Abstract
Objectives: Successful endodontic treatment requires complete information about morphology of root canals of the tooth. The object of our research was to assess the prevalence of third root in permanent mandibular first molars between Iraqi people.
Methods: Two hundred fifty-seven patients (161 females and 96 males) were included in this study. Those patients required endodontic treatment for permanent mandibular first molar. Examination of teeth was done during a period of one and a half year. Digital radiograph was used to investigate the occurrence of radix entomolaris. Comparison of the percentage of third root between males and females were established. Data were statistically analyzed with chi-square test.
Results: Statistical evaluation was carried out for the presence of third root among males and females using chi-square test with SPSS version 20. In this test P > 0.05 (non-significant), P ≤ 0.05 (significant). Total incidence of radix entomolaris was five teeth (5/257) the percentage was 1.9 %. Statistical analysis revealed a non-significant difference in the incidence of third root between females (2/161) and males (3/96).
Conclusion: Endodontists should have thorough information about anatomical variations of the root and root canals of mandibular first molar during endodontic treatment. Correct examination clinically and radiographically is essential to discover the presence of any morphological variations of the root canal system.
Keywords
Digital radiograph, Distolingual root, Endodontic treatment, Radix entomolaris, Maxillary first molar
Introduction
Scientific knowledge of the morphology of the tooth roots and their canals plays an important role during endodontic treatment. This will ensure complete debridement of all infected pulp with complete instrumentation and obturation [1]. A periapical lesion may be result from failed endodontic treatment if any one of these steps are inadequately done [2]. Generally, permanent mandibular first molars have two roots: one root mesially and one root distally. Two root canals present in the mesial root (mesiobuccal and mesiolingual). One canal present in the root distally, sometime distal root may comprise a second canal. The presence of the further distolingual root in the mandibular first molar is considered the main variant of this tooth, named radix entomolaris (RE) and its occurrence is infrequent. There are numerous anatomical surveys established a racial origin for the occurrence of third distolingual root in the permanent mandibular first molar. It presents with an incidence of 5 to more than 30% in populations with Mongoloid traits, such as Chinese, Eskimos, and American-Indians [3,4], A maximum rate of 3% in African population [5,6], while its prevalence in Europeans was less. Cinically, it is of great importance to provide sufficient information about morphological variation of any tooth that can affect the success rate of the root canal therapy. Our research was aimed to determine the prevalence of third root distolingually in the permanent mandibular first molar in Iraqi people.
Materials and Methods
Two hundred fifty-seven patients with an average age of 20-45 years old (161 females and 96 males) were included in this study. Those patients attained private dental clinic for endodontic treatment. Two Preoperative radiographs were done for each patient with a digital X-ray sensor (Visiodent RVG Dental Sensor, France). Sign of the presence of third root is translucent lines defining the pulp space and the periodontal ligaments located in the superior part of the distal root. Firstly, anaesthetic solution was injected to patient. Rubber dam was applied for tooth isolation. Then prepared the access cavity. Pulp extirpation was accomplished. Apex locator (Woodpex III Golden Apex Locater, Zhengzhou Linker Medical Equipment Co., Ltd. China) was used to determine working length. Radiograph using digital X-ray sensor was taken to establish working length. The next step is the instrumentation of all canals by using a rotary endodontic system (protaper Gold, Dentsply, Maillefer, Switzerland), then obturation was done by using single cone with bioceramic sealer. After finishing, a radiograph was obtained in order to evaluate the efficiency of the obturation (Figures 1-3).
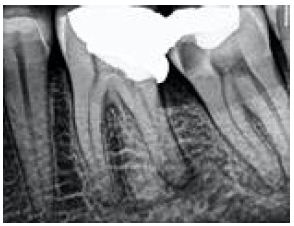
Figure 1: Preoperative radiograph

Figure 2: Cone fit checking

Figure 3: Obturation with bioceramic sealer
Results
Statistical evaluation was carried out for the presence of third root among males and females using chi-square test with SPSS version 20. In this test P > 0.05 (Non-significant), P ≤ 0.05 (Significant) Two hundred fifty-seven patients (161 females and 96 males) were included in this study. Total incidence of radix entomolaris was five teeth (5/257) the percentage is 1.9 %. Statistical analysis revealed a non-significant difference (P > 0.05) in the incidence of third root between females (2/161) and males (3/96) as shown in Table 1.
Table 1: Percentage of radix entomolaris in the tested patients

Discussion
The first Permanent teeth erupted is the Mandibular first molar. This tooth highly involved with tooth decay and commonly need to root canal treatment. Missed canals with the subsequent incomplete instrumentation of all infected pulp tissues are one of the most common reasons of unsuccessful endodontic treatment. Full familiarity with morphological variations of root plays an important role in increasing the chance of the successful root canal treatment. In the cases of incomplete treatment for all root canals such as the third root distolingually this will result in failure of the endodontic treatment. Radix entomolaris has been classified into the following types: Type I means straight root or canal. Type II means the beginning of the entry is curved and then continued as a straight root/root canal. Type III means the beginning of the entry is curved in the coronal third of the root canal with the presence of another curve started in the middle and continuing to the apical third [7]. Requirement of successful endodontic treatment is the preoperative radiograph with a correct examination of the tooth clinically [8]. Thorough information about the presence of additional root or root canals can be obtained by taking a radiograph with various angles [7]. The clinician can suspect the presence of additional third root when he noticed changing of the tooth form coronally, like a highly clear distolingual lobe with a convex cervical outline [9]. Many studies stated that taking two radiographs with mesial or distal shifting cone (30 degrees) very helpful for investigating occurrence of the of radix entomolaris [10]. Rectangular or trapezoidal outline access cavity preparation should be performed when the additional third root is established or suspected radiographically. The location of the orifice of radix entomolaris is disto to mesiolingually from the main distal canal. If the access to third root not clearly seen after the roof of the pulp chamber is removed, this need to complete detection of wall and floor of the pulp chamber, mainly distolingually by using sharp endodontic explorer [9]. In the current study, the total percentage of third root incidence in mandibular first molars was 1.9%, the result in accordance with other investigations that were accomplished on Middle East people [10,11]. In comparison with data of another studies collected for Asian origin our result is lower, they reported the incidence of additional root as follows: in Koreans 4.5% [12], in Chinese 32% [13], and in Taiwanese 25.6% [14]. Our result showed a non significant difference in the occurrence of radix entomolaris between males and females. Other studies showed similar results [15-18]. Previous in vivo study was accomplished by Mukhaimer and Azizi whom study the incidence of radix entomolaris in Palestinian people when they attained a dental center for endodontic treatment, the total percentage of third root incidence in mandibular first molars was 3.73%, which considered within the range of other researches done for the Middle East population, although it was significantly lesser than the range obtained for population of far east [19]. Whenever the additional root suspected to presence during endodontic treatment of permanent mandibular first molar, modification of the access cavity preparation should be performed in order to ensure complete cleaning and obturation of all root canals, Otherwise the presence of missed canal can result in failure of the treatment.
Conclusion and Recommendation
Endodontists should have thorough information about anatomical variations of the root and root canals of mandibular first molar during endodontic treatment. Correct examination clinically and radiographically is essential to discover the presence of any morphological variations of root canal system. Preoperative radiographs with certain angulation are a vital issue in this matter. Modification of access cavity is necessary to locate all root canal orifices to certify complete debridement and obturation.
Conflict of Interest
The authors declare that they have no conflicts of interest.
Source of Funding
This research did not receive any specific grant from funding agencies in the public.
Ethical Approval
This research was performed in accordance with Helsinki Declaration and approved by the Ethical Approval Committee at university of Anbar.
Date: 21/6/2021
No.83
Author Contribution
All authors have participated sufficiently in this work in order to have a public responsibility for its contents, including conception and design, or analysis and interpretation of the data, conscripting the article or revising it critically for important intellectual content; and final approval of the article. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
NAH Concept and design of the study, research conduction, OHA collection and organization of data, analyzing and interpretation of data, HAS writing the initial and final draft of the manuscript, and all authors have critically reviewed and approved the final draft and are agreed for their responsibility for the contents and similarity index of the manuscript.
References
- Sjogren U, Agglund BH, Sundqvis Gt, Wing K (1990) Factors affecting the long-term results of endodontic treatment, J Endod 16: 498-504. [crossref]
- Siqueira JF (2001) Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J 34: 1-10. [crossref]
- Turner II CG (1971) Three-rooted mandibular first permanent molars and the question of American Indian origins. Amer J Phy Anth 34: 229-241. [crossref]
- Curzon ME, Curzon JA (1971) Three-rooted mandibular molars in the Keewatin Eskimo. J Can Den Ass 37: 71-72. [crossref]
- Sperber GH, Moreau J L (1998) Study of the number of roots and canals in Senegalese first permanent mandibular molars. Int Endod J 31: 117-122. [crossref]
- Ahmed HA, Abu-Bakr NH, Yahia NA, Ibrahim YE (2007) Root and canal morphology of permanent mandibular molars in a Sudanese population. Int Endod J 40: 766-771. [crossref]
- De Moor RJG, Deroose CA, Calberson FLG (2004) The radix entomolaris in mandibular first molars: an endodontic challenge. Int Endod J 37: 789-799. [crossref]
- Carlsen O, Alexandersen V (1999) Radix paramolaris and radix distomolaris in Danish permanent maxillary molars. Acta Odont Scan 57: 283-289. [crossref]
- Calberson FL, De Moor RJ, Deroose CA (2007) The radix entomolaris and paramolaris: clinical approach in endodontics. J Endod 33: 58-63
- Naoum HJ, Love RM, Chandler NP, Herbison P (2003) Effect of X-ray beam angulation and intraradicular contrast medium on radiographic interpretation of lower first molar root canal anatomy. Int Endod J 36: 12-19. [crossref]
- Al-Nazhan S (1999) Incidence of four canals in root-canal-treated mandibular first molars in a Saudi Arabian subpopulation. Int Endod J 32: 49-52. [crossref]
- Al-Qudah AA, Awawdeh LA (2009) Root and canal morphology of mandibular first and second molar teeth in a jordanian population. Int Endod J 42: 775-784. [crossref]
- Song JS, Choi HJ, Jung IY, Jung HS, Kim SO (2010) The prevalence and morphologic classification of distolingual roots in the mandibular molars in a korean population. J Endod 36: 653-657. [crossref]
- Gu Y, Lu Q, Wang H, Ding Y, Wang P, Ni L (2010) Root canal morphology of permanent three-rooted mandibular first molars—part I: pulp floor and root canal system. J Endod 2010; 36: 990-994. [crossref]
- Tu MG, Tsai CC, Jou MJ et al. (2007) Prevalence of three-rooted mandibular first molars among Taiwanese individuals. J Endod 2007;33: 1163-1166. [crossref]
- Schafer E, Breuer D, Janzen S (2009) The prevalence of three-¨ rooted mandibular permanent first molars in a German population. J Endod 35: 202-205. [crossref]
- Garg AK, Tewari RK, Kumar A, Hashmi SH, Agrawal N, et al. (2010) Prevalence of three-rooted mandibular permanent first molars among the indian population. J Endod 36: 1302-1306. [crossref]
- Olak HC, Ozcan E, Hamidi MM (2012) Prevalence of three-¨ rooted mandibular permanent first molars among the Turkish population. Nig J Clin Prac 15: 306-310. [crossref]
- Mukhaimer R, Azizi Z (2014) Incidence of radix entomolaris in mandibular first molars in Palestinian population: a clinical investigation. Int Schol Res Not. [crossref]