Introduction
Fascial Manipulation® (FM®), a modality of manipulative physical therapy originated with an Italian physical therapist, Luigi Stecco, is classified roughly into two types, i.e., FM® for musculoskeletal dysfunction and FM® for internal dysfunction. In the FM® for musculoskeletal dysfunction, a route to fascial compensation is revealed from results of inquiries, exercise test, and palpation test, and then points of Center of Coordination (CC) and Center of Fusion (CF), which are associated with the compensation, are treated. In general, FM® is therapeutically designed to recover the feature of sliding of the deep fascia and to improve patient’s pain, Range of Motion (ROM), and muscle strength [1,2]. Focusing on low back pain, which physical therapists and physicians frequently encounter and treat in clinical settings, practical cases of FM® for musculoskeletal dysfunction are mentioned through 2 case reports in this article.
Practical cases of FM®
Case 1 – Ascending Fascial Compensation
General information
A 32-year-old woman, a care worker, has started playing badminton since her age of 10 years. At present she plays badminton about once a month. The physician who examined the patient made a diagnosis of myofascial low back pain, as any distinct finding on X-ray or MRI image was observed, and treated the patient by physical therapy.
Inquiries
The chief complaint of the patient was left low back pain (at the level of the 4th-5th lumbar vertebrae). She had the pain 6 months ago without manifestation by any overt symptom. It was caused by the long-time standing position and assistance for transfer activities during the work. She had no pain in her sitting or lying position. The most severe pain showed score 7 based on the Numerical Rating Scale (NRS). The patient has always been feeling physical disorder at her medial left scapula since 3 months ago (NRS: 1-2).
Inquiries about past histories revealed that the patient had fracture of the distal end of the right radius one year ago and received the 4-week treatment by plaster fixation. She had pain in the lateral region of the left elbow joint 10 years ago. The longest past history was left ankle joint inversion sprain 17 years ago. It was treated by plaster fixation for 3 weeks, and it needed 4 months to have fully recovered. The patient had no dysesthesia at any terminal point (head, fingers, or toes), surgical history, or non-contributory internal past history.
Hypothesis
In FM® a hypothesis is built up regarding a route to fascial compensation from temporal/spatial viewpoints on the basis of the results of inquiries [1]. Figure 1 shows a timeline of information, which was collected on inquiries about the chief complaint (the most severe pain at present), its associated pain, and past histories of he patient. Figure 2 shows a body chart including the same information as that in Figure 1.
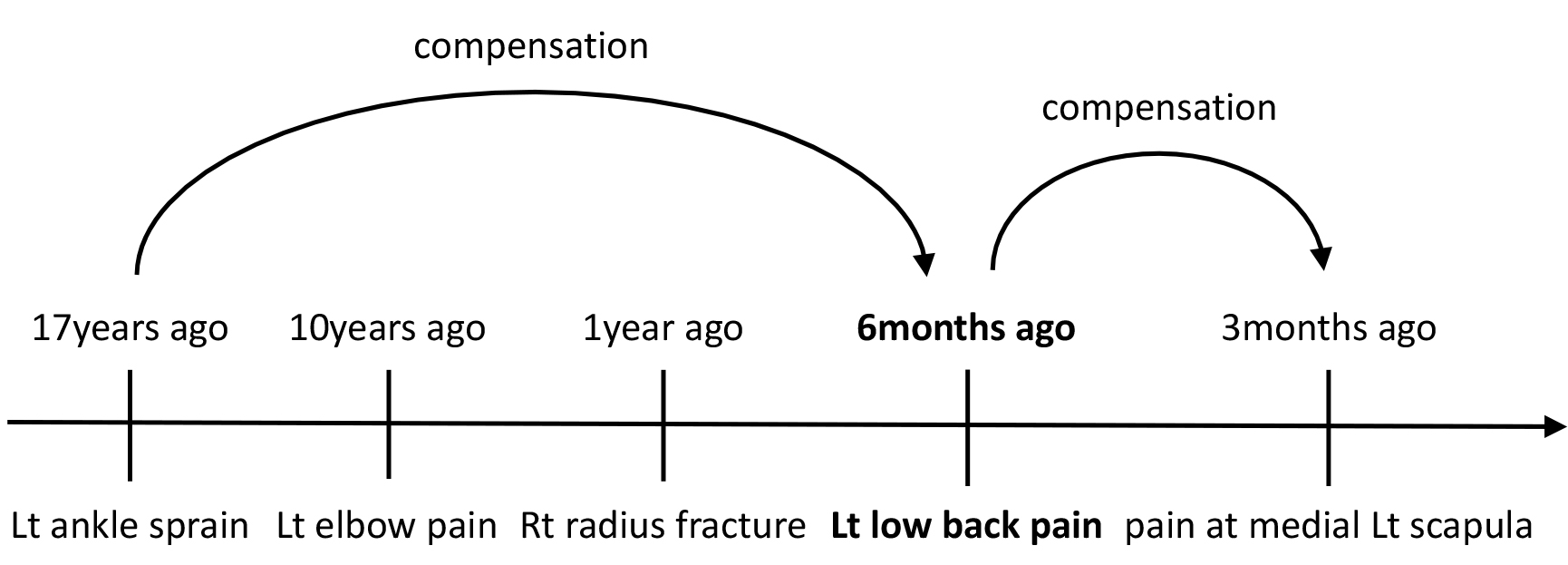
Figure 1. A timeline (case 1).
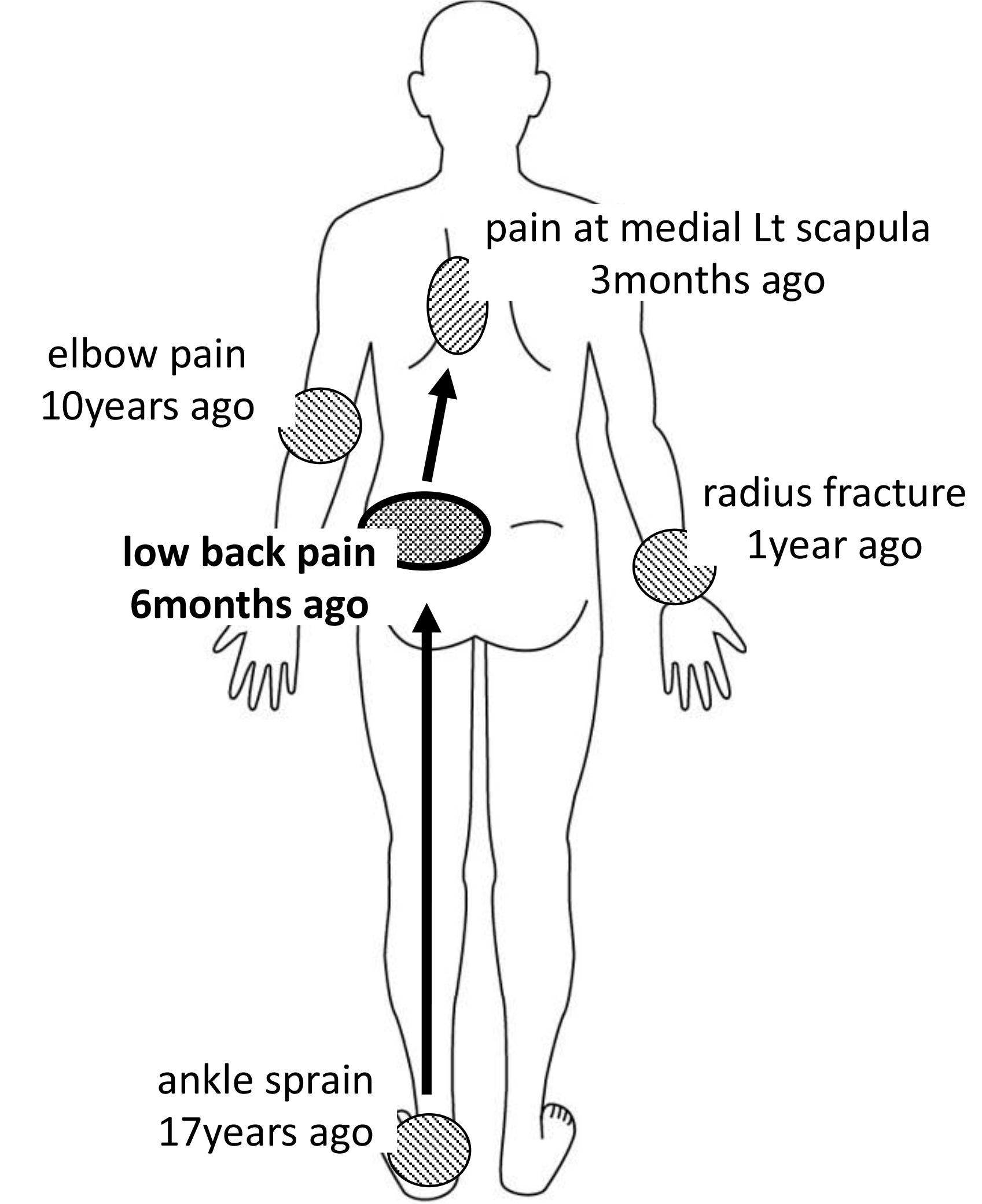
Figure 2. A body chart (case 1).
Several hypotheses can be built up about the route to fascial compensation from Figures 1 and 2. When the occurrence of low back pain as chief complaint in a standing position is taken into consideration, however, insufficient sliding of the deep fascia may have been induced by long-term plaster fixation of the left ankle during the treatment of ankle inversion sprain [1], probably leading to the ascending fascial compensation and left low back pain in the patient.
Evaluation by the therapist
(1) Exercise test
On the basis of the above-mentioned hypothesis, two segments, i.e., pelvic girdle (PV) and ankle joint (TA), were selected for exercise test. As a result, the same type of pain (NRS: 6) as the chief complaint, was induced to PV by pelvic anterior tilt movement in a standing position, while no marked finding was observed in TA.
(2) Palpation test
The segments selected first for palpation test were PV, i.e., segment of the chief complaint, TA, i.e., the origin of the fascial compensation, and the hip joint (CX) localized between the PV and TA segments. As for these segments, all CC points (anterior, rearward, inward, outward, internal rotation, and external rotation) were palpated. As a result of palpation test for CC, there was no difference in the number of the points at which findings of high density were observed, or the degree of high density among sagittal planes (anterior/rearward), frontal planes (inward/outward), and horizontal planes (internal rotation/external rotation), suggesting that fascial diagonal or fascial spiral, rather than fascial arrangement, is involved with fascial compensation. Therefore, palpation test for CF points of the above-mentioned three segments was conducted, revealing that CF of left RE-LA-PV1 (Figure 3) showed a large area of high density and had remarkable pain associated with irradiating pain. As other findings, left RE-LA-TA2 and left Re-LA-CX showed moderately high density.
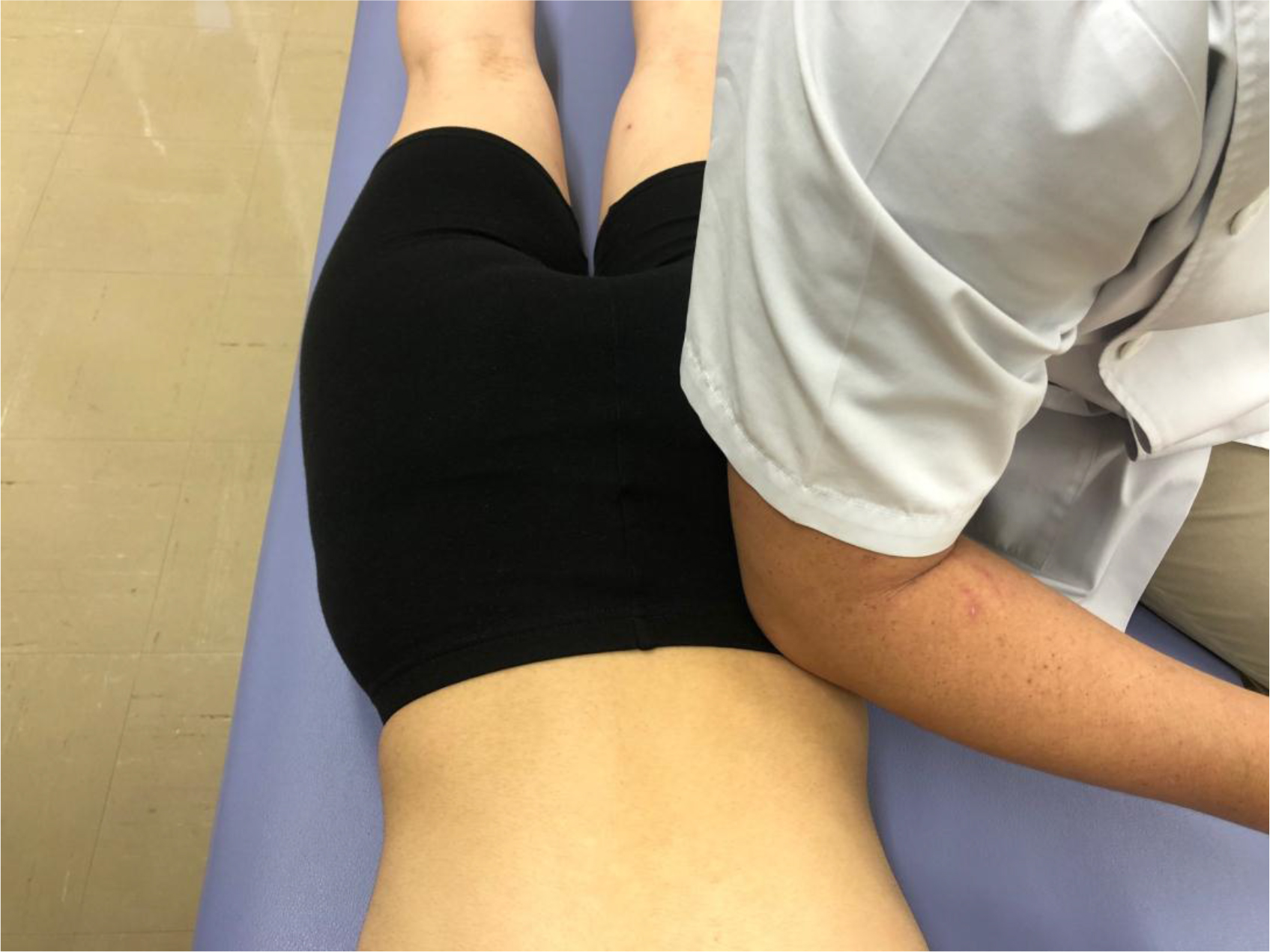
Figure 3. Palpation and treatment for RE-LA-PV1 CF.
It was considered from the results of palpation test for the PV, TA, and CX that a left RE-LA diagonal or a left AN-ME spiral was involved with the patient’s chief complaint. Faced with this situation, CF points were palpated at RE-LA and AN-ME of segments of toes (PE) and knee joint (GE) on the left side and low back (LU), and thorax (TH) on both sides. As a result, left RE-LA-TH showed findings of a large area of high density, and left RE-LA-PE3 and RE-LA-LU on both sides showed findings of moderately high density. It was judged from these findings that a left RE-LA diagonal was mostly involved with the patient’s chief complaint. Then, the patient was treated based on the evaluation.
Treatment
In FM® the CC/CF points treated are selected, and routes to fascial compensation are taken into consideration even on determining the treatment order [1, 2]. In general, since CC/CF points of segments with the chief complaint frequently show serious pain, the treatment rarely starts with the segments. In this patient the treatment started with RE-LA-PE3 (Figure 4) and RE-LA-TA2 (Figure 5), which were localized at the left ankle joint, i.e., the estimated origin of fascial compensation. As a result of the judgment of the efficacy of the treatment of these CF points from the exercise test results, pain on the pelvic anterior tilt movement was reduced to 50% of that before the treatment. Consequently, the hypothesis built up was judged to be valid, and the treatment of the RE-LA diagonal was advanced.
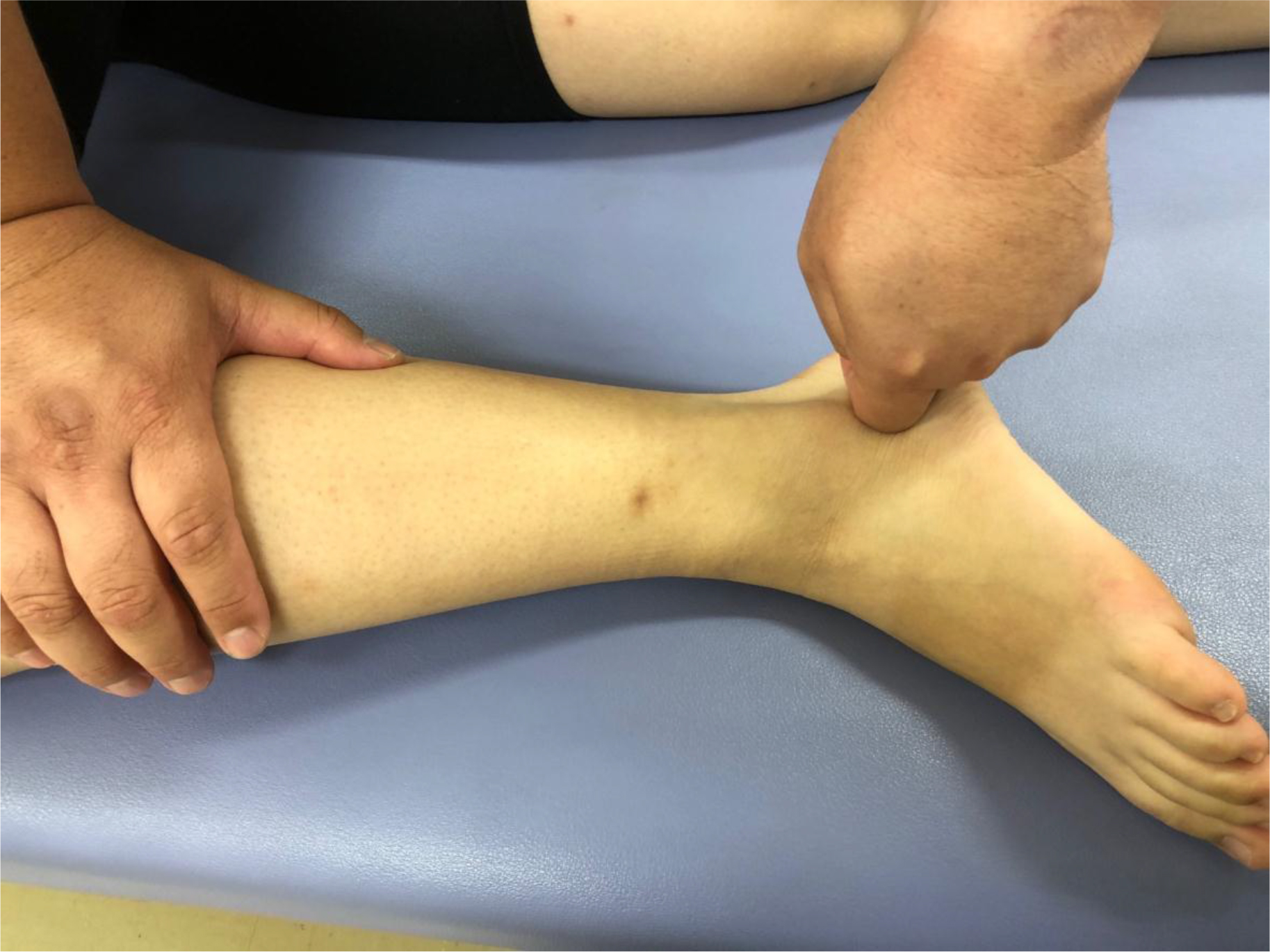
Figure 4. Palpation and treatment for RE-LA-PE3 CF.

Figure 5. Palpation and treatment for RE-LA-TA2 CF.
CF points of the left RE-LA-PE3 were treated first, followed by those of the left RE-LA-TA2, left RE-LA-TH, left RE-LA-LU, left RE-LA-CX, left RE-LA-PV, and right RE-LA-LU, in that order. After all these CF points were treated, exercise test was conducted again. As a result, the left low back pain on pelvic anterior tilt movement was fully resolved, and the patient had no pain on any other low back movement.
Case 2 – Descending Fascial Compensation
General information
A 54-year-old man, a viola player, has been practicing the viola for 4-8 hours almost every day since he was a child. According to his reminiscence, he has taken the same posture, i.e., putting the viola on his left shoulder and settling it with his neck, for a long time. The physician who examined him recognized the narrow intervertebral space of L3/4 and L4/5 on X-ray images, made a diagnosis of lumbar disc disease, and treated the patient by physical therapy.
Inquiries
The chief complaint of the patient was left low back pain (at the level of the 1st-3rd lumbar vertebrae). He had the pain 6 years ago without manifestation by any overt symptom. He had the pain particularly during getting up at the time of rising from his bed and in a long-time sitting position. The most severe pain showed score 5 based on NRS.
The patient has been suffering from left shoulder pain (NRS: 4) since 7 years ago, as well as the left low back pain. Inquiries about past histories revealed that the patient had left elbow joint pain 10 years ago, right elbow joint pain 12 years ago, and neck pain 20 years ago. He had no past history of either lower extremity. He had no headache or numbness in any finger/toe. He had no surgical history or noncontributory internal past history.
Hypothesis
Figure 6 shows a timeline of information, which was collected on inquiries about the chief complaint, its associated pain, and past histories of the patient. Figure 7 shows a body chart including the same information as that in Figure 6. In this patient, his past histories were restricted to his upper body, and he had low back pain as the chief complaint in such an occasion as that without body weight bearing on lower extremities; it occurred during getting up and taking a sitting position for a long time. Based on these situations, it was considered that the patient took a specific posture because of playing a viola and the overuse of the neck and upper extremities led to insufficient sliding of the deep fascia [1], which was responsible for the descending fascial compensation.
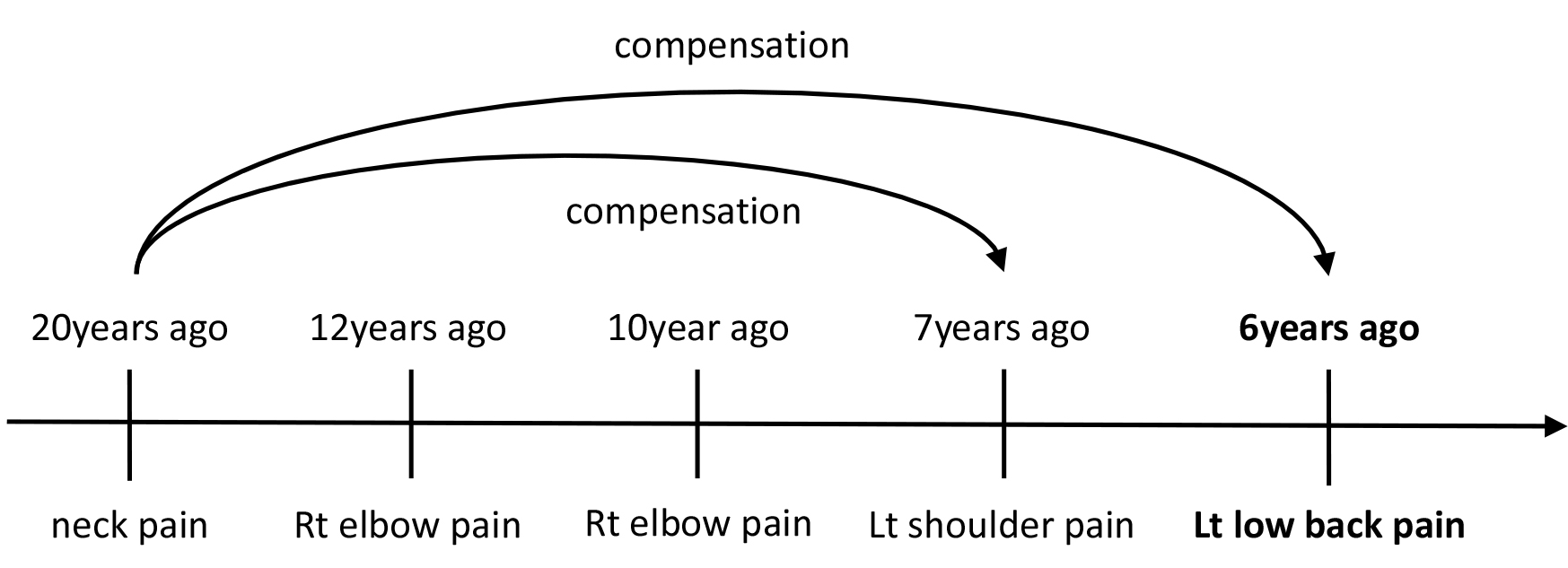
Figure 6. A timeline (case 2).
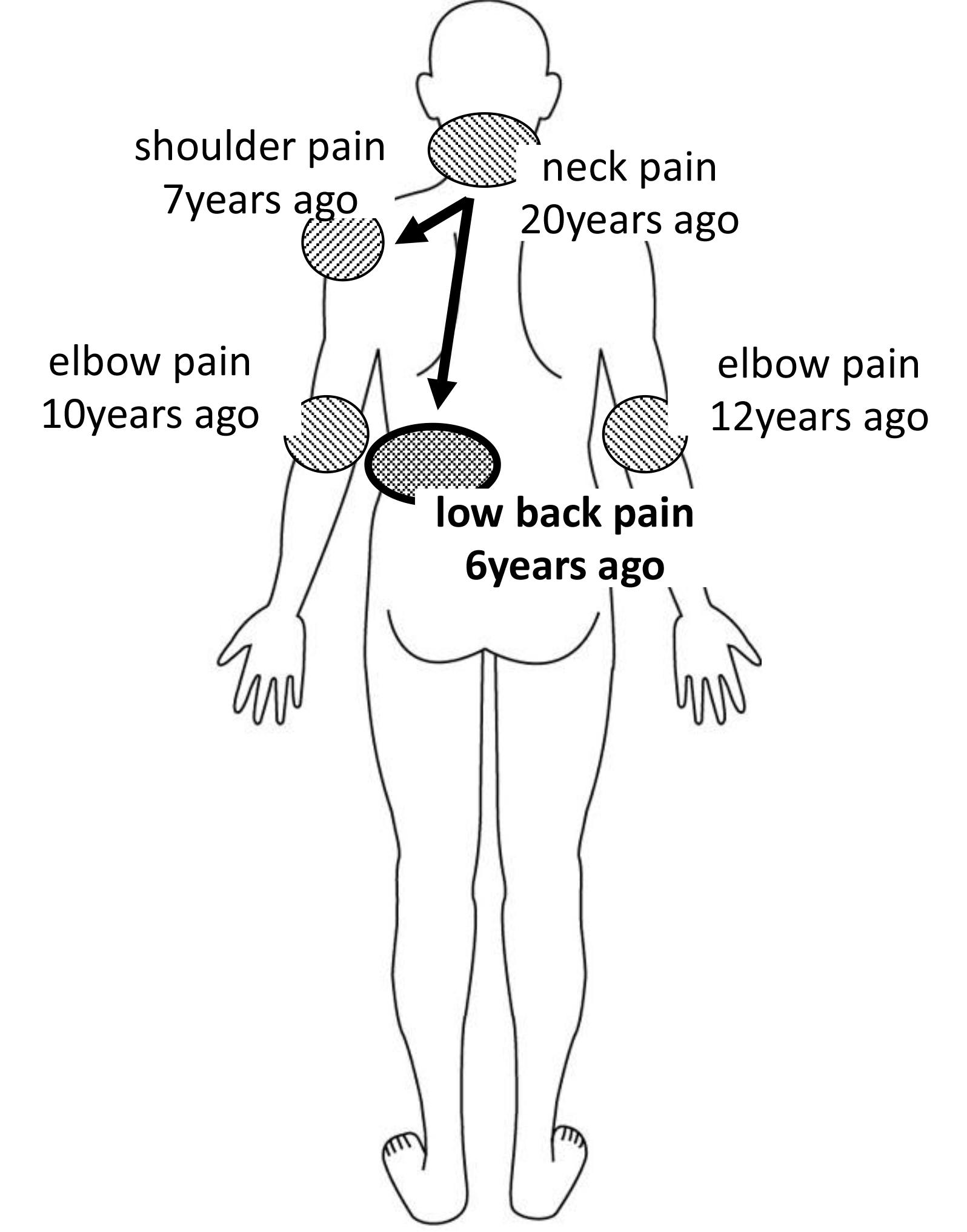
Figure 7. A body chart (case 2).
Evaluation by the therapist
(1) Exercise test
On the basis of the above-mentioned hypothesis, two segments, i.e., low back region (LU) and shoulder joint (HU), were selected for exercise test. Consequently, low back pain was induced as a chief complaint by extension movement and right flexion movement of the low back region. On the other hand, shoulder pain was induced to the same site as that where the patient felt pain during abduction movement of the left shoulder. ROM on active movement was 120°.
(2) Palpation test
The segments selected first for palpation test were LU, i.e., the segment of chief complaint, the cervical vertebra (CL) involved with the longest past history, and HU, i.e., the segment of its associated pain. As for these segments, all 6 CC points were palpated. As a result of palpation test, RE-CL on both sides (Figure 8) and left RE-LU (Figure 9) showed high-density areas, and had remarkable pain associated with irradiating pain. As other findings, RE-HU and AN-LU on the left side and right RE-LU showed moderately high density. When the frequency of high density was compared among the sagittal, frontal, and horizontal planes, it was highest on the sagittal planes.

Figure 8. Palpation and treatment for RE-CL CC.

Figure 9. Palpation and treatment for RE-LU CC.
From the results of palpation test for LU, CL, and HU, it was judged that left fascial arrangement on the sagittal plane was most involved with the patient’s chief complaint. To find latent CC points, anterior (AN) and rearward (RE) CC points of segments of the shoulder girdle (SC), thorax (TH), and pelvis (PV) on both sides were palpated. As a result, RE-TH, RE-SC, and AN-PV on the left side showed findings of moderately high density.
Treatment
The treatment started with the CC points of the RE-TH of the adjacent TH segment (Figure 10) because of remarkable tenderness in CC points of CL (RE-CL on both sides), i.e., the estimated origin of fascial compensation. The exercise test following the treatment of the CC points revealed that the pain on low back extension and right low back flexion decreased to 50% of that before treatment. Furthermore, the pain during shoulder abduction movement was reduced to 20% of that before treatment, and the restricted ROM was almost resolved. From the results, the built-up hypothesis was judged to be valid, and treatment of the points on the sagittal planes was advanced. CC points of the left RE-TH were treated first, followed by those of the left RE-SC, RE-CL on both sides, left RE-HU, RE-LU on both sides, and left AN-LU, in that order. When RE-CL points were palpated again after the treatment of the RE-SC, tenderness was reduced. Therefore, they were included in the subjects of treatment. After all the above-mentioned CC points were treated, exercise test was implemented again. As a result, the patient had no pain in his low back or shoulder during any movement.

Figure 10. Palpation and treatment for RE-TH CC.
Conclusion
In this article the treatment using FM® for 2 patients with low back pain was surveyed. They had left low back pain in common. Particularly noteworthy is the fact that they were different from each other regarding the segments evaluated and the CC/CF points treated despite the feature common to them. It is important for implementation of the treatment appropriate for the individual patient to collect information about pain at present and in the past as accurately as possible on inquiries. On the occasion of information collection, specific attention should be paid to trauma, immobilization, and overuse, because they may lead to increased mucosity associated with aggregation (high density) of hyaluronic acid in the deep fascia ad to adversely influence the sliding system of the deep fascia [1]. It should also be mentioned that setting-up of the hypotheses about routes to fascial compensation on the basis of information collected on inquiries before the start of exercise test and palpation test was important for evaluation and treatment to proceed smoothly. This article did not describe any concrete method of exercise or palpation test or position of each point of CC/CF as space is limited. The author would be obliged if the readers would be confirmed in FM®-related publications.
References
- Luigi Stecco, Antonio Stecco (2018) Fascial Manipulation Practical Part – First Level. Padova: Piccin Nuova Libraria S.p.A.
- Luigi Stecco, Carla Stecco (2019) Fascial Manipulation Practical Part – Second Level. Padova: Piccin Nuova Libraria S.p.A.