Abstract
Introduction: Coronavirus disease of 2019 started started in Wuhan China as an epidemic causing pneumonia-like illness. It became a global pandemic in a period of two months. On January 30, 2020, the World Health Organization (WHO) declared the outbreak of COVID-19 as the sixth global public health emergency (PHEIC), and on March 11, 2020, the WHO declared COVID-19 a pandemic. The waves in the epidemiological curve of the pandemic show the the progression of the pandemic. Our study aims at evaluating the the patient characteristics in first and second curve of COVID-19 pandemic.
Materials and Methods: We conducted a prospective study of all hospitalized cases of SARS COV-2 infection in KRL Hospital Islamabad, admitted between March 2020 and February 2021. All patients admitted upto August 2020 were considered in 1st wave & all those admitted from September 2020 to February 2021 were considered in 2nd wave which divided the study groups into two equal parts i.e., 6 months.
Results: In this study, the average length of stay in both waves was similar (10 days). The second wave of the pandemic inflicted younger patients greater than the first wave of the pandemic. The difference of severity of disease in the patient presenting in the first and second waves was insignificant (p > 0.05).
Conclusion: COVID-19 cases presented differently in both first and second waves of COVID-19 pandemic. The comparison of case presentation and severity of disease may help the healthcare professionals and epidemiologists to valuate the treatment and management methods. It may highlight the effectiveness of administrative aspects of controlling the pandemic.
Introduction
Coronavirus-19 (COVID-19), produced by the acute respiratory tract coronavirus 2 (SARS-CoV-2), has become a global epidemic, posing a serious health threat worldwide. Several countries have seen the pattern of two reported cases, the first wave in spring and the second in late summer and autumn [1-3]. On January 30, 2020, the World Health Organization (WHO) declared the outbreak of COVID-19 as the sixth global public health emergency (PHEIC), and on March 11, 2020, the WHO declared COVID-19 a pandemic [4]. The first case of COVID-19 was reported from Karachi on February 26, 2020, when the estimated population of Pakistan was 204.65.3,4 million [5]. As a result of the outbreak, the government introduced a series of rigorous prevention measures, including home confinement, followed by a three-month period of increased social networking, performance and hard work. With social life in the country it was back to normal, without the obligation to wear a mask and keep the public space safe. Unfortunately, the number of patients with COVID-19 began to skyrocket in August and a month later it showed the same numbers as in April. This has forced the government to reinstate drastic measures to prevent, including the closure of facilities and facilities, the closure of parks, restaurants, cultural and sports activities, and the curfew. The number of cases in Pakistan has continued to grow since then, sometimes downwards, and at the time of writing this article seems to be declining slightly. The second wave of COVID-19 was predicted months ago and already existed in some countries [6]. After the relaxation of the measures in the summer, the second wave began in mid-September 2020 and expanded until March 2021 [7]. While some countries have a second wave that is much better than the first. Meanwhile more than 20,000 people have died compared to less than 10,000 across the first wave, which is a clear indication that the medical services at hospitals were second only around [8].
This study investigated the severity and characteristics of the two waves in hospitalized patients in Islamabad.
Material & Methods
We conducted a prospective study of all hospitalized cases of SARS COV-2 infection in KRL Hospital Islamabad, admitted between March 2020 and February 2021.
All patients admitted unto August 2020 were considered in 1st wave & all those admitted from September 2020 to February 2021 were considered in 2nd wave, which divided the study groups into two equal parts i.e. 6 months.
All the patients who were hospitalized with diagnosis of SARS-COV-2 (Covid Pneumonia) were included in the study. Those with suspected SARS-COV-2 infection but no laboratory confirmation were excluded from the study. SARS-COV-2 infection was confirmed using RT-PCR using swab samples from upper respiratory tract (nasopharyngeal / oropharyngeal swabs).
The Ethical Review Board, KRL Hospital Islamabad, approved this study.
Results
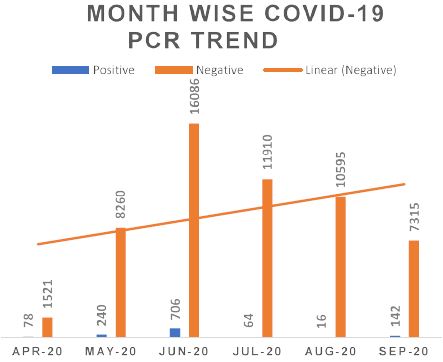
Figure 1: (1st wave) showing month wise data of all COVID-19 PCR tests conducted and positivity rate for COVID-19 infection. 57027 tests performed till 30th September 2020. COVID-19 PCR positivity rate was 2.1% which equal to national positivity rate.
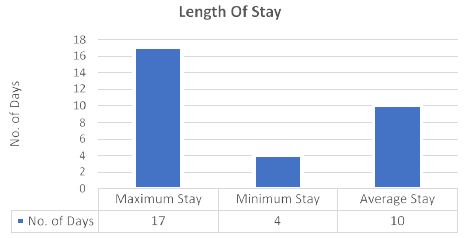
Figure 2: (1st wave)The average length of stay was 10 days with high recovery rate at 99%.
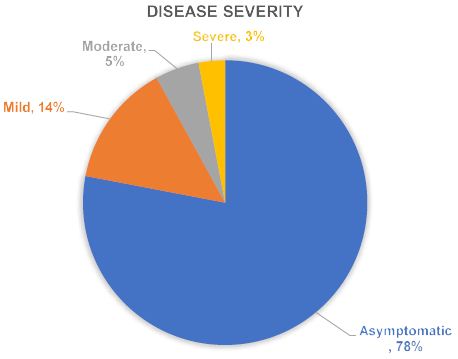
Figure 3: (1st wave) Asymptomatic: With no symptoms, only PCR positive. Mild Symptoms: Fever (1000F – 1020F) shortness of breath on exertion, body aches, maintaining>95% oxygen saturation at room air. Moderate: Fever (1010F – 1030F) shortness of breath, myalgia’s, oxygen saturation at 3-5 liters max with NIV nasal cannula. Sever Disease illness: Fever (1010F – 1030F) shortness of breath, body aches, myalgia, prominent changes on imaging and difficulty in maintaining blood oxygen saturation with NIV nasal cannula (highly oxygen dependent).
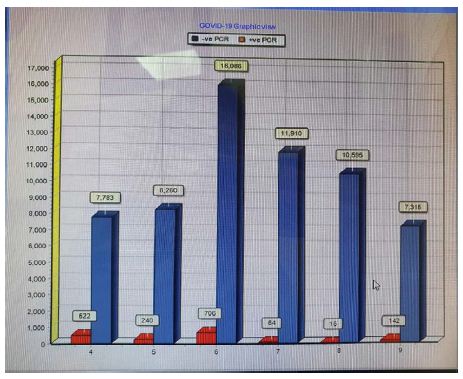
Figure 4: Second Wave showing month wise data of all COVID-19 PCR tests conducted and positivity rate for COVID-19 infection.
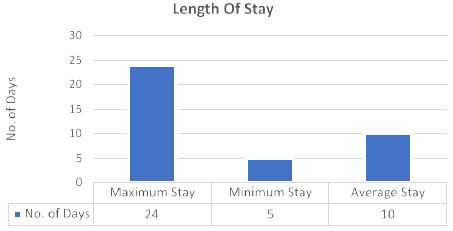
Figure 5: (Second Wave) The average length of stay was 10 days with high recovery rate at 99%.
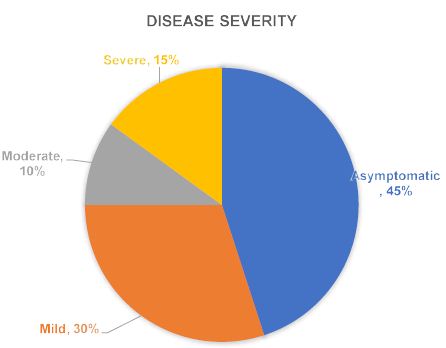
Figure 6: (Second Wave) Asymptomatic: With no symptoms, only PCR positive. Mild Symptoms: Fever (1000F – 1020F) shortness of breath on exertion, body aches, maintaining >95% oxygen saturation at room air. Moderate: Fever (1010F – 1030F) shortness of breath, myalgia’s, oxygen saturation at 3-5 liters max with NIV nasal cannula. Sever Disease illness: Fever (1010F – 1030F) shortness of breath, body aches, myalgia, prominent changes on imaging and difficulty in maintaining blood oxygen saturation with NIV nasal cannula (highly oxygen dependent).
Discussion
Pakistan is one of the most populous countries globally, which had about 0.9 million cases of COVID-19 until now [9]. The time span for the first wave ranged till August 2020, and that of the second was from September 2020 to February 2021, and both these waves had their peak for around about one month in which we reported the highest cases. It was observed that there was an inverted U wave pattern of seroprevalence of SARS CoV-2 infection; the same pattern was observed in another study [10]. One of the significant thing that came into account is the age of patients who were infected by the deadly and lethal virus, which was surprisingly younger people, children, and women, as also revealed by Fan G. et al [11] which may be due to poor compliance with social distancing and other Standard Operating Procedures (SOPs) may have resulted in spreading of the pandemic in younger patients. This may be due to some myths that the virus can only infect the elderly, which is a foolish thing to say, but these young people can also infect their own elderly, and when they do, the prudent time will be gone.
The high incidence of seropositive COVID-19 in younger patients resulted in depression in the case fatality rate, as shown by Iftimie S et al. [12]. There were many reasons for decreased case fatality rate, which includes firstly, the younger the patients, the better would be the immunity; secondly, now we had better understandings, perceptions, and comprehension of pathophysiology of plague, thirdly, Dexamethasone was used frequently because of the results published by Horby PW et al. [13], and Remdisivir was also proved to be a benchmark in preventing death and mitigating the hospital stay of the patient, which other researchers also witnessed [14] and last but not least the Planned and organized effort of Government in implementing the smart lock-down policy was worth it. However, the treatment plan of COVID-19 patients was changed in the second wave, so it was impossible to compare the effectiveness of the management plan.
Although we had a high proportion of patients having moderate and severe symptoms in the second wave as compared to the first wave, which is contrary to other studies [15-16-17], the recovery rate wasn’t changed despite the higher number of severe seropositive COVID-19 patients, which is mainly due to reasons mentioned above. At the same time, hospital stay remained consistent in both of the waves.
As Pakistan conducted lesser Real-Time Polymerase Chain Reaction (RT-PCR) tests than other major countries of the world, it would be useless to compare the number of the confirmed cases of SARS CoV with that of foreign countries. However, considering the number of deaths in western countries is much more than in Pakistan, albeit the exact reason is not known, genetic makeup could also be the reason for significantly fewer deaths [18].
This study has some limitations, including a small sample size and uni-centric research, due to which we couldn’t apprehend the bigger picture. And due to limited resources and restricted contact tracing measures, we can only locate the tip of the iceberg, but the real problem which should be addressed wasn’t in our hands. The cases of re-infection couldn’t be examined in detail because of the lack of facilities that depict viral genome, and the determinants of infectivity in first and second waves couldn’t be studied in detail. And as we know, there was a whole different set of medications in treatment for COVID-19 patients in both waves, so that will be unfruitful to compare the effectiveness of medicines.
In summary, we had a slightly higher seroprevalence of COVID-19 in the second wave; it was more common in younger patients. At the same time, the hospital admission tenure in both of the waves was the same. There were more severe and moderate category cases, but now, the mortality rate hasn’t changed because of having a better approach towards this ailment. Pre-existing comorbidities in the second wave were the same as that of the first one. Developing countries like Pakistan cannot afford different waves of COVID-19 because our healthcare is always working on its total efficiency; any more addition will result in the collapse of the system. Our only way out from this is to vaccinate the mob as much as possible so that the level of herd immunity can be achieved. Being healthcare professionals, our moral and ethical obligation is to spread awareness about the disease and the vaccine. And we also have to break myths which is one of the biggest obstacles in not getting the jab.
Conclusion
Covid-19 pandemic struck the world extremely hard in terms of world wide spread and mortality. The pattern of COVID-19 spread and severity varied during first and second waves of the pandemic. The account of the changes in the behavior of the waves of the pandemic is crucial for the evaluation of the preparedness for the pandemic. The evolution of the pandemic can be halted by active surveillance and adequate measures to bring the epidemiologic curve to the baseline.
References
- Vahidy FS, Drews AL, Masud FN, Schwartz RL, Boom ML, Phillips RA, et al. (2020) Characteristics and outcomes of COVID-19 patients during initial peak and resurgence in the Houston metropolitan area. JAMA 324: 998–1000. [crossref]
- Fan G, Yang Z, Lin Q, Zhao S, Yang L, He D. (2020) Decreased case fatality rate of COVID-19 in the second wave: a study in 53 countries or regions. Transbound Emerg Dis. Epub ahead of print. [crossref]
- Saito S, Asai Y, Matsunaga N, Hayakawa K, Terada M, Ohtsu H, et al. (2020) First and second COVID-19 waves in Japan: A comparison of disease severity and characteristics: Comparison of the two COVID-19 waves in Japan. J Infect. S0163-4453(20)30693-9. [crossref]
- World Health Organization. Naming the coronavirus disease (COVID-19) and the virus that causes it. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it. Accessed March 16, 2020.
- Government of Pakistan; Ministry of Planning, Development & Special Initiatives; Pakistan Bureau of Statistics. Pakistan Statistical Year Book 2018 (Provisional).
http://www.pbs.gov.pk/sites/default/files//PAKISTAN%20STATISTICAL%20YEAR%20BOOK%202018.pdf. - Renardy M, Eisenberg M, Kirschner D. (2020) Predicting the second wave of COVID-19 in Washtenaw County, MI. J Theor Biol. 507: 110461. [crossref]
- Vicente Soriano, Pilar Ganado-Pinilla, Miguel Sanchez-santos, et al. (2021) Main differences between the first and second waves of COVID-19 in Madrid, Spain. International Journal of Infectious Diseases, 105 (2021) 374-376. https://doi.org/10.1016/j.ijid.2021.02.115. [crossref]
- Graichen H. (2021) What is the difference between the first and the second/third wave of Covid-19? – German perspective. J Orthop. Mar-Apr;24:A1-A3. doi: 10.1016/j.jor.2021.01.011. Epub 2021 Jan 27. [crossref]
- Official Updates Coronavirus – COVID-19 in Pakistan (https://www.covid.gov.pk/)
- Hattori T, Saito A, Chiba H, Kuronuma K, Amishima M, Morinaga D, Shichinohe Y, Nasuhara Y, Konno S. (Mar. 2021) Characteristics of COVID-19 patients admitted into two hospitals in sapporo, Japan: Analyses and insights from two outbreak waves. Respiratory Investigation 1;59(2):180-6. [crossref]
- Fan G, Yang Z, Lin Q, Zhao S, Yang L, He D. (Mar. 2021) Decreased case fatality rate of COVID‐19 in the second wave: a study in 53 countries or regions. Transboundary and emerging diseases 68(2):213-5. [crossref]
- Iftimie S, López-Azcona AF, Vallverdú I, Hernández-Flix S, De Febrer G, Parra S, Hernández-Aguilera A, Riu F, Joven J, Andreychuk N, Baiges-Gaya G. (Mar. 2021) First and second waves of coronavirus disease-19: A comparative study in hospitalized patients in Reus, Spain. PloS one 31;16(3):e0248029. [crossref]
- Horby PW, Mafham M, Bell JL, Linsell L, Staplin N, Emberson J, Palfreeman A, Raw J, Elmahi E, Prudon B, Green C. (Oct. 2020) Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. The Lancet 24;396(10259):1345-52. [crossref]
- Costanzo M, De Giglio MA, Roviello GN. (Aug. 2020) SARS-CoV-2: recent reports on antiviral therapies based on lopinavir/ritonavir, darunavir/umifenovir, hydroxychloroquine, remdesivir, favipiravir and other drugs for the treatment of the new coronavirus. Current medicinal chemistry 1;27(27):4536-41.
- Sho Saito MD, Terada M, Shinya Tsuzuki MD. First and second COVID-19 waves in Japan: A comparison of disease severity and characteristics. [crossref]
- Shen KL, Yang YH, Jiang RM, Wang TY, Zhao DC, Jiang Y, Lu XX, Jin RM, Zheng YJ, Xu BP, Xie ZD. (2020) Updated diagnosis, treatment and prevention of COVID-19 in children: experts’ consensus statement (condensed version of the second edition). World Journal of Pediatrics 16(3):232-9. [crossref]
- Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, Tong S. (2020) Epidemiology of COVID-19 among children in China. Pediatrics 1;145(6). [crossref]
- Ellinghaus D, Degenhardt F, Bujanda L, Buti M, Albillos A, Invernizzi P, Fernández J, Prati D, Baselli G, Asselta R, Grimsrud MM. (June 2020) Genomewide association study of severe COVID-19 with respiratory failure. N Engl J Med https://doi. org/10.1056/NEJMoa2020283. [crossref]
- Saeed, U., Uppal, S.R., Piracha, Z.Z. et al. (2021) Evaluation of SARS-CoV-2 antigen-based rapid diagnostic kits in Pakistan: formulation of COVID-19 national testing strategy. Virol J18, https://doi.org/10.1186/s12985-021-01505-3. [crossref]