Abstract
Introduction: It is unclear, how many of the isolated fractures of the greater trochanter who have further extension into the intertrochanteric area.
Method: Data have been retrospectively pulled from patients between October 1999 and September 2019 CAT scans and MRI scans were made with an isolated fracture of the greater trochanter on a plain radiograph, in the emergency department at Aarhus University Hospital, Denmark – to further analyse the extent of the fracture into the intertrochanteric region, if one was present.
Result: 59 patients were included. 25.4% of the fractures did not have further extension into the intertrochanteric region and 74.6%, had to some degree extension into the intertrochanteric region.
Discussion: The majority of seemingly isolated fractures of the greater trochanter have a non-displaced extension into the intertrochanteric region. MRI seems to be CAT-scanning superior in determining in-bone involvement. Further prospective studies with blinded randomization and larger cohorts are required to further power the strengths of the findings.
Keywords
Isolated trochanteric hip fracture, Intertrochanteric involvement, MRI vs. C, Extension of fracture not visual
Introduction
Hip fractures incidents increases exponentially with age, and with approximately 3,000/100,000 hip fractures per year in women older than 85 years, hip fractures are a common fracture in orthopaedic patients [1]. Correct and early diagnosis is important in lowering mortality, as these fractures are often seen in elderly and fragile patients [2,3]. Trauma mechanism and patient symptoms dictates further diagnostics and plain radiograph is often considered first choice in the line of determining treatment. If a fracture of the hip is visualized, treatment would often rely on surgical intervention, within a short time frame.
Isolated fracture of the Greater Trochanter (GT) is relatively uncommon. One study found that among 455 hip fractures only 2% were isolated fractures of the GT [4], thus demanding further diagnostic imaging other than radiographs, as proven by multiple studies [5-10], to determine whether the Intertrochanteric (IT) space is involved. IT-involvement does not clearly and explicit show on plain radiographs, however, when it does, it should be classified as an IT fracture.
Literature shows that, when further diagnostic imaging is needed Magnetic Resonance Imaging (MRI) is preferred as this imaging modality has a high sensitivity examining soft tissue like bone marrow. Fractures are identified when a large area of poorly defined bone oedema is present in a linear lesion in a T1-weighted image. Contrary to the normal hyperdense area of the bone, a fracture would show as a dark hypodense area [11].
It is unclear how many isolated trochanteric fractures defined on radiographs that really represents IT-fractures. Therefore, the aim of this paper is to quantify the frequency of IT-involvement of seemingly isolated GT fractures, and to what extend the IT space is affected.
Methods
Between October 1999 and September 2019 patients presenting with a confirmed isolated fracture of the GT in plain radiographs and who received further diagnostic imaging by either MRI or Computed Axial Tomography (CAT)-scans in the emergency department at Aarhus University Hospital were collected by one surgeon on site. Retrospectively, data where controlled for radiographs, CAT and MRI scans and obtained using the online imaging system, IMPAX (Agfa Healthcare, Mortsel, Belgium). Patients were excluded from the study if scans were not obtainable. Demographical data were obtained through IMPAX as well.
All CAT and MRI scans were assessed by all authors (JN, RT and DW) to determine the extent of the fracture into the IT space. Consensus was reached in all cases. The fracture extension of the IT space was determined as either ‘No involvement’, ‘One third of the IT space’, ‘Two thirds of the IT space’, ‘Borderline intertrochanteric fracture’ or ‘IT”, see Figure 1. Furthermore, the distribution of the involvement was determined from fractioning the frequency of the fracture type in the group by the sample size (n/N) times 100.
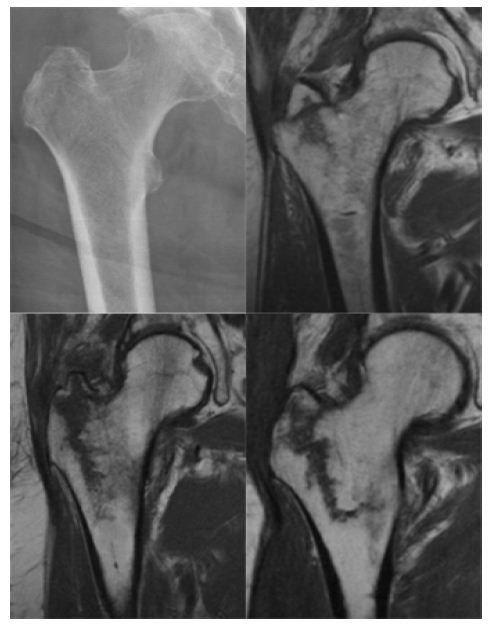
Figure 1: Illustrates how the graduation of intertrochanteric involvement was evaluated.
Top left: A radiograph of an isolated fracture of the great throchanter.
Top right: Isolated fracture of the great throchanter with 1/3 of the interthrocanteric space involved.
Bottom left: Isolated fracture of the great throchanter with 2/3 of the interthrocanteric space involved.
Bottom right: Bordering intertrochanteric fracture.
Results
59 patients were included in this study. Of these 19 were men and 40 women with a mean age of 68 (range 46 – 98). One patient was excluded due to the patient having a prosthesis in the femur, and further two were excluded due to a collum femoris fracture. 46 patients underwent only MRI-scans after the concluding x-ray, 12 patients had only CAT-scans done, and two patients had both CAT-scans and an MRI.
CAT and MRI where assessed, and the distribution and extension of IT-involvement were measured (Table 1). Table 1 shows 25.4% of the fractures did not have further extension into the IT-region. Half of the descriptions were based on only CAT-scans as the additional diagnostic imaging, the other half was MRI confirmed. 74.6% of isolated fractures of the GT, had extension into the IT-region, one patient had a definite IT fracture only discovered through MRI.
Table 1: Distribution of intertrochanteric involvement in isolated fractures of the greater trochanter.
|
It Involvement |
No Involvement | 1/3 | 2/3 | Bordering Intertrochanteric Fracture |
Intertrochanteric Fracture |
|
No. |
15 | 16 | 18 | 9 |
1 |
|
% of |
25.4 | 27.1 | 30.5 | 15.3 |
1.7 |
In the two cases, where both MRI and CAT were utilized, it was discovered that the CAT scan was not able to rediscover the IT involvement, being linear bone edema that was visualized on the MRI scan. Hereby wrongly concluding no IT involvement in the first place.
Discussion
This paper found that more than 74% of seemingly isolated fractures of the greater trochanter on plain radiographs have in addition a coexisting non-displaced involvement of the IT region towards the medial cortex of the femur, near the area of the lesser trochanter. As other studies [5-7,10,12,13] concluded, this in general counts for the majority of isolated fractures of the greater trochanter.
In two cases CAT-scans seemed to be MRI-scans inferior, when extension proven by MRI, could not be rediscovered on CAT-scans. This may undermine the general use of CAT-scans when determining in-bone involvement in fractures. All fractures found on CAT-scans were also identified on MRI-scans.
Specific guidelines for the treatment of isolated GT-fractures have yet to be defined. Studies suggest that the involvement of the IT space plays a role in determining what treatment the patient should be offered. Park et al., [7] suggest that if the extension is only located within the lateral one third, conservative treatment with immediate weight-bearing would suffice. Furthermore, they advise that in cases of extension through the medial one third of the femur or cortex, the fracture would be unstable, and should undergo immediate surgical intervention. Nevertheless, international consensus on this topic is yet to be reached.
The treatment strategy for this kind of fracture remains inconclusive, due to the rarity of the fracture. However, studies examining this issue found that cases with IT involvement extending up to two thirds of the IT area, conservative treatment with immediate weight-bearing, and the assistance of a walker aid, showed no fall-outs in boney-union or fibrous union in the healing of the fracture in all 43 patients [7,12,13]. However, further medial involvement would destabilize the fracture, making immediate weight bearing, or non-surgical intervention, a hazard for the patient.
This paper carries a high external validity. While the fracture itself is uncommon, the patient group of elderly patients and the trauma mechanism with low-energy impact fall to the hip is one of the most common emergency room incidents. The image-diagnostic findings and their attainableness are simple in interpretation and are already common hold in most hospitals.
Looking at seemingly isolated fractures of the GT, a definitive IT fracture, or secondary displacement, from the available literature, is rare, and conservative treatment with immediate weight-bearing seems to be safe and effective in the bony union of the fracture. However, further imaging should always be considered, considering that the majority of seemingly isolated fractures of the greater trochanter have to a variable extent involvement of the IT area – and further visualization of the fracture line, is imminent in determining further treatment, because surgical intervention with stabilization of the fracture, should be considered in bordering IT fractures. Otherwise, early weight-bearing could cause an unstable fracture to progress into a complete IT fracture.
Limitations to this paper include having no follow-up in patient outcome, to further affirm immediate weight-bearing as the first choice of treatment in fractures of the GT with IT extension. Inclusion of patients is done by one surgeon and thereby not exhaustive for the period. This paper is retrospective in composition and would not be able to randomize patients to either surgical intervention or conservative treatment in a randomized controlled trial. In addition, a larger scale of patients would be required to higher the power of the hypothesis.
Conclusion
This paper observed, that 74.6% of seemingly isolated fractures of the GT has a non-displaced extension of the fracture line into the IT region. This extension is best visualized via MRI, deeming CAT-scanning inferior when determining in-bone involvement. Furthermore, some extensions can be well handled conservatively – however if surgery is required, visualization of the IT space should only be done via MRI.
References
- Dhanwal DK, Dennison EM, Harveyb NC, Cooper C (2011) Epidemiology of hip fracture: Worldwide geographic variation. Indian J Orthop 45: 15-22 [crossref]
- Bredahl C, Nyholm B, Hindsholm KB, Mortensen JS, Olesen AS (1992) Mortality after hip fracture: Results of operation within 12 h of admission. Injury 23: 83-86. [crossref]
- Fernandez MA, Griffin XL, Costa ML (2015) Management of hip fracture. Br Med Bull 115: 165-172.
- Moon NH, Shin WC, Do MK, Woo SH, Son SM, et al. (2018) Diagnostic strategy for elderly patients with isolated greater trochanter fractures on plain radiographs. BMC Musculoskelet Disord 19: 256. [crossref]
- Craig JG, Moed BR, Eyler WR, van Holsbeeck M (2000) Fractures of the greater trochanter: Intertrochanteric extension shown by MR imaging. Skeletal Radiol 29: 572-576. [crossref]
- Feldman F, Staron RB (2004) MRI of Seemingly isolated greater trochanteric fractures. American Journal of Roentgenology 183: 323-329. [crossref]
- Park JH, Shon HC, Chang KS, Kim Ch, Byun SE, et al. (2018) How can MRI change the treatment strategy in apparently isolated greater trochanteric fracture? Injury 49: 824-828. [crossref]
- Omura T, Takahashi M, Koide Y, Inoue T (2000) Evaluation of isolated fractures of the greater trochanter with magnetic resonance imaging. Arch Orthop Trauma Surg 120: 195-197. [crossref]
- Lee KH, Kim HM, Kim YS, Jeong C, Moon CW, et al. (2010) Isolated fractures of the greater trochanter with occult intertrochanteric extension. Arch Orthop Trauma Surg 130: 1275-1280.
- Chung PH, Kang S, Kim JP, Kim YS, Lee HM, et al. (2016) Occult intertrochanteric fracture mimicking the fracture of greater trochanter. Hip Pelvis 28: 112-119. [crossref]
- Speer KP, Spritzer CE, Bassett FH, Feagin JA, Garrett, WE (1992) Osseous injury associated with acute tears of the anterior cruciate ligament. Am J Sports Med 20: 382-389. [crossref]
- LaLonde B, Fenton P, Campbell A, Wilson P, Yen D (2010) Immediate weight-bearing in suspected isolated greater trochanter fractures as delineated on MRI. Iowa Orthop J 30: 201-204. [crossref]
- Kent WT. Whitchurch, Siow M, Chun L, Bardesi J, et al. (2020) Greater trochanteric fractures with lntertrochanteric extension identified on MRI: What is the rate of displacement when treated nonoperatively? Injury.