Abstract
Introduction: Rapid palatal expansion is utilized in Orthodontics to treat maxillary transverse deficiencies. Such deficiencies can cause functional defects, misalignments, and mandibular shifts that can impact one’s function, comfort, and quality of life. This review aimed to synthesize the clinical findings of rapid palatal expanders.
Methods: A literature search of skeletal effects of maxillary rapid palatal expansion was performed using PubMed and Google Scholar. Inclusion criteria consisted of studies that measured changes in maxillary width over at least one year of expansion and retention or radiographic confirmation of skeletal expansion with a sample size of over 15 subjects. Exclusion criteria were subjects with developmental defects, such as cleft palate, or any type of surgical assisted rapid palatal expansion. A total of 12 articles were found from January 1990 to April 2022 and included in this review.
Results: All 12 articles reported that rapid palatal expansion notably increases the maxillary skeletal transversal dimension. Across all studies, the amount of intercanine expansion from rapid palatal expansion ranged from 2.5 to 4.0 mm, and the amount of intermolar expansion ranged from 3.9 to 6.5 mm. The studies also showed a significant expansion of nasal cavity (airway), various facial sutures being affected, occurrence of buccal tipping of all maxillary teeth, mandibular spacing being gained, and that relapse, although present, had an insignificant effect on the long-term retention of expansion.
Conclusion: Rapid palatal expanders are effective in producing both immediate and long-term transverse expansion in subjects in late mixed dentition.
Keywords
Rapid palatal expansion, Mixed dentition, Orthodontics, Tooth-borne, Maxillary expansion, Midpalatal suture, Computed tomography analysis, Retention, Skeletal changes
Introduction
Rapid palatal expansion (RPE) is utilized in Orthodontic treatment to correct maxillary transverse deficiencies. Patients with maxillary transverse deficiencies may present with functional problems such cross bites, misaligned teeth due to lack of arch coordination, and even mandibular shifts that can develop into future skeletal asymmetry [1]. RPE treatment has long been advocated to solve maxillary constriction. There is a wide variety of maxillary palatal expansion appliances in use today, all with similar effectiveness [2].
The American Association of Orthodontics states that the most critical factor for RPE success is timing and thus routine orthodontic screenings in children are highly recommended to diagnose and treat problems such as cross bites [3]. RPE is most effective in children and young adolescents because their palatal and maxillary sutures are still malleable, as they have not yet completely fused. Transverse expansion of the maxilla is accomplished by banding an expander appliance on the patient’s upper dentition; the appliance has an inbuilt jackscrew that is turned to provide leveraged force that pushes the appliance apart, which then provides force that widens the skeletal base of the palate. Most of the force is applied to split the midpalatal suture; however, the pterygopalatine, inter maxillary, intranasal, maxillonasal, front maxillary, and frontonasal sutures are also affected [4]. Early indicators of maxillary expansion success is evident by the formation of a diastema between the front teeth and an increased intermural width. When these sutures are completely fused, usually by early adulthood, they require more invasive methods of separation such as surgical or manipulate induced separation of the sutures.
It is critical to note that maxillary expansion is one of the most difficult procedures to achieve and maintain, due to the body’s tendency for relapse from disruption of the neuromuscular equilibrium including factors such as (but not limited to): teeth tipping back, incomplete alveolar bone remodelling (necrosis or fenestrations), and periodontal fiber inelasticity. Multiple studies have found that rapid palatal expanders have relapse rates of up to 60% [5,6]. Additionally, because the force is distributed between the maxilla and the teeth, this expansion is a combination of both dental tipping and skeletal expansion, even though purely skeletal expansion is what is desired as the expansion from the dental tipping relapses quickly (within one year) as the teeth upright over time due to equilibrating intraoral pressures [1].
While there are many individual studies that present the results of RPE, the aim of this study is to present a more focused review. Many earlier studies presented the immediate effects of RPE but did not account for the fact that maxillary expansion often partially relapses after treatment, thus overestimating expansion. Studies included in this review had either: 1) skeletal effects of expansion verified through radiographic analysis (such as confirming sutural bone deposition or transverse maxillary bone deposition) or 2) sufficient elapsed time (1 year) for the bone to remodel and teeth to be stable in their new expansive positions. This study also distinguishes between anterior and posterior maxillary expansion and presents intercanine and intermural distance in order to present quantifiable data. The data provided in this study can be useful for clinicians to predict the changes in intercanine and intermural distances to help clinician’s treatment plan more effectively.
Methods
This study consisted of a literature review in which the sources were all obtained from a search through published papers in PubMed and Google Scholar. Search terms included RPE; rapid palatal expansion; retention; radiographic analysis; tooth-borne; maxillary expansion; midpalatal suture; mixed dentition; computed tomography analysis; retention; skeletal changes.
Inclusion and Exclusion Criteria
Inclusion criteria consisted of only English language articles from January 1990 to April 2022 that included sufficient elapsed time (>1 year follow up) or radiographic confirmation of skeletal expansion. Only studies with a sample size greater than 15 subjects were considered.
Exclusion criteria consisted of studies involving patients with developmental defects such as cleft lip or palate or developmental disorders and those with miniscrew-assisted rapid palatal expansion and surgically assisted rapid palatal expansion.
Study Selection
A total of 501 articles were found from Pubmed (n=220) and Google Scholar (n=281). After removing duplicates and screening by inclusion/exclusion criteria, a total of 12 articles met the selection criteria (Figure 1).
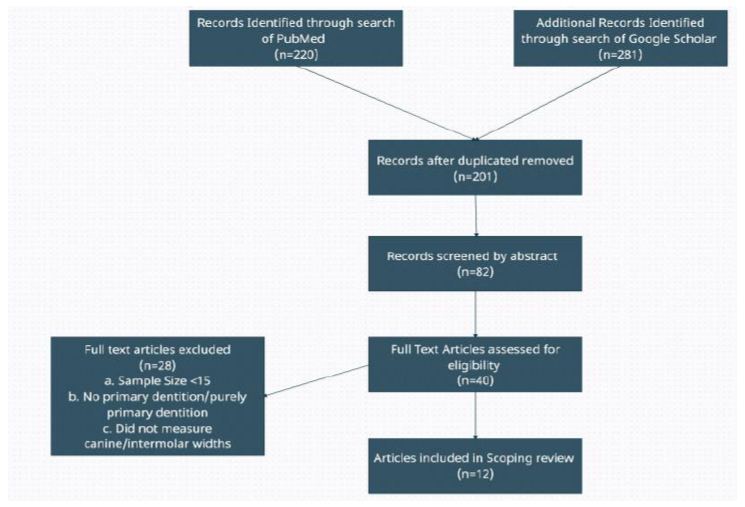
Figure 1: Literature search flow chart
Results
Across all twelve studies, the range of intercanine expansion was 2.5-4.0 mm; the range of intermural expansion was 3.9-6.5 mm (Table 1). The control for intercanine expansion ranged from 0.05 to 3.0 mm, and for intermural expansion, the control ranged from 0.02 to 0.8 mm. When broken down by using radiographic versus cast analysis: Half of the 12 studies analysed RPE radiographically and found intercanine expansion ranged from 2.5 mm to 3.5 mm whereas the controls ranged from 0.25 mm to 0.30 mm expansion. Intermural expansion ranged from 4.5 to 6.0 mm whereas control ranged from 0.02 mm-0.80 mm. The other 6 studies analysing the casts of RPE patients found that RPE intercanine expansion ranged from 2.9 to 4.0 mm whereas the control ranged from 0.05 mm to 0.30 mm. Intermural expansion ranged from 4.4 to 6.1 mm, and control ranged 0.55 mm to 0.61 mm. One meta-analysis analysing 18 studies revealed an overall average gain in intercanine dimension of 2.91 mm and intermural expansion of 4.38 mm. Together, these studies support existing literature that rapid palatal expanders are effective in promoting transverse expansion.
Table 1: Summary of Findings – Changes in Intercanine & Intermolar Widths, Experimental vs. Control
|
(Article Number) Author Last Name |
Average Age, (Sample Size) | Experimental-Intercanine Expansion | Experimental-Intermolar Expansion | Control-Intercanine Width | Control-Intermolar Width |
| (1) Mehtaa [7] |
13.9 ± 1.14 (21) |
N/A | 6.1 | N/A | .02 |
| (2) Kavand [8] |
14.4 ± 1.3 (18) |
N/A |
4.5 | N/A | N/A |
| (3) da Silva [9] |
8.0 (32) |
3.05 ± 1 | 5.05 ± 1.0 | 0.04 | 0.55 |
| (4) Reed [10] | 13.3 (55) | N/A | 5.4 ± 2.1 | N/A | N/A |
| (5) Bazargani [11] | 9.3 (26) | 2.5 | 4.75 ± 1 | 0.25 | 0.80 |
| (6) Celenk-Koka [12] | 13.8 ± 1.4 (20) | N/A | 4.2 ± 1.7 | N/A | N/A |
| (7) McNamara [13] | 12.2 ± 1.3 (112) | 3.9 ± 2.7 | 4.4 ± 1.8 | 0.30 | 0.60 |
| (8) Fenderson [14] | 11.7 ± 1.7 (41) | 3.9 ± 5.8 | 6.1 ± 2.3 | N/A | N/A |
| (9) Geran [15] | 8.8 (51) | 4.0 | 4.3 | 0.21 | 0.70 |
| (10) O’Grady [16] | 9.0 (27) | 4.0 | 3.9 | 0.30 | 0.55 |
| (11) Moussa [17] | 13.7 (165) | 2.5 | 5.5 | 0.05 | 0.60 |
| (12) Adkins [18] | 14.0 (21) | 2.9 ± 1.4 | 6.5 ± 1.2 | N/A | N/A |
Anatomically, the studies found that patients undergoing RPE underwent a significant increase in maxillary width, nasal cavity, and nasopharynx volume as well due to midpalatal suture expansion [1,2,4,8,9,10]. Most of the patient groups demonstrated a triangular-shaped sutural opening that was wider anteriorly, and that the arch development in the maxilla resulted in a complimentary 2.5 mm average space gain in the mandibular arch perimeter as well [1,3,4]. In terms of the dent alveolar changes, the studies found that RPE resulted in slight palatal movement of maxillary incisors, mild buccal crown tipping of all the maxillary dentition, with up righting of the mandibular dentition as a result of the curve of Wilson being levelled over time [2,6,7,9,10].
Discussion
Rapid palatal expanders have been used to increase the maxillary transverse dimension. While there are many individual studies examining the effect of rapid palatal expanders, this literature review presents quantifiable clinical results of expansion verified through stable retention. The existing reviews in the literature focused on RPE’s effects on other anatomical structures or analysed surgically assisted rapid palatal expansion. This review adds to the literature by synthesizing non-surgical RPE clinical finding.
The average age of patients across the studies ranged from 8.0 to 14.4 years old and had either mixed dentition or permanent dentition. Rapid palatal expanders have long been recommended for children and young adolescents before the palatal and maxillary sutures have fused. Because skeletal changes are less significant when matured due to increased rigidity [19], timing of treatment is important. Notably, our results showed that patients in early permanent dentition had more intermural width expansion. Sari et al compared rapid maxillary expansion in mixed dentition (average age 9.2 years) and early permanent dentition (average age 12.7 years) and found that intercanine and intermural widths increased and remained stable in both the mixed dentition and permanent dentition groups [20]. However, subjects in mixed dentition showed a greater tipping of the anchorage teeth and less increases in the ANB angle [20], suggesting that it might be better to delay RPE treatment until early permanent dentition. Another study evaluated the effects of RPE according to cervical vertebrae maturity, with the group treated before the pubertal peak (average age 11 years) showing significantly greater maxillary skeletal and intermural width compared to those treated after (average age 13.6 years) [21]. Based on our review, it appears that treatment with rapid palatal expanders is effective in both mixed and early permanent dentition with an emphasis to treat patients before palatal sutures fuse.
Furthermore, our study evaluated articles that had radiographic evidence of expansion or sufficient elapsed time for remodelling to be stable (>1 year). The results showed a retained increase in intercanine and intermural width. Many studies suggest a significant relapse in maxillary expansion following RPE with one study finding no significant difference in relapse rate between mixed or permanent dentition [22]. Contrarily, other studies have found good stability for intercanine and intermural widths following treatment [17,23], consistent with our findings. However, long-term stability of rapid palatal expansion still seems to be questionable with mixed results across studies. The short-term results are consistent [24], showing significant palatal and/or dental expansion. Nevertheless, orthodontists may experience some long-term relapse in intercanine and intermural expansion everyday practice due to natural neuromuscular equilibrium forces. Orthodontists can utilize the findings of this study to better accurately predict the amount of intercanine and intermural expansion that can be utilized to align the teeth. For this reason, long-term follow-up of children treated with RPE is important.
Limitations
One limitation of this review is that not all articles included control values for intercanine and intermural widths. Except for two studies, each study had uniquely different presentations of their findings. For example, some studies looked into sutural expansion, arch length (in addition to width), tipping of teeth, nasal/oropharyngeal cavity changes, and bone density/deposition to name a few. Additionally, variation in operator technique, RPE design, patient compliance, slight age variations, and physiologic differences are just a few of the factors that add to the complexity of synthesizing various studies.
Conclusion
Rapid palatal expanders are effective in promoting transverse expansion in subjects in late mixed dentition. When timed appropriately, RPE can be utilized to successfully promote maxillary expansion. A future review could focus on a more thorough, dual approach: combining long-term follow-up along with cone beam computed tomography measurements of skeletal expansion. Future review could also compare expansion in pure primary dentition vs early adolescent (mixed) dentition.
References
- Proffit WR, Fields HW, Sarver DM (2007) Contemporary Orthodontics St Louis: Mosby 689-693.
- Agarwal A and Mathur R (2010) Maxillary expansion. Int J Clin Pediatr Dent 3(3):139-146. [crossref]
- Baccetti T, Franchi L, Cameron CG, et al. (2001) Treatment timing for rapid maxillary expansion. Angle Orthod, 71(5), 343-350. [crossref]
- Ghoneima A, Ezzat AF, James H, et al. (2011) Effects of rapid maxillary expansion on the cranial and circummaxillary sutures. Am J Orthod Dentofacial Orthop 140(4): 510-519. [crossref]
- Bishara Samir E and Staley RN (1987) Maxillary expansion: clinical implications. Am J Orthod Dentofacial Orthop, 91(1): 3-14. [crossref]
- Velazquez P, Benito E, and Bravo LA (1996) Rapid maxillary expansion: A study of the long-term effects. Am J Orthod Dentofacial Orthop 109(4): 361-367. [crossref]
- Shivam M, Wanga D, Chia-Ling K, et al. (2021) Long-term effects of mini-screw-assisted rapid palatal expansion on airway: A three-dimensional cone-beam computed tomography study. Angle Orthod 91(2): 195-205. [crossref]
- Golnaz K, Lagravère M, Kula K, et al. (2019) Retrospective CBCT analysis of airway volume changes after bone-borne vs. tooth-borne rapid maxillary expansion. Angle Orthod 89(4): 566-574. [crossref]
- Silva Filho OG, Prado Montes LA, and Torelly LF (1995) Rapid maxillary expansion in the deciduous and mixed dentition evaluated through posteroanterior cephalometric analysis. Am J Orthod Dentofacial Orthop 107(3): 268-275. [crossref]
- Reed N, Ghosh J and Nanda RS (1999) Comparison of treatment outcomes with banded and bonded RPE appliances. Am J Orthod Dentofacial Orthop 116(1): 31-40. [crossref]
- Bazargani F, Feldmann I, Bondemark L (2013) Three-dimensional analysis of effects of rapid maxillary expansion on facial sutures and bones: a systematic review. Angle Orthod 83(6): 1074-1082. [crossref]
- Celenk-Koca T, Erdinc AE, Hazar S, et al. (2018) Evaluation of miniscrew-supported rapid maxillary expansion in adolescents: a prospective randomized clinical trial. Angle Orthod 88 (6): 702-709. [crossref]
- McNamara JA, Baccetti T, Franchi L, et al. (2003) Rapid maxillary expansion followed by fixed appliances: a long-term evaluation of changes in arch dimensions. Angle Orthod 73(4): 344-353. [crossref]
- Fenderson FA, McNamara JA, Baccetti T, et al. (2004) A long-term study on the expansion effects of the cervical-pull facebow with and without rapid maxillary expansion. Angle Orthod 74(4): 439-449. [crossref]
- Geran RG, McNamara JA, Baccetti T, et al. (2006) A prospective long-term study on the effects of rapid maxillary expansion in the early mixed dentition. Am J Orthod Dentofacial Orthop 129(5): 631-640. [crossref]
- O’Grady PW, McNamara JA, Baccetti T, et al. (2006) A long-term evaluation of the mandibular Schwarz appliance and the acrylic splint expander in early mixed dentition patients. Am J Orthod Dentofacial Orthop 130(2): 202-213. [crossref]
- Moussa R, O’Reilly MT and Close JM (1995) Long-term stability of rapid palatal expander treatment and edgewise mechanotherapy. Am J Orthod Dentofacial Orthop 108(5): 478-488. [crossref]
- Adkins MD, Nanda RS, Currier GF (1990) Arch perimeter changes on rapid palatal expansion. Am J Orthod Dentofacial Orthop 97(3): 194-199. [crossref]
- Wertz RA (1970) Skeletal and dental changes accompanying rapid midpalatal suture opening. Am J Orthod 58(1): 41-66. [crossref]
- Sari Z, Uysal T, Usumez S, et al. (2003) Rapid maxillary expansion. Is it better in the mixed or in the permanent dentition? Angle Orthod 73(6): 654-661 [crossref]
- Baccetti T, Franchi L, Cameron CG, et al. (2001) Treatment timing for rapid maxillary expansion. Angle Orthod 71(5): 343-350. [crossref]
- Mohan CN, Araujo EA, Oliver DR, et al. (2016) Long-term stability of rapid palatal expansion in the mixed dentition vs. the permanent dentition. Am J Orthod Dentofacial Orthop 149(6): 856-862. [crossref]
- Mew J (1983) Relapse following maxillary expansion: a study of twenty-five consecutive cases. Am J Orthod 83(1): 56-61. [crossref]
- Ciambotti C, Ngan P, Durkee M, et al. (2001) A comparison of dental and dentoalveolar changes between rapid palatal expansion and nickel-titanium palatal expansion appliances. Am J Orthod Dentofacial Orthop 119(1): 11-20. [crossref]