregnancy, in which women are motivated to seek and consume foods rich in energy and micronutrients essential for fetal development. |
|
Presence of active compounds in the desired foods |
Orloff, 2014 (9) |
The pregnant woman, through cravings, consumes food with bioactives that produce a sensation of well-being.
|
|
Hormonal Fluctuations |
Orloff, 2014 (9) |
There is a relationship between hormonal changes and the frequency and intensity of cravings in pregnant women. |
Although there may be a biological and evolutionary component in the development of these modifications in food preferences, food cravings or aversions do not escape the cultural food patterns that are also involved in the food choices of pregnant women [5]. There are civilizations that have a cultural model in which the cravings must be fulfilled by the pregnant woman, in some cases rituals are performed at the end of pregnancy to ensure that the wishes of the woman and the “fetus” have been fulfilled [9, 12]. However, in other cultural settings, pregnant women do not have a “special” treatment, so cravings are not very valued [12].
In such a way that from an anthropological and cultural perspective, interpreting the meanings behind the expressions of food cravings and aversions and unraveling the biocultural mechanisms of these food choices could be more complex than expected. In addition to evolutionary influences, experiences during an individual’s life can have significant impacts on the nature of food cravings and aversions. Both the context and social status as well as relative wealth can affect the choices of which foods are desired or avoided by the pregnant women [5].
Possible consequences postulated upon the presence of food cravings
Beyond the different theories that can cause food cravings, we have also tried to explain the possible consequences that such cravings could generate in the pregnant woman. A recent explanation suggests a possible association between cravings and the risk of excessive weight gain during pregnancy [9]. This association is based on the high frequency of cravings during pregnancy in North American women, and the increasing increment in the prevalence of pregnant women with greater weight gain than recommended [40–42]. This construction is based on the popular belief that cravings should be fulfilled by pregnant women. A possible explanation could be based on a model in which the cravings result from ambivalence or a tension between giving (please) or avoiding (effort to restrict consumption) the desired food. It is assumed that women, in general, try to resolve this ambivalence in favor of abstinence due to the cultural pattern of thinness, but this model also gives occasional permission to break the restriction, resulting in episodic consumption and potentially excessive of the desired foods [9]. This statement would be supported in part by recent studies [41, 43] that identify cravings during pregnancy as a possible predictor of excess of weight gain.
Another potential risk suggests that cravings for sweet foods are associated with an increased risk of abnormal glucose tolerance and the development of gestational diabetes mellitus [44, 45]. In some studies, women who developed gestational diabetes mellitus had a decreased perception of sweet taste and an increase in food cravings with that taste mainly during the third trimester, compared to healthy pregnant women. However, these associations are weak and other investigations fail to support this association between cravings for sweet-tasting foods and maternal blood glucose levels [45, 46].
Prevalence and characteristic of food cravings and aversions
The prevalence with which cravings occur varies from 40 to 79%, the lowest figure comes from Europe, while the highest prevalence corresponds to the African continent. With respect to food aversions, its occurrence varies from 38% in pregnant women in Asia to 78% in Africa.
The nature of the food desired and / or rejected also has special characteristics according to the geographical context in which they are studied, possibly shaped by cultural, ethnic and / or socio-economic influence. In general terms, foods craved for by pregnant women in Western cultures are chocolate, fruits and fruit juices, sweet foods such as ice cream and desserts and to a lesser extent different types of meat and dairy products. On the other hand, pregnant women in other geographic contexts of greater socioeconomic vulnerability experience cravings mainly for protein foods of animal origin such as meat, cheese and milk followed to a lesser extent by vegetables, fruits and grains.
On the other hand, meat and protein-rich foods such as dairy products are largely avoided by pregnant women from Western countries, followed by coffee, highly spicy foods and to a lesser extent vegetables. Cereals such as wheat, corn and rice and less strongly vegetables and meats are mostly avoided by pregnant women in other geographical areas such as Africa and Asia.
(Table 2) summarizes the prevalence and characterization of food cravings and aversions in different geographical contexts.
Table 2. Prevalence and characterization of food cravings and aversions in different parts of the world.
|
Author, year (reference) |
Place (n) |
Prevalence of cravings and foods mostly craved for |
Prevalence of aversions and foods mostly aversive |
|
Tsegaye, 1998 |
Africa, Etiophia (n:295) |
72% |
65% |
|
Nyaruhucha, 2009 |
Africa, Tanzania (n: 204) |
73% |
70% |
|
Young, 2012 |
Africa, Kenya and Tanzania: (n:188) |
56% |
78% |
|
Patil, 2012 |
Africa, Tanzania (n: 545) |
79% |
63% |
|
Placek, 2015
|
Asia, India (n:149)
|
50% |
60% |
|
Qureshi, 2015 |
Asia, Pakistan (n: 110) |
78% |
38% |
|
Mc Kerracher, 2016 |
Oceania |
Bananas, mango, green leafy vegetables, fish and meat. |
Fish, cassava, meat, non-fish aquatic foods, imported starches, locally grown starches and rarely spicy, sour or bitter-tasting vegetables. |
|
Bayley, 2002 |
Europe, Great Britain (n: 99) |
61% |
54% |
|
Hill, 2015 |
Europe, Great Britain (n: 1693) |
39% |
Not studied |
|
Coronios Vargas, 1992 |
América, USA |
dairy products, chocolate, tea |
Vegetables, meats and dairy products. |
|
Weigel, 2011
|
América, Ecuador (n: 849) |
69% |
74% Different types of meats (beef, pork, lamb, liver, other organs, sausages), poultry (chicken), fish (tilapia, sea bass, tuna), seafood (shrimp, prawns, squid) and chicken or quail eggs, “toxic vegetables” such as cabbage, cauliflower, broccoli, Brussels sprouts, onions, eggplants, tomatoes, turnips, potatoes and mellocos, an indigenous tuber similar to potatoes, white rice, wheat noodles, corn, barley and other foods with carbohydrates with starch. |
|
Orloff, 2014 |
América, USA (n: 200) |
Sweet foods (chocolate, candies), carbohydrates with high calories and flavors (pizza, chips) animal protein (meats, chicken), fruits, cheeses, creams, other carbohydrates, fast foods. |
Not studied. |
|
Orloff, 2016 |
América, USA (n: 83) |
Sweet foods, as chocolate, cookies, ice creams and fast foods |
Not studied. |
|
Farland, 2015 |
América, USA (n: 2022) |
45% |
Not studied. |
|
Flaxman, 2000 |
Systematic review Cravings: 21 studies, n: 6239 Aversions: 20 studies, n: 5.432
|
67% |
65% |
aVariations in the selection according to ethnic origin.
Conclusion
Cravings and food aversions are frequent phenomena that affect the selection of food during pregnancy; its etiology is still unclear. Numerous hypotheses focused on biological, cultural and anthropological approaches attempt to explain their occurrence. Although the description of food cravings and aversions during pregnancy has been studied by various authors, there is no uniformity of criteria in the modalities used for their characterization. Different types of questionnaires, the vast majority of which have not been validated, have been used to identify these phenomena. Having diagnostic tools specially designed to know the occurrence and describe the cravings and aversions during pregnancy is an important step to learn more about the relationship these changes may have in the selection of foods with nutritional status and maternal-fetal health.
Acknowledgement
This Word was supported by the University of Buenos Aires (UBACyT Code: 20020170100385BA).
References
- Academy of Nutrition and Dietetics (2014) Position of the Academy of Nutrition and Dietetics: Nutrition and lifestyle for a healthy pregnancy outcome. J Acad Nutr Diet 114: 1099–1103.
- Gernand AD, Schulze KJ, Stewart CP, West Jr KP, Parul C (2016) Micronutrient deficiencies in pregnancy worldwide: Health effects and prevention. Nat Rev Endocrinol 12: 274–289.
- Tsegaye D, Muroki NM, Kogi-Makau W (1998) Food aversions and cravings during pregnancy: Prevalence and significance for maternal nutrition in Ethiopia. Food and Nutrition Bulletin 19: 85.
- Coronios-Vargas M, Toma RB, Tuveson RV, Schutz IM (1992) Cultural influences on food cravings and aversions during pregnancy. Ecol Food Nutr 27: 43–49.
- Young AG, Pike IL (2012) A Biocultural Framework for Examining Maternal Cravings and Aversions among Pastoral Women in East Africa. Ecol Food Nutr 51: 444–462.
- Patil CL, Young SL (2012) Biocultural considerations of food cravings and aversions: an introduction. Ecol Food Nutr 51: 365–373. [crossref]
- Mahaluf ZJ, Nader NA, Correa D, Vargas J, Arraztoa V, et al. (1991) El antojo en la embarazada definición inicial. Rev. Psiquiatr clín 28: 118–125.
- Bayley TM, Dye L, Jones S, DeBono M, Hill AJ (2002) Food cravings and aversions during pregnancy: relationships with nausea and vomiting. Appetite 38: 45–51. [crossref]
- Orloff NC1, Hormes JM (2014) Pickles and ice cream! Food cravings in pregnancy: hypotheses, preliminary evidence, and directions for future research. Front Psychol 5: 1076. [crossref]
- Flaxman SM1, Sherman PW (2000) Morning sickness: a mechanism for protecting mother and embryo. Q Rev Biol 75: 113–148. [crossref]
- Weigel MM, Coe K, Castro NP, Caiza ME, Tello N, et al. (2011) Food Aversions and Cravings during Early Pregnancy: Association with Nausea and Vomiting. Ecol Food Nutr 50: 197–214.
- Placek CD1, Hagen EH (2015) Fetal Protection : The Roles of Social Learning and Innate Food Aversions in South India. Hum Nat 26: 255–276. [crossref]
- López LB, Ortega Soler CR, Pita Martín de Portela ML (2004) La pica durante el embarazo: un trastorno frecuente subestimado. Arch Latinoam Nutr 54: 17–24.
- Poy MS, Weisstaub A, Iglesias C, Fernández S, Portela ML, et al. (2012) [Pica diagnosis during pregnancy and micronutrient dificiency in Argentine women]. Nutr Hosp 27: 922–928. [crossref]
- Meyer-Rochow VB (2009) Food taboos: their origins and purposes. J Ethnobiol Ethnomed 5: 18. [crossref]
- Vasilevski V, Carolan-Olah M (2016) Food taboos and nutrition-related pregnancy concerns among Ethiopian women. J Clin Nurs 25: 3069–3075.
- Carlin A, Alfirevic Z (2008) Physiological changes of pregnancy and monitoring. Best Pract Res Clin Obstet Gynaecol 22: 801–823. [crossref]
- Purizica M (2010) Modificaciones fisiológicas en el embarazo. Rev PeR Ginecol obstet 56: 57–69.
- Ojeda González J, Rodríguez Alvarez M, Estepa Pérez J, Piña Loyola, Cabeza Poblet B (2011) Cambios fisiológicos durante el embarazo. Su importancia para el anestesiólogo. Revista Electrónica de las Ciencias Médicas en Cienfuegos 9: 484–491.
- Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A (2016) Physiological changes in pregnancy. Cardiovasc J Afr 27: 89–94. [crossref]
- Graves A (2010) Synapse. The Boston University Undergraduate Science magazine. http://www.bu.edu/synapse/2010/07/28/the-mystery-of-pregnancy-cravings/
- Irving FC (1940) The treatment of pernicious vomiting of pregnancy. Virginia Medical Monthly 67: 717–724 https://archive.org/details/virginiamedicalm67unse/page/n775.
- Flaxman SM, Sherman PW (2008) Morning sickness: adaptive cause or nonadaptive consequence of embryo viability? Am Nat 172: 54–62. [crossref]
- Hook EB (1978) Dietary cravings and aversions during pregnancy. Am J Clin Nutr 31: 1355–1362. [crossref]
- Profet M (1988) The evolution of pregnancy sickness as protection to the embryo against Pleistocene teratogens. The University of Chicago. Biology Department. Evolutionary theory 8: 177–190.
- Profet M (1995) Pregnancy sickness as adaptation: a deterrent to maternal ingestion of teratogens. Adapt Mind 327–365.
- Fessler DM (2002) Reproductive immunosupression and diet. An evolutionary perspective on pregnancy sickness and meat consumption. Curr Anthropol 43: 19–61.
- McKerracher L, Collard M, Henrich J (2016) Food Aversions and Cravings during Pregnancy on Yasawa Island, Fiji. Hum Nat 27: 296–315.
- Brown EA, Ruvolo M, Sabeti PC (2013) Many ways to die, one way to arrive: how selection acts through pregnancy. Trends Genet 29: 585–592. [crossref]
- Drewnowski A (1997) Taste preferences and food intake. Annu Rev Nutr 17: 237–253. [crossref]
- Haig D (1996) Altercation of generations: genetic conflicts of pregnancy. Am J Reprod Immunol 35: 226–232. [crossref]
- Huxley RR (2000) Nausea and vomiting in early pregnancy: its role in placental development. Obstet Gynecol 95: 779–782.
- Holland TD, O’Brien MJ (2003) On morning sickness and the Neolithic revolution. Current Anthrop 44: 707–711.
- Lumey LH (1998) Compensatory placental growth after restricted maternal nutrition in early pregnancy. Placenta 19: 105–111.
- Godfrey K, Robinson S, Barker DJ, Osmond C, Cox V (1996) Maternal nutrition in early and late pregnancy in relation to placental and fetal growth. BMJ 312: 410–414. [crossref]
- Tierson FD, Olsen CL, Hook EB (1985) Influence of cravings and aversions on diet in pregnancy. Ecol Food Nutr 17: 117–129.
- Räikkönen K, Pesonen AK, Järvenpää A-L, Strandberg TE (2004) Sweet babies: chocolate consumption during pregnancy and infant temperament at six months. Early Hum Dev 76: 139–145.
- Nordin S, Broman DA, Olofsson JK, Wulff M (2004) A longitudinal descriptive study of self-reported abnormal smell and taste perception in pregnant women. Chem Senses 29: 391–402. [crossref]
- Nordin S, Broman DA, Bringlöv E, Wulff M (2007) Intolerance to ambient odors at an early stage of pregnancy. Scand J Psychol 48: 339–343. [crossref]
- Institute of Medicine (2009) Weight Gain During Pregnancy: Reexamining the Guidelines. Washington, D.C. National Academy Press.
- Orloff NC, Flammer A, Hartnett J, Liquorman S, Samelson R, et al. (2016) Food cravings in pregnancy: Preliminary evidence for a role in excess gestational weight gain. Appetite 105: 259–265.
- Academy of Nutrition and Dietetics (2016) Position of the Academy of Nutrition and Dietetics: Obesity, Reproduction, and Pregnancy Outcomes. J Acad Nutr Diet 116: 677–691.
- Allison KC, Wrotniak BH, Pare E, Sarwer DB (2012) Psychosocial characteristics and gestational weight change among overweight, African-American pregnant women. Obstet Gynecol 2012: 878607.
- Belzer LM, Smulian JC, Lu SE, Tepper BJ (2010) Food cravings and intake of sweet foods in healthy pregnancy and mild gestational diabetes mellitus. A prospective study. Appetite 55: 609–615.
- Farland LV, Rifas-Shiman SL, Gillman MW (2015) Early Pregnancy Cravings, Dietary Intake, and Development of Abnormal Glucose Tolerance. J Acad Nutr Diet 115: 1958–1964.
- Hill AJ, Cairnduff V, McCance DR (2016) Nutritional and clinical associations of food cravings in pregnancy. J Hum Nutr Diet 29: 281–289. [crossref]
- Nyaruhucha CNM (2009) Food cravings, aversions and pica among pregnant women in Dar es Salaam, Tanzania. Tanzan J Health Res 11: 29–34.
- Patil CL (2012) Appetite Sensations in Pregnancy among Agropastoral Women in Rural Tanzania. Ecol Food Nutr 51: 431–443.
- Qureshi Z, Khan R (2015) Diet intake trends among pregnant women in rural area of Rawalpindi, Pakistan. J Ayub Med Coll Abbottabad 27: 684–688.