Abstract
The wrist joint pain and instability are frequently caused by distal radioulnar joint disorders. Most common aetiology is displaced fracture or malunion of distal radius and tears of the triangular fibrocartilage complex with DRUJ instability. A 65-year-old male patient presented to us with complains of pain and deformity of the right wrist of two months duration. Radiographs revealed a malunited distal end radius and a malunited distal ulna fracture. He underwent Sauvé kapandji procedure, in which his distal radius fracture was fixed with locking plate. Follow ups were done at periodic intervals and wrist physiotherapy was instituted. He had acceptable wrist motion at six weeks.
Keywords
Sauvé kapandji, Distal radius, Malunion
Introduction
The wrist joint also referred as the radio carpal joint is a condyloid synovial joint of the distal upper limb that connects and serves as transition point between the forearm and hand and distal radio ulnar articulation is a synovial pivot-type joint between two bones in forearm; the radius and ulna. The wrist joint performs very important functions in day to day life activities of a person, flexion and extension of wrist along with pronation and supination at distal radioulnar joint are fairly important for a person to perform daily activities, injury to wrist joint may result in digital radioulnar joint instability and can lead to deformity and degenerative changes this is often manifested with peanut ulnar side of wrist limited rotation of the forearm with loss of function.
In suave kapandji procedure arthrodesis of the distal radioulnar joint combined with creation of pseudo arthrosis of the digital ulnaArthrodesis of the distal radioulnar joint with creation of distal Nur pseudo arthrosis maintained the owner head in good position provided support for the ulnar corpus and allowed prono supination at the pseudoarthrosis [1]. The suave kapandji procedure is indicated for treatment of conditions that result in DRUJ pain or instability or both and that are refractory to non-surgical treatment, this procedure has been advocated as operation of choice for derangement of distal radial nerve joint in patients with high demand wrists and in particular for post traumatic problems of the distal radioulnar joint it is considered that retaining the head of ulna allows for more normal transmission of force through the rest very few publications have been reported regarding this procedure.
Case Report
A 65-year-old gentleman from a remote village with history of fall sustained injury to right wrist and right hip two months prior to presenting to us, had received conservative management in form of plaster for wrist joint and hip immobilisation, due to ongoing covid pandemic, he did not receive immediate surgical management. He presented with complaints of pain and deformity and restriction motion of the right wrist with pain over right hip and difficulty in standing and walking of two months duration. On clinical examination he had tenderness over distal radioulnar joint with mobility at fracture site and shortened radius with manus valgus deformity reduced the range of motion in all directions.
Radiographs revealed distal end radius communicated fracture with loss of radial height, radial inclination and distal ulna communicated fracture with displaced fragments.
Patient underwent open reduction internal fixation of distal end radius fracture with locking plate and augmentation with k wires to stabilise the fractured styloid fragment and prevent its rotation, comminuted fragments of ulnar remove from separate incision over ulna and distal ulnar head was fixed to radius with the cortico cancel screw this procedure restored the store wrist joint of the patient. a rigid plaster dressing was applied for 6 weeks, after 6 weeks k-wires were removed, and wrist physiotherapy was started at the end of six months he had acceptable range of painless range of motion at wrist with dorsiflexion of 70 degrees palmar flexion of 60 degrees supination 80 degrees pronation 60 degrees and wrist Mayo score of 80 which infers good result.
Discussion
Distal radius fractures (DRF) are very common in orthopaedic practice and are often accompanied by instability of the distal radio ulnar joint (DRUJ) The Sauvé-Kapandji procedure allows fusion at the joint thus decreasing ulnar instability as well as stabilizing the surrounding soft tissue support to the joint. Here the ulnar head is left intact and minimizes the potential for some of the complications that can follow its excision. The most commonly arising complication is the proximal stump instability. The Sauvé-Kapandji procedure is usually useful for treating various pathologic conditions that alter normal function of the DRUJ. The Sauvé-Kapandji procedure is designed to treat pain arising from the distal radio-ulnar joint by fusion, to correct the ulnar variance by recession of the ulnar head and maintain rotation of the forearm by creating a pseudarthrosis. There are strong biomechanical arguments for retaining the ulnar head, especially after trauma and ligamentous weakness of the radiocarpal joint. Conservation of the head maintains the triangular fibrocartilage complex to allow a more physiological transmission of forces from the hand to the forearm. It has been shown that approximately 20% of axial load is passed through the ulnar carpus and even minor derangements in this region can result in changes of load pattern. The ulnar head is also important in the mechanism of action of ECU, which further adds to stability.
Taleisnik [3] suggested that in cases involving subluxation or dislocation of the DRUJ, rupture of the interosseous membrane, which had contributed to static stability, could result in an excessively mobile distal ulna even after surgery. Because chronic derangement in most patients noting discomfort at the proximal ulnar stump was caused by DRUJ dislocation, Kapandji [4] suggested that leaving a short distal ulna fragment, fashioning the ulnar gap as far distally as possible, and creating a pseudarthrosis of approximately 10 mm would decrease the instability of the proximal ulnar stump. To obtain more stability of an excessively mobile proximal ulnar stump, Kapandji’s [4] recommendation should be followed combined with the tenodesis procedure, especially when the cause of DRUJ derangement is dislocation.
Deformities caused by different conditions at the DRUJ which can impair the normal function of the DRUJ can be treated by the Sauvé-Kapandji procedure [5]. A study done by Minami A et al has shown a combination of Sauvé-Kapandji procedure along with extensor carpi ulna tenodesis helps reduce the incidence of instability of the proximal stump [6]. Mohamed et al. [7] mentioned that patient with chronic post-traumatic derangement of DRUJ were treated by a modified Sauvé-Kapandji operation and the post-operative results were acceptable to the patients. Much has been written about problems of the ulnar stump associated with the Sauvé-Kapandji procedure. After the operation, the structures supporting the shaft of the ulna are the interosseous membrane (static), the tendons of ECU and FCU and the pronator quadratus muscle (dynamic). After injury these structures may be damaged, and rupture of the interosseous membrane may lead to a very mobile ulna. Most authors have described problems with pain and clicking of the ulnar stump, but this is usually only a minor inconvenience. Our patient was seldom troubled by symptoms of instability, most only experiencing minor, if any, discomfort. Various modifications have been described to decrease the incidence of this problem and good results have been reported. In our case we performed fixation of distal end radius fracture with locking plate augmented with K wires from styloid and listers tubercle and arthrodesis of distal radioulnar joint with creation of pseudo arthrodesis of digital ulna our patient had good wrist function (Figures 1-4).

Figure 1: Pre-operative radiographic images
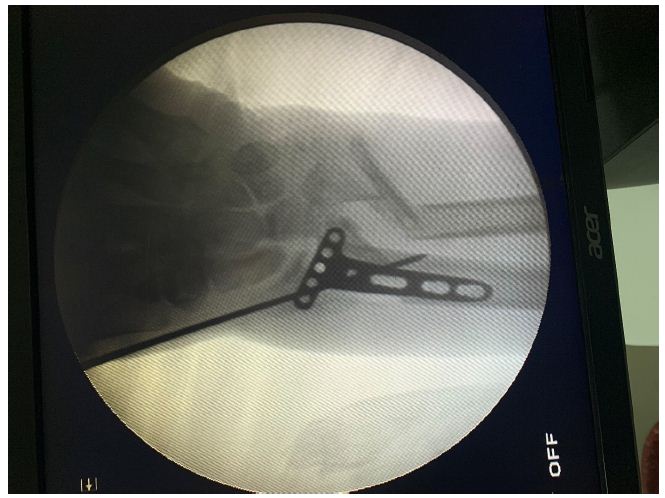
Figure 2: Intra-operative images under c-arm

Figure 3: Post-op images at 1 month interval
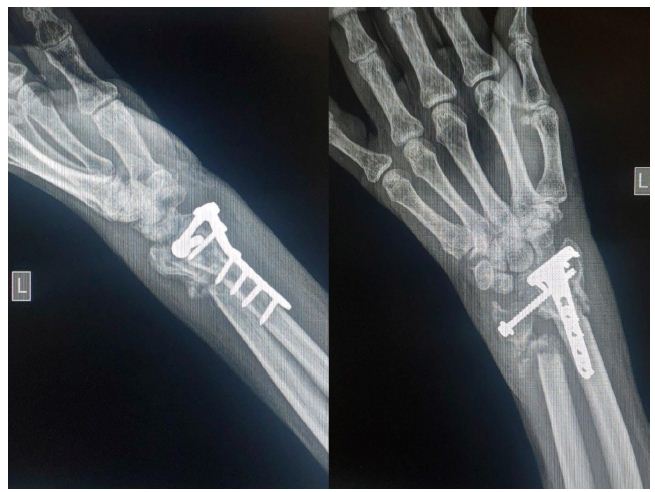
Figure 4: Follow up radiographic images at 6 months
Conclusion
Our case highlights the importance of considering the patient needs and the type of fracture in choosing the management required, a blanket approach can be suitable only when fractures are typical, but such atypical fractures along with advanced age can be successfully managed with wrist joint salvaging procedure, our patient had good outcome with no residual pain.
Conflict of Interest
Nil
Funding
Nil
Ethical approval
Not required
Informed consent
Well informed consent taken after explanation of procedure
References
- Hironobu Inagaki, Ryogo Nakamura, Emiko Horii, Etsuhiro Nakao, Masahiro Tatebe (2006) Symptoms and Radiographic Findings in the Proximal and Distal Ulnar Stumps after the Sauvé-Kapandji Procedure for Treatment of Chronic Derangement of the Distal Radioulnar Joint. The Journal of Hand Surgery. 31: 780-784. [crossref]
- Lamey DM, Fernandez DL (1998) Result of the modified Sauvé-Kapandji procedure in the treatment of chronic posttraumatic derangement of the distal radioulnar joint. J Bone Joint Surg. 80A: 1758-1769. [crossref]
- Taleisnik J (1992) The Sauvé-Kapandji procedure. Clin Orthop. 275: 110-123. [crossref]
- Kapandji IA (1986) Opération de Kapandji-Sauvé. Techniques et indications dans les affections non rhumatismales. Ann Chir Main, 5:181-193.
- Aleisnik J (1992) The Sauve-Kapandji procedure. Clin Orthop Relat Res. 110-1023. [crossref]
- Minami A, Kato H, Iwasaki N (2000) Modification of the Sauvé-Kapandji procedure with extensor carpi ulnaris tenodesis. J Hand Surg Am. 25:1080-1084. [crossref]
- Mohamed MO (2016) Modified Sauve-Kapandji operation for treatment of chronic post-traumatic derangement of the distal radioulnar joint. Anti-Cancer Drugs. [crossref]