A 24-year-old right dominant male threw a softball extremely hard from outfield. A loud, crackingnoise was accompanied by pain and inability to lift his right arm. Radiographs performed in ED revealed a severe displaced, comminuted fracture of the right humerus known as a “thrower’s fracture” (Figures 1,2). The patient was a healthy, recreational athlete. A blood test, bone scan, and MRI all revealed negative results for bone pathology prior to surgical open reduction internal fixation (ORIF) of the right humerus (Figure 3).
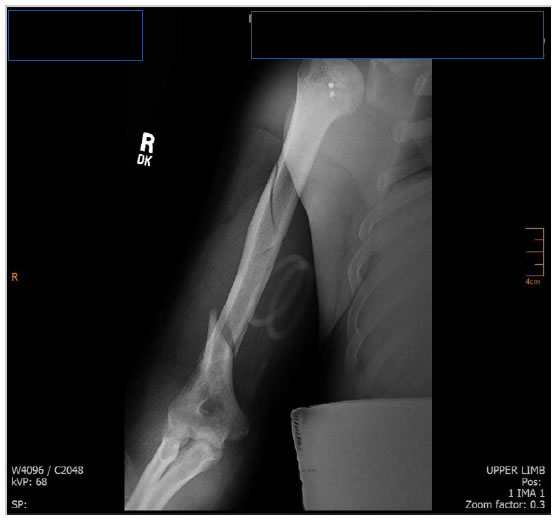
Figure 1. A-P Radiograph with comminuted fracture of right humerus.
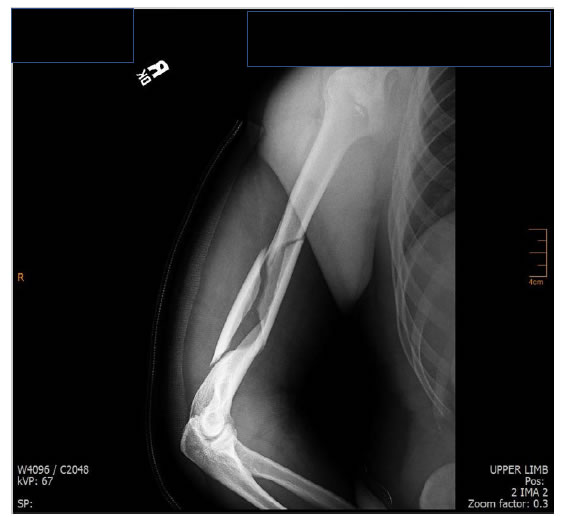
Figure 2. IR-AP of Right humerus.
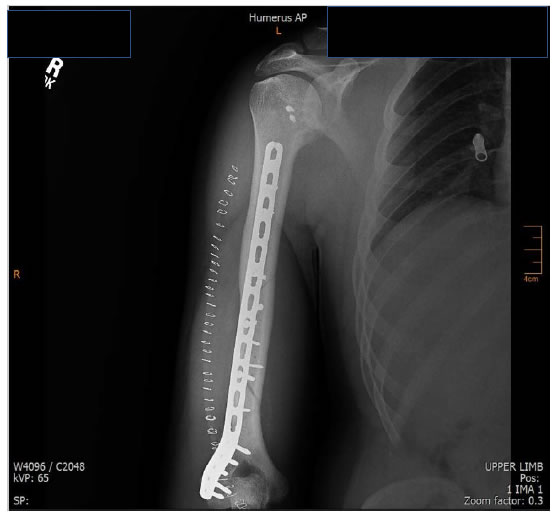
Figure 3. Post-surgical A-P radiograph.a
Thrower’s fracture, somewhat rare, is an acute fracture of the mid-to-distal third of the humeral diaphysis during a forceful throwing motion, usually involving an excessive torque during the cocking and acceleration phase of motion [1, 2]. The internal rotation of the latissimus dorsi, subscapularis, and pectoralis major all contribute to the strong internal rotation force. During the cocking and throwing phase, a torsional force is applied to the humeral insertion of these muscles while the distal humerus is external rotation, causing a spiral type fracture. Thrower’s fracture is seen more in ages 20s-30s or recreational athletes, who often lack cortical hypertrophy seen in professional pitchers [1, 2] rarely is the radial nerve, involved, but if injured, usually heals without surgical involvement [1, 2].
No post-op complications or radial nerve involvement were noted. A sling was worn for 2 weeks and ROM began at 4 weeks. He resumed light duty work at 2 months. Full ROM, less 3ºextension was obtained. At 3 months post-surgery, he resumed gym workouts, but no recreational softball.
References
- Colapinto MN, Schemitsch EH, Wu L (2006) Ball-thrower’s fracture of the humerus. Canadian Med Assc J 175:33.
- Miller A, Dodson CC, Ilyas AM (2014) Thrower’s fracture of the humerus. Orthop Clin North Am 45:565-569.