DOI: 10.31038/CST.2017253
Abstract
Background: Cardiac hemangioendothelioma (CHE) in the adult and cardiac involvement in adult patient with non cardiac-hemangioendothelioma (NC-HE) were rare and uncommon in daily clinical experience.
Methods: We researched in PubMed, Web of Science, Scopus, Cochrane library, and Medline for identifying relevant studies, case series, review and case reports.
Results: We found 33 cases of CHE in the adult and 7 cases of cardiac involvement in NC-HE patients. According to scientific data, the most of CHE patients were female (52%), histological type epithelioid (64%), with main localization in right atrium (41%), and the main clinical diagnosis was incidentally discovered on echocardiogram. The main therapeutic choice was surgical. Otherwise the cardiac metastasis in NC-HE patients (7 cases reported) were most frequent in the hepatic hemangioendothelioma primary localization (57%) than others (spleen, bone, limb, intracranial). The most of patients were female (85.7%) and the main clinical presentation were heart failure (85%).
Conclusion: CHE and cardiac metastasis of NC-HE patients in the adult were rare and unusual neoplasms. The early diagnosis and surgical treatment in each case demonstrated an increase of patients’ survival and quality of life. We explained the scientific data to increase physician knowledge about this rare adulthood vascular neoplasm.
Keywords
Hemangioendothelioma; Primary Cardiac Tumor; Metastatic cardiac tumor; cardiac tumor; cardiac neoplasm; cardiac metastasis.
Introduction
Historical background: Hemangioendothelioma (HE) was described for the first time by Mallori in the 1908 and it was defined as a vascular neoplasms characterized by intermediate features between hemangiomas and angiosarcomas [1, 2]. With the technological evolutions, Stout and colleagues [3] studied firstly in deep the microscopic appearances in the 1943 and explained the likeness of HE to the blood vessels. In the 1967, Fernholz edited one of the first article on “Contribution of History of HE”. Only in the 1988, Enzinger and colleague defined the HE features in intermediate, borderline, or low grade malignancy.
Classification and Clinical presentation: HE was a vascular neoplasm with typical prevalent proliferation of endothelial cells and is was distinguished according to its histological characteristics as [2, 4]:
- papillary intralymphatic,
- retiform hemangioendothelioma,
- kaposiform hemangioendothelioma,
- epithelioid hemangioendothelioma,
- pseudomyogenic hemangioendothelioma
- and composite hemangioendothelioma
HE was characterised by suggestive histological feature as intracytoplasmic vacuoles, nuclear cytoplasmic inclusion, myxoid stroma, hyaline stroma and chondroid stroma (Figures 1 a and b). The most of patient had expression of vascular markers (CD 31, CD 34, ERG, FL1I) and cytokeratins (CAM 5.2, CK7, CK 18) [5].
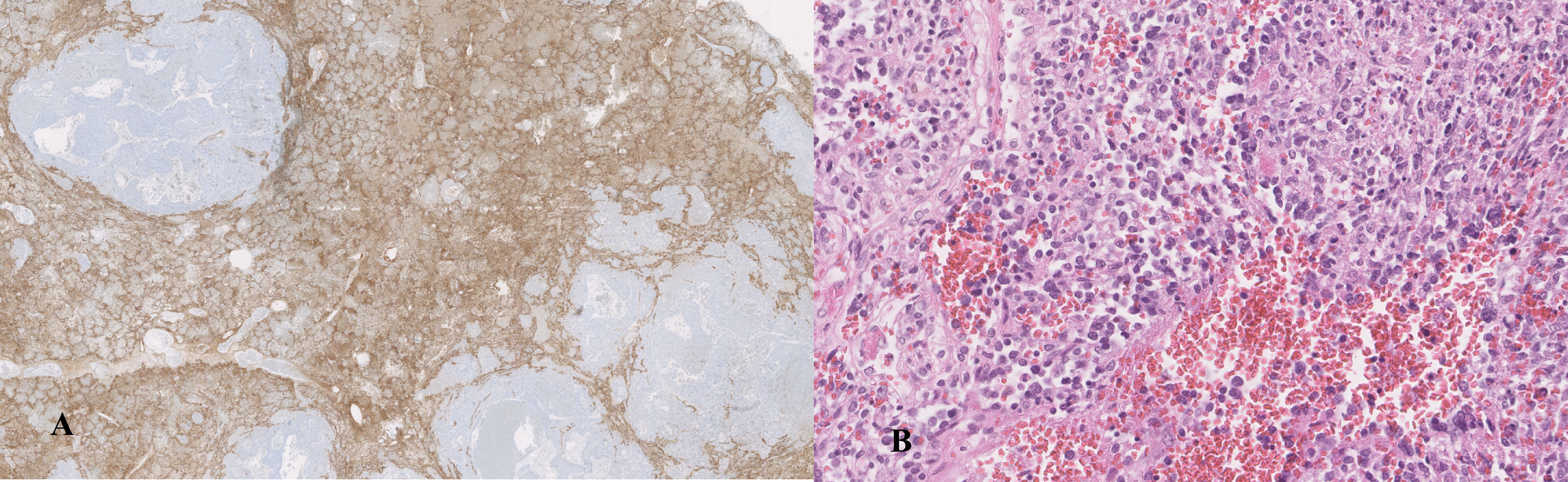
Figure 1. Kaposiform hemangioendothelioma of the right atrium associated to KAsabach- Merritt syndrome: a) image of the vascular neoplasm with epithelial membrane antigen (EMA) antibodies and b) eosin and hematoxylin view.
HE involved mainly liver, lung, skin, soft tissue, bone and spleen and occurring firstly in infancy and early childhood, in the adult it was very uncommon [2].
Each of the histological types of HE had own typical presentations and patterns, such as association with lymphatic vessel proliferation as well as Kasabach-Merritt syndrome (KMS) [6-9]. KMS included thrombocytopenia, microangiopathic hemolytic anemia and mild consumptive coagulopathy, and developed often in KHE, Kaposiform lymphatic anomaly (KLA) and tufted angioma (TA) [7, 8].
HE would have different grades of aggression like:
- finite
- low aggression
- mild aggression
- moderate aggression
- severe aggression, like Kaposiform HE
- Local to the adjoining structures
- Metastatic
Singularly, epithelioid HE was defined in two histological grade according to its aggressiveness: classic (low-grade) and malignant (intermediate-grade) [5-55].
The progression of HE was unpredictable: sometimes it grew slowly and sometimes the tumour was more active and spread quickly [2]. The characteristics of the patients, the different clinical and spreading of HE influenced the therapeutic choices: surgical, medical or palliative.
Finally, also the mortality depended to histological type and grade of aggression and clinical correlations.
Methods
We researched english article on PubMed, Web of Science, Scopus, Cochrane library, and Medline for identifying relevant english studies, reviews, case series and case reports in the adult with the following keywords: 1) cardiac hemangioendothelioma,
2) primary cardiac hemangioendothelioma, 3) cardiac metastasis in hemangioendothelioma, 4) Cardiac Involvement in Hemangioendothelioma in the adult, and 5) Hemangioendothelioma/ Heart/ Adult. We found 272 articles with those criteria (Figure 2) and we selected and chosen 33 case reports and 7 reviews that satisfied our research criteria (Figure 2).
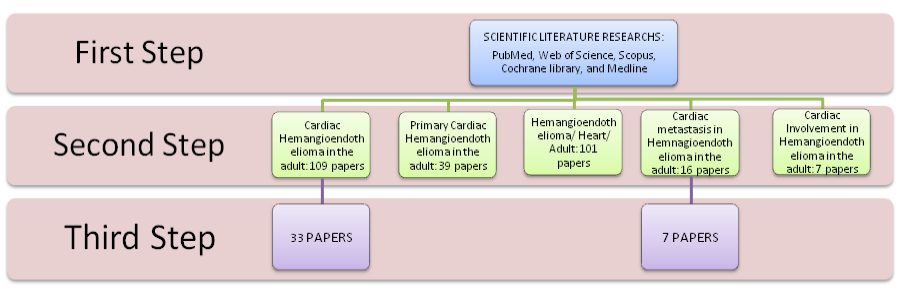
Figure 2. Description of scientific literature review process: first step we had researched all article in the literature
Results
According to our scientific research, the primary cardiac hemangioendothelioma was 33 reported cases. The patient age range was from 19 to 77 year-old, the average age was 45.1 ± 16.5 year-old (Table 1). The most of patients were female (n=17, 52%, Figure 3). The most common primary cardiac localization was right atrium (n=14, 41%) then the cardiac valve (n=5, 15%), left atrium ( n=4, 12%), right ventricle ( n=3, 9%), coronaric sinus (n=2, 6%), superior vena cava/ right atrium (n=2, 6%), right appendage (n=1, 3%), left ventricle (n=1, 3%), and not defined (n=2, 6%) (Figure 4). The histopathological feature of the HE in the case reported was predominantly ephiteloid (n=21, 66%), kaposiform (n=1, 3%) and defined malignant ( n=3, 9%) and not defined (n=8, 24%) (Figure 4). The clinical presentations of these patients were characterised by incidentally discovered on echocardiogram (n=11, 34.4%), dyspnoea (n=2, 6.3%), chest pain (n=4, 12.5%), alveolar hemorrhage (n=1, 3.1%), cardiac tamponade (n=3, 9.4%), incidentally discovered an heart murmur (n=3, 9.4%), arrhythmia (n=1, 3.1%), cerebrovascular event like stroke (n=1, 3.1%), widened superior mediastinum noticed on a routine chest radiograph (n=1, 3.1%), thromboembolism (n=1, 3.1%), and incidentally discovered by autopsy (n=1, 3.1%) (Figures 5 and 6). The most of patients were CD31 and CD34 positive (30.3%) and CD 99 positive (18.1%). The main therapy were the surgery (n=21, 65.6%). In the case of cardiac metastasis of hemangioendothelioma (seven reported cases in literature), the age of patients were 61.7± 12.7 year-old and they were female (85.7%). The first localization of the tumour was indicated in the Table 2. In all the cases, the patient suffered of heart failure and the most of them were undergone to surgery.
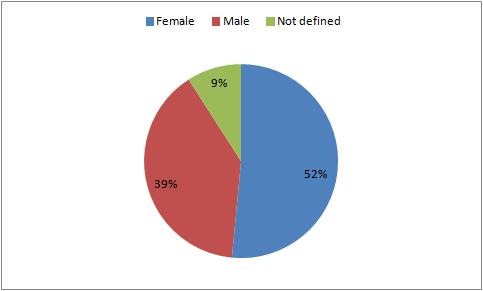
Figure 3. The percentage of cardiac hemangioendothelioma localization in the reported literature cases.
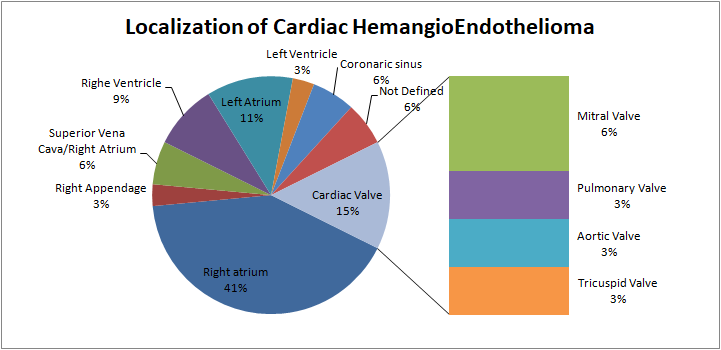
Figure 4. The percentage of cardiac hemangioendothelioma histological type in the reported literature cases.
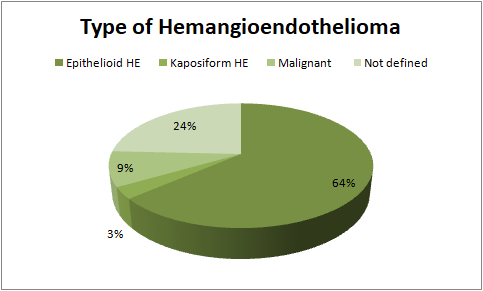
Figure 5. Type of hemangioendothelioma
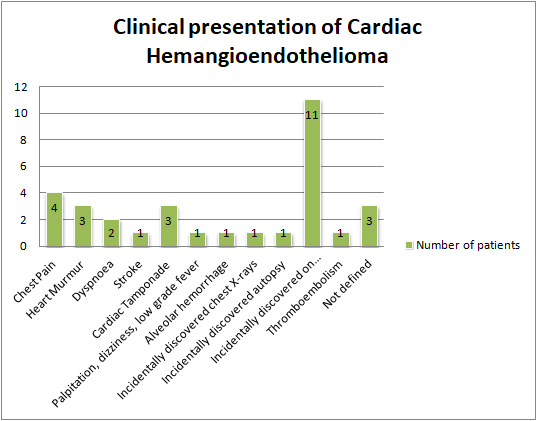
Figure 6. The clinical presentation of cardiac hemangioendothelioma in the reported literature cases were absolutely unpredictable in the adult with a major incidence of chest pain or dyspnea but wide variability in the clinical first manifestation due to patient’s health background, histological type of hemangioendothelioma and grade of aggression.
Discussion
The cardiac hemangioendothelioma was predominantly epithelioid type (66% of the cases), with a peculiar tumour site in right atrium (40% of the cases). The most of these patients were female and they had good outcome (follow up positive after 6 months in the 46.9%). In particularly, the patients undergone to aggressive and rapid surgery, were better outcome than delay diagnosis or late surgical procedure [15-45]. As reported by scientific literature, cardiac malignant tumours were rare and uncommon, especially metastatic cardiac involvement [53, 54]. Cardiac hemangioendothelioma were considered an atypical unexpected malignant cardiac tumours with high local aggressiveness and metastasizing potential [30-32, 34, 36-37].
On the other hand, we had researched the reported articled of cardiac metastasis in patient with non cardiac hemangioendothelioma reported in Table 2 [48-52]. Bisesi and colleagues [14], had already firstly documented the possibility of cardiac involvement in multifocal epithelioid hemangioendothelioma in 1996, hence we had studied in deep the scientific literature to look for other cases like this and to understand the clinical presentation and evolution of the cardiac metastasis of a hemangioendothelioma.
In our research, we had found 6 cases of cardiac metastasis of hemangioendothelioma. All of the cases were in female (100%) with a primary HE in liver (50%), one ovarian HE, one bone HE and the last intracranial HE. The most of them showed heart failure and worsening hemodynamic parameters in association with coagulative disorders and hence end–stage of multi-organ failure. The prognosis of them was unfavourable specially in the presence of coagulative disorders.
Conforming in Table 2 and our review of the literature, cardiac metastasis in patients with non-cardiac hemangioendothelioma were out of ordinary and exceptional but remarkable for the prognosis of the patients [14, 48-52].
Table 1. Cases of cardiac hemangioendothelioma in the adult reported in scientific literature. M: male, F: female, ND: non defined, RA: right atrium, MV: mitral valve, LA: left atrium, RV: right ventricle, LV: left ventricle, PV: pulmonary valve, AV: aortic valve, TV: tricuspid valve, CS: coronaric sinus, SCV: superior vena cava, F-up: follow up.
| Reference | Year | Age | Sex | Site | HE Type | Presentation | Therapy | Follow up | |
| 1 | Blanchard et al15 | 1952 | 29 | M | Right Appendage |
ND | Chest pain | ND | ND |
| 2 | Crenshaw et al16 | 1959 | 36 | F | RA | ND | Chest pain | ND | ND |
| 3 | Allaire et al17 | 1964 | ND | ND | ND | ND | ND | ND | ND |
| 4 | Hayward et al18 | 1979 | 49 | F | MV | Epithelioid | Diastolic murmur typical of mitral stenosis | Surgical | Alive after 4 years |
| 5 | Di Biasi et al20 | 1988 | ND | M | RV | Epithelioid | Incidentally discovered on echocardiogram | Surgical | ND |
| 6 | Singal et al19 | 1987 | 19 | F | LA | Epithelioid | Heart murmur, clubbed finger | Resection | Dead |
| 7 | Gegenbach et al21 | 1991 | ND | ND | LV | Epithelioid | Incidentally discovered on echocardiogram | ND | Alive after 4 months |
| 8 | Montes Orbe et al | 1991 | 56 | F | PV | Epithelioid | Thromboembolism | Surgical and medical |
ND |
| 9 | Marchiano et al22 | 1993 | 71 | F | RA | Epithelioid | Palpitation, dizziness, low grade fever | Surgical resection |
Alive after surgery |
| 10 | Billé-Turc et al23 | 1993 | 59 | M | AV | Epithelioid | Stroke | Surgical | Alive (F-up 1 year) |
| 11 | Di Biasi et al24 | 1995 | 35 | M | RV | Epithelioid | Incidentally discovered on echocardiogram | Surgical | Alive (F-up 1 year) |
| 12 | Ichikawa et al25 | 1997 | 32 | F | CS | Malignant | Incidentally discovered on echocardiogram | Surgical | Alive |
| 13 | Hongquan et al26 | 1998 | 42 | F | RA | ND | Incidentally discovered on echocardiogram | Surgical | Alive |
| 14 | Yoshida et al27 | 1999 | ND | M | RA | Malignant | Cardiac tamponade | Surgical | Dead |
| 15 | Di Biasi et al24 | 1995 | 35 | M | RV | ND | Dyspnoea | ||
| 16 | Kamiyoshihara M28 | 2001 | 32 | M | ND | Malignant | ND | Surgical Excision |
Dead after 41 months |
| 17 | Agaimy et al29 | 2002 | 68 | M | RV/TV | Epithelioid | Incidentally discovered antopsy | ND | Dead |
| 18 | Kitamura et al30 | 2005 | 36 | F | RA | Epithelioid | Cardiac tamponade | Surgical resection |
Alive (F-up 3 years) |
| 19 | Vall Bernal et al31 | 2005 | 69 | F | MV | Epithelioid | Edema, exertional dyspnea | Surgical resection |
Alive (F-up 6 months) |
| 20 | Wang et al32 | 2006 | 36 | F | RA | ND | Dyspnoea | ND | ND |
| 21 | Moulai et al33 | 2006 | 53 | M | CS | Epithelioid | Incidentally discovered on echocardiogram | Heart transplant | Alive (F-up 10 years) |
| 22 | Lisy et al34 | 2006 | 61 | M | LA | Epithelioid | Incidentally discovered on echocardiogram | Surgical resection |
ND |
| 23 | Safirstein et al35 | 2007 | 51 | F | RA | Epithelioid | Incidentally discovered on echocardiogram | Surgical resection |
Alive (F-up 8 years) |
| 24 | Zhang et al36 | 2008 | 66 | F | LA | Epithelioid | Incidentally discovered on echocardiogram | Heart transplantation | Alive |
| 25 | Messias et al37 | 2008 | 21 | F | LA | Epithelioid | Chest pain | Surgical resection |
Alive |
| 26 | Kahlout M et al38 | 2009 | 44 | F | RA | Epithelioid | Cardiac tamponade | ND | ND |
| 27 | Guray et al39 | 2010 | 25 | M | RA | ND | Heart failure | Medical | ND |
| 27 | Lahon et al40 | 2012 | 29 | F | SVC | Epithelioid | widened superior mediastinum noticed on a routine chest radiograph | Surgical resection |
Alive |
| 28 | Sugimoto T et al41 | 2013 | 77 | F | RA | Epithelioid | Incidentally discovered on echocardiogram | ND | ND |
| 29 | Allain et al42 | 2014 | ND | ND | SVC/RA | Epithelioid | ND | ND | ND |
| 30 | Ellouze et al43 | 2015 | 53 | M | RA | Epithelioid | Incidentally discovered on echocardiogram | Surgical resection |
Alive |
| 31 | Gaytán-Cortés et al44 | 2016 | 23 | M | RA | ND | chest pain, intermittent paroxysmal nocturnal dyspnea and malaise | Surgical resection |
Alive |
| 32 | Lappa et al45 (article in press) |
2017 | 36 | F | RA | Kaposiform | Alveolar Hemorrhage | Surgical and drug supports |
Dead |
Table 2. Cases of cardiac metastasis in adult patients with non-cardiac primary hemangioendothelioma, reported in scientific literature. M: male, F: female, ND: non defined, MTs: metastasis; RA: right atrium; HE; hemangioendothelioma; IL: interleuchin; CT: chemotherapy; Pt: patient.
| Principal Reported Case of metastatic cardiac hemangioendothelioma | |||||
| Author | Age Pt | Gender | Primary Tumor | Complications | Therapy |
| Myauchi et al (1987)46 | ND | F | Ovarian Hemangiomatosis | MTS pericardium and RA | Medical |
| Dubois et al (1987)47 | 64 | F | hepato-splenoganglionic hemangioendothelioma | MTs at the heart à heart failure | Surgical and medical |
| Hurley et al (1994)48 | ND | F | Intracranial epithelioid HE | Seizures, Liver and heart multifocal locliation |
Aggressive surgical treatment |
| Bhutto et al (1995)49 | ND | M | hepatic epithelioid hemangioendothelioma | Heart MTs | irradiation, IL-2 injection, and/or surgery |
| Bellmunt et al (1999)50 | 48 | F | hepatic epithelioid hemangioendothelioma | Heart metastasis Portal hypertension |
CT à adriamycin |
| Ilasi et al (1999)51 | ND | F | HE of the bone | Heart failure MTs in RA |
Chemotherapy |
| Hsu CY (2014)52 | 73 | F | hepatic epithelioid hemangioendothelioma | Heart failure | embolization of the abnormal neoangiogenic vessels |
Conclusion
Our literature review would like to be a resume of the cardiac hemangioendothelioma and cardiac involvement in patients with non- cardiac hemangioendothelioma in daily clinical experience. In line with our analysis, the cardiac-HE was vascular aggressive neoplasm with variable histopathological pattern and outcome, principally in female patient and right atrium. Its outcome would be influenced to the early diagnosis and prompt surgical and medical treatments. On the contrary, the cardiac involvement in patients with non-cardiac hemangioendothelioma was weird and life-threatening: only seven cases described and with worsening evolution due to coagulative disorders, heart failure and end-stage multi-organ disease. In case of suspicion of CHE or cardiac involvement of NC-HE were immediately undergone to appropriate diagnostic exams (lab test, echocardiogram, computed tomography, and so on) and rapid surgical and medical therapies in order to avoid the life-threatening evolution of these malignant pathologies.
Acknowledgements: A special thanks go to Dr. Rosalba Grillo and her collaboration in the production of histological images.
Funding: none
Conflicts of interest: All the authors declare non conflict of interest.
References
- Mallory FB (1908) The Results Of The Application Of Special Histological Methods To The Study Of T J Exp Med 10: 575–593. [crossref]
- Requena L, Kutzner H (2013) Semin Diagn Pathol.
- Stout AP (1943) Hemangio-Endothelioma: a Tumor of Blood Vessels Featuring Vascular Endothelial Ann Surg 118: 445–464.
- Fernández Y, Bernabeu-Wittel M, García-Morillo JS, et (2009) Kaposiform hemangioendothelioma. Eur J Intern Med.
- Anderson T, Zhang L, Hameed M, Rusch V, Travis WD, Antonescu CR (2015) Thoracic epithelioid malignant vascular tumors: a clinicopathologic study of 52 cases with emphasis on pathologic grading and molecular studies of WWTR1- CAMTA1 Am J Surg Pathol 39: 132–139.
- Larsen EC, Zinkham WH, Eggleston JC, Zitelli BJ (1987) Kasabach-Merritt syndrome: therapeutic considerations. Pediatrics 79: 971–980. [crossref]
- Maguiness S, Guenther L (2002) Kasabach-Merritt syndrome. J Cutan Med Surg.
- Kelly M (2010) Kasabach-Merritt Pediatr Clin North Am
- Haahr V, Jacobsen E, Bendix K, Nielsen JL, Peterslund NA (1994) [Kasabach–Merritt syndrome]. Ugeskr Laeger 156: 6011–6014. [crossref]
- Messias P, Bernardo J, Antunes MJ (2008) Primary left atrial haemangioendothelioma. Interact Cardiovasc Thorac Surg 7: 945–946. [crossref]
- Safirstein J, Aksenov S, Smith F (2007) Cardiac epithelioid hemangioendothelioma with 8-year follow-up. Cardiovasc Pathol.
- Gaytan-Cortes FC, Arteaga-Adame J, Careaga-Reyna G, Lezama-Urtecho C, Alvarez-Sanchez L (2016) [Primary cardiac hemangioendothelioma: early diagnosis and surgical resection]. Rev Med Inst Mex Seguro
- Toursarkissian B, O’Connor WN, Dillon ML (1990) Mediastinal epithelioid hemangioendothelioma. Ann Thorac Surg.
- Bisesi MA, Broderick LS, Smith JA (1996) MR demonstration of right atrial involvement in multifocal epithelioid AJR Am J Roentgenol 167: 953–954. [crossref]
- BLANCHARD AJ, HETHRINGTON H (1952) Malignant haemangioendothelioma of heart. Can Med Assoc J 66: 147–150. [crossref]
- CRENSHAW JF, DOWLING EA, CRESSWELL WF Jr (1959) Primary hemangio-
endothelioma of the heart. Ann Intern Med 50: 1289–1298. [crossref] - Allaire FJ, Grimm CA, Taylor LM, et (1964) Primary Hemangioendothelioma of the heart. Report of a case treated with irradiation and cyclophosphamide. Rocky Mt Med J 61: 34–37.
- Hayward RH, Korompai FL (1979) “Endothelioma of the Mitral Valve,” The Annals of Thoracic Surgery 28: 87–89.
- Singal KK, Alagaratnam DM, Brundage B, Ferlinz J, Ghou P (1987) Intracardiac mass in a young woman with a history of brain tumor. Chest 92: 337–341. [crossref]
- Di Biasi P, Santoli E, Santoli C (1988) Primary tumors of the right ventricle: apropos of a case of hemangioendothelioma treated surgically. G Ital Cardiol 18: 1025–7
- Gengenbach S, Ridker PM (1991) Left ventricular hemangioma in Kasabach- Merritt syndrome. Am Heart J 121: 202–203. [crossref]
- Marchiano D, Fisher F, Hofstetter S (1993) Epithelioid hemangioendothelioma of the heart with distant metastases. A case report and literature review. J Cardiovasc Surg (Torino) 34: 529–33.
- Bille’-turk F, Padovani R, Rosario R, et (1993) “Hemangio- endothelioma of the Aortic Valve Revealed by Transient Ischemic Episodes,” La Presse Médicale.
- Di Biasi P, Scrofani R, Santoli C (1995) Cardiac Ann Thorac Surg 59: 792–3.
- Ichikawa H, Kaneko T, Obayashi T, et (1997) Surgical treatment of malignant hemangioendothelioma originated from the right atrium: a case report. Kyobo Geka 50: 67–70.
- Hongquan Y, Hua R, Quancai C, Qi M, Xiaocheng L, et (1998) Cardiac hemangioendothelioma. J Cardiovasc Surg (Torino) 39: 655–658. [crossref]
- Yoshida A, Kanda T, Sakamoto H, et (1999) Sudden death with malignant hemangioendothelioma originating in the pericardium–a case report. Angiology 50: 607–11.
- Kamiyoshihara M, Ishikawa S, Morishita Y (2001) Sudden death due to rupture of an omental metastatic tumor arising from cardiac A case report. J Cardiovasc Surg (Torino) 42: 495–7.
- Agaimy A, Kaiser A, Wünsch PH (2002) Epithelioid hemangioendothelioma of the heart in association with myelodysplastic syndrome. Z Kardiol 91: 352–6.
- Kitamura K, Okabayashi H, Hanyu M, et (2005) Successful Enucleation of a Gi- ant Cardiac Hemangioendothelioma Showing an Unusual Proliferation Pattern. The Journal of Thoracic and Cardiovascular Surgery 130: 1199–1201.
- Val-Bernal JF, Gracia-Alberdi E, Gutierrez JA and Garijo MF (2005) Incidental in Vivo of an Epithelioid Heman-gioendothelioma of the Mitral V Pathology Interna-tional 55: 644–648.
- Wang LF, Liu M, Zhu H, Han W, Hu CY, et (2006) Primary cardiac hemangioendothelioma: a case report. Chin Med J (Engl) 119: 966–968. [crossref]
- Moulai N, Chavanon O, Guillou L, Noirclerc M, Blin D, et (2006) “Atypical Primary Epithelioid He- mangioendothelioma of the Heart,” Journal of Thoracic Oncology 2: 188–189.
- Lisy M, Beierlein W, Muller H, Bultmann B and Ziemer G (2007) “Left Atrial Epithelioid Hemangioendothelioma,” The Journal of Thoracic and Cardiovascular Surgery 133: 803–804.
- Safirstein J, Aksenov S, Smith F (2007) Cardiac epithelioid hemangioendothelioma with 8-year follow-up. Cardiovasc Pathol 16: 183–186. [crossref]
- Zhang PJ, Brooks JS, Goldblum JR, Yoder B, et (2008) Primary cardiac sarcomas: a clinicopathologic analysis of a series with follow-up information in 17 patients and emphasis on long-term survival. Hum Pathol 39: 1385–95.
- Messias P, Bernardo J, Antunes MJ (2008) Primary left atrial haemangioendothelioma. Interact Cardiovasc Thorac Surg 7: 945–946. [crossref]
- M Kahlout, A Al-Mulla, A Chaikhouni, et al. (2009) Unusual presentation of a rare tumor: Cardiac epithelioid hemangioepithelioma presenting as cardiac Heart Views 10: 132–5.
- Güray Y, Demirkan B, Güray U, BoyaciA(2010) Right atrial hemangioendothelioma: a three-dimensional echocardiographic Anadolu Kardiyol Derg 10: E7–8.
- Lahon B, Fabre D, De Montpreville V and Dartevelle P (2010) Epithelioid haemangioendothelioma of the superior vena Interact Cardiovasc Thorac Surg 15: 186–7.
- Sugimoto T, Yamamoto K and S (2013) Yoshi A Primary Epithelioid Hemangioendothelioma of the Right Atrium: Report of a Case and Literature Review. Open Journal of Thoracic Surgery 3: 63–67.
- Allain G, Hajj-Chahine J, Lacroix C, et (2014) Surgical management of an epithelioid hemangioendothelioma of the superior vena cava protruding into the right atrium. J Card Surg 29: 779–81.
- Ellouze M, Dami M, Beaulieu Y, et (2015) Resection of a right atrial epithelioid hemangioendothelioma. Cardiovasc Pathol 24: 401–4.
- Gaytán-Cortés FC, Arteaga-Adame J, Careaga-Reyna G, et (2016) Primary cardiac hemangioendothelioma: early diagnosis and surgical resection. Rev Med Inst Mex Seguro Soc 54: 392–6.
- Angela Lappa, Marzia Cottini, Silvia Donfrancesco, et (2017) Primary cardiac kaposiform hemangioendothelioma: the rare adult-onset. Review of the literature. EC Anesthesia.
- Miyauchi J, Mukai M, Yamazaki K, Kiso I, Higashi S, Hori S (1987) Bilateral ovarian hemangiomas associated with diffuse hemangioendotheliomatosis: a case Acta Pathol Jpn 37: 1347–55.
- Dubois A, Eledjam JJ, Deixonne B, et (1987) Lymph node-hepatosplenic hemangioma in an adult with consumption coagulopathy and fatal cardiac insufficiency. Ann Gastroenterol Hepatol (Paris) 23: 363–6.
- Hurley TR, Whisler WW, Clasen RA, Smith MC, Bleck TP, et (1994) Recurrent intracranial epithelioid hemangioendothelioma associated with multicentric disease of liver and heart: case report. Neurosurgery 35: 148–51.
- Bhutto AM, Uehara K, Takamiyagi A, Hagiwara K, Nonaka S (1995) Cutaneous malignant hemangioendothelioma: clinical and histopathological observations of nine patients and a review of the J Dermatol 22: 253–61.
- Bellmunt J, Allende E, Navarro M, Morales S, Sans M, et (1989) Epithelioid hemangioendothelioma of the liver with myocardial metastases. Jpn J Clin Oncol 19: 153–158. [crossref]
- Ilasi JA, Smilari TF, Kolitz J, Zanzi I, Hajdu SI (1999) Malignant hemangioendothelioma presenting as multifocal intraskeletal lesions during pregnancy. A case J Reprod Med 44: 49–52.
- Hsu CY, Liu YC, Li CP, Huang PH, Lin CH, Chao Y (2014) Malignant hepatic epithelioid hemangioendothelioma with high-output heart failure: successful management of heart failure with transcatheter arterial Asia Pac J Clin Oncol 10: e118–21.
- Salcedo EE, Cohen GI, White RD, Davison MB (1992) Cardiac tumors: diagnosis and management. Curr Probl Cardiol 17: 73–137. [crossref]
- Travis WD, Brambilla E, Mu¨ller-Hermelink (2004) World Health Organisation classification of Pathology and genetics of tumours of the lung, pleura, thymus and heart. Lyon, France: IARC Press.
- Deyrup AT, Tighiouart M, Montag AG, Weiss SW (2008) Epithelioid hemangioendothelioma of soft tissue: a proposal for risk stratification based on 49 Am J Surg Pathol 32: 924–927.