A 52-year female was admitted with a complaint of palpitation. On current admission to our hospital, she is mildly dyspneic, impaired heart sounds and blood pressure of 95/60 mmHg. Electrocardiography revealed atrial fibrillation with heart rate of 120/min. She did not have any chronic illness, such as diabetes mellitus, hypertension. Transthoracic echocardiography was performed and found normal. Transesophageal echocardiography was performed for electrical cardioversion and there was no thrombus in left atrial appendage.
The rhythm of atrial fibrillation returned to sinus rhythm after cardioversion. Coronary angiography was performed because of suspected ischemia. In coronary angiography, left anterior descending artery and circumflex artery was normal and Right Coronary Artery (RCA) arose from the ascending aorta with a high takeoff (approximately 5 cm above sinotubuler junction, Figure 1). RCA seemed such a saphenous graft (Figure 2).
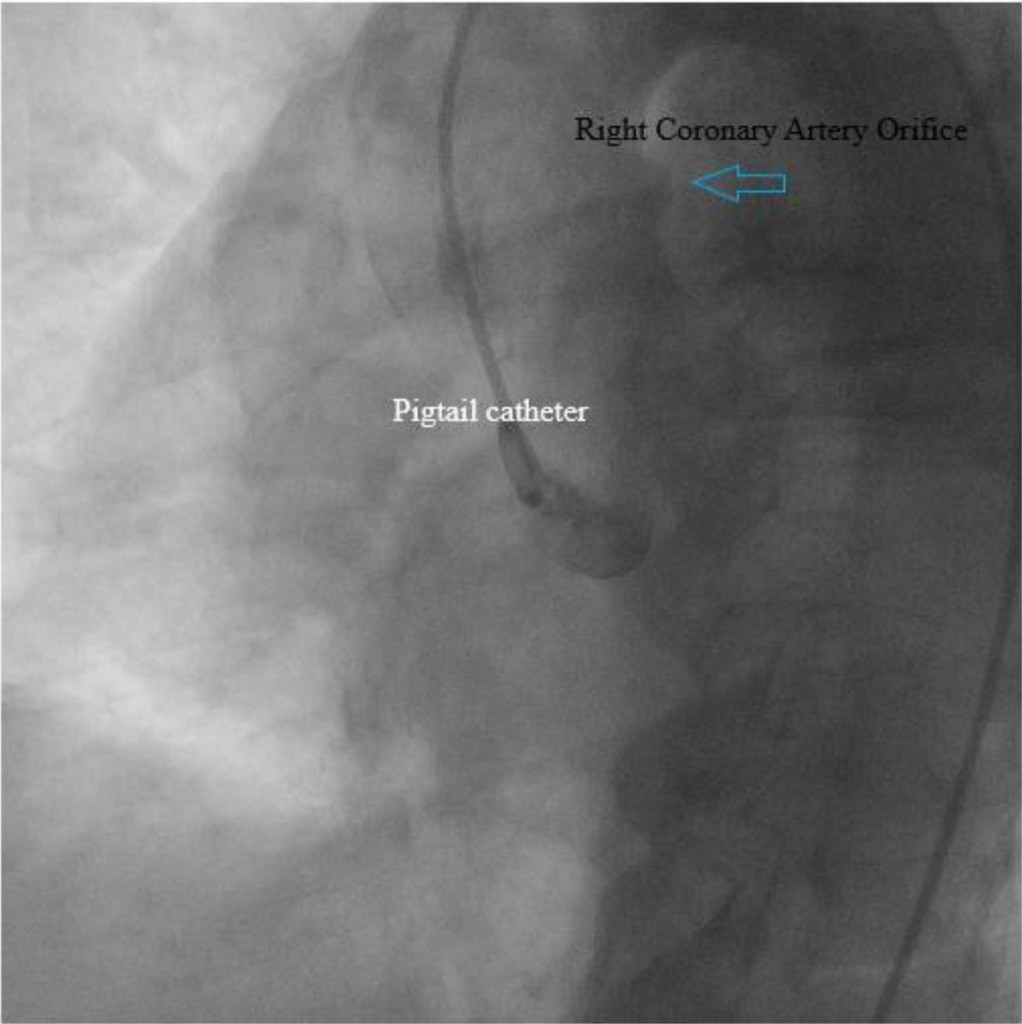
Figure 1. Right Coronary Artery (RCA) arose from the ascending aorta with a high takeoff.

Figure 2. RCA seemed such a saphenous graft
In studies RCA origin abnormality, 0, 04-0, 46% frequency has been found [1, 2]. Ayalp et al found that frequency of occurrence of the anomalous RCA in the Turkish population is 0, 09% [3]. However, anomalous origin of the RCA from the left side of the ascending aorta is very more rare and only a few cases have been reported [4]. In our case, RCA was arising from the left side of the ascending aorta, approximately 5 cm above the sinotubuler junction.
In anomalous origin of the RCA might be compressed between the aorta and pulmonary trunk and may the reduction of coronary blood flow. As a result, cardiac arrhythmia and sudden death can be seen.
References
- Cieslinski G, Rapprich B, Kober G (1993 ) Coronary anomalies: incidence and importance. Clin Cardiol 16: 711–715. [Crossref]
- Garg N, Tewari S, Kapoor A, Gupta DK, Sinha N (2000) Primary congenital anomalies of the coronary arteries: a coronary arteriographic study. Int J Cardiol 12: 39–46.
- Ayalp R, Mavi A, Sercelik A, Batyraliev T, Gumusburun E (2002) Frequency in the anomalous origin of the right coronary artery with angiography in a Turkish population. Int J Cardiol 82: 253–257. [Crossref]
- Motamedi MH, Hemmat A, Kalani P, Rezaee MR, Safarnezhad S (2009) High take-off of right coronary artery: an extremely rare case of RCA anomaly. J Card Surg 24: 343-345. [Crossref]