Abstract
Background: DDH constitutes a group of conditions involving hip sublaxation and dislocation. It is mandatory for management of these cases to be followed by aftercare with Braces. Some complications may develop during follow-up in hip spica or hip brace.
Introduction: DDH encompasses a spectrum of diseases that includes dysplasia (a shallow or underdeveloped acetabulum), subluxation, and dislocation. These conditions are commonly seen with arthrogryposis, myelomeningocele, and Larsen’s syndrome. Cases of developmental dislocation of the hip (DDH) still occur after walking age because of Late or missed diagnosis and failed conservative treatment. Lack of follow-up leads to a lot of complications.
Case presentation: 4years old female child admitted to our hospital complaining of limbing and had neglected history of right DDH. She w managed by derotation femoral osteotomy and hip spica cast with smooth follow-up recovery. At 12 weeks an abduction hip brace was advised but follow-up last for few weeks. When returned back and during routine x-ray inferior dislocation was noticed. Patient planned for surgery and hip Spica cast. Follow-up passed smoothly for 12 months then the Spica cast replaced by Abduction hip brace. The reduction was confirmed by good x-ray.
Discussion: Bracing is an important step in follow-up treatment program of DDH. Loss of reduction as a complication may occur during follow-up regimen. Inferior hip dislocation in the hip abduction brace is a rare complication and rarely mentioned in the literatures. Avoidance of this complication can be achieved by having good orthotics in the hospital and applying the brace under supervision of the orthopedic surgeon. Immediate x-ray to check for good position of the head, and closed monitoring of the patient to detect any changes in the hip position.
Conclusion: Inferior hip subluxation in the hip brace rarely occurs as a complication during follow-up program of DDH treatment. Early recognition of this complication and reduction of the flexion angle led to a stable dislocation of the hip.
Keywords
Developmental hip dislocation, Dysplasia, Hip spica, Hip brace
Introduction
Developmental hip dysplasia (DDH) encompasses a spectrum of conditions that include dysplasia (a flat or underdeveloped acetabulum), subluxation, or dislocation. There is also a teratologic hip that is dislocated in utero and irreducible on neonatal examination. It has a pseudo-acetabulum, and is associated with neuromuscular and genetic disorders. These disorders are common in arthrogryposis, myelomeningocele, and Larsen syndrome. Cases of developmental hip dislocation (DDH) continue to occur even after walking age owing to late diagnosis or failure of conservative treatment [1]. Conservative or surgical treatment for DDH needs aftercare for braces. Lack of aftercare leads to a lot of complications related to Spica Casting – hip abduction braces (Figure 1). These complications involve compression of femoral nerve due to hyperflexion, inferior dislocation, skin detachment and the most important one is avascular necrosis of femoral head. Care of the cast or the brace should bear attention to the fully reducible hip, child not attempting to stand, close regular follow-up (every 1-2 weeks) by imaging and adjustments of the brace when necessary by the surgeon[2-3]. Pavlik Harness Failure may occur due to: Improper application and follow-up by the physician, inadequate initial reduction, failure to recognize persistent dislocation and poor parent compliance. The risk factors predispose to Pavilk harness failures include: bilateral hip dislocation, age greater than seven weeks prior to initiation of treatment with the harness and lack of Ortolani sign at initial examination.
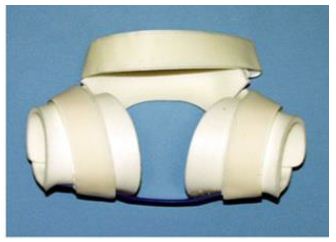
Figure 1: Spica Casting – hip abduction braces
Case Presentation
Four years female child presented to the orthopedic department of El-Hussein University Hospital with painless limping, limb shortening and radiographs showed a neglected right DDH. The patient was scheduled for surgery (femoral shortening with derotation osteotomy) and hip spica. Recovery was smooth and follow-up care was good. At 12 months the hip Spica was removed and the patient was advised to have an abduction hip brace. She went to a place outside the hospital and the technician applied the brace. The patient did not come back to the hospital to continue the follow-up program. After 6 weeks the child’s parents returned back to our hospital to make sure of the condition. Unfortunly plain x-ray showed strange inferior dislocation of hip (Figure 2a and 2b) and CT confirmed the diagnosis Figure 3.
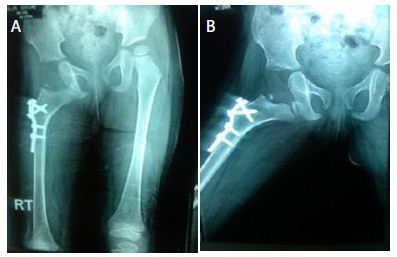
Figure 2: X-ray showing strange inferior dislocation of hip

Figure 3: CT diagnosis
Plan of Management
The patient was scheduled for operative intervention. Closed reduction was an attempt first but failed as there was a band of elasticity feeling preventing relocation of the hip. We decided to go to open intervention.
Operative Details
We used the same incision. The operative findings revealed the femoral head was buttonholed in the capsule that preventing reduction. The capsule was release and the head was relocated easily to the acetabulum. The position was checked by C-arm and hip Spica applied for 4 weeks. The abduction hip splint was applied by the orthopedic surgeon and an immediate X-ray was done and confirmed the good reduction (Figure 4). The postoperative course was uneventful, with no early or late infection being observed. The results were evaluated according to modified McKay criteria, Severin radiological criteria, and Bucholtz – Ogden system of AVN grading after a mean follow-up for 6 months. In the last follow-up, the Clinical Evaluation patient reported no significant hip pain, and radiologically no signs of dislocation or AVN (Figure 5).

Figure 4: X-ray of abduction hip splint

Figure 5: Radiologically no signs of dislocation or AVN
Discussion
Bracing is considered a gold standard in treating Developmental Dysplasia of the Hip (DDH) in infants less than 6 months of age with reducible hips. A variety of braces are available that work on similar principles of limiting hip adduction and extension. The brace eliminates dislocating forces from the hamstrings, the block to reduction of the psoas and improves the muscle line of pull to stabilize the hip joint [4]. The use of excessive force or exceeding the safe zone to maintain hip position can lead to complications, such as femoral nerve palsy and avascular necrosis (AVN) [5-6]. Inferior dislocation (obturator dislocation) from the abduction brace rarely mentioned in literature. Rombouts and Kaelin [3] mention two cases of inferior dislocation but in a neonate due to the Pavlik harness. Also, they reviewed the literatures and mentioned Five cases of inferior (obturator) dislocation complicating the treatment of developmental dislocation of the hip that had been reported previously [7-10]. Only one of these cases was in a neonate [10]. Pediatric orthopedic surgeons have been aware of the problem but no one has studied it fully to declare why it happens and there were no studies to follow up and report on the final results for children with this complication. Ramsey et al. [11] emphasized that adequate hip flexion must be obtainable so that the femoral head is directed towards the triradiate cartilage. Excessive hip flexion, however, directs the metaphysis of femur to come below the triradiate cartilage and may produce an inferior (obturator) dislocation. This complication is classified as grade IIIb according to the Clavien-Dindo classification [12] (Intervention under general anesthesia). To avoid this complication we need to have good orthotics in the hospital, application of the brace should be under the supervision of the orthopedic surgeon, immediate x-ray to check for good position of the head, and closed monitoring of the patient to detect any changes in the hip. In our case and after open reduction; a hip spica cast was applied and followed for 4 weeks. After that an abduction brace was applied carefully by the surgeon and under C-arm image control to verify the proper location of the hip. The brace was gradually weaned over a period of several months [13].
Conclusion
Abduction brace can cause inferior hip dislocation during treatment of DDH. Gentle manipulation may be tried and if failed go for open reduction. Closed monitoring of the brace is mandatory. Early recognition of the complication and diminution of the angle of flexion gave a stable relocation of the hip joint.
Abbreviations
DDH: Developmental Dysplasia of Hip; AVN: Avascular Necrosis
References
- Gulati V, Eseonu K, Sayani J, Ismail N, Uzoigwe C, et al. (2013) Developmental dysplasia of the hip in the newborn: A systematic review. World J Orthop 4: 32-41. [crossref]
- Viere RG, Birch JG, Herring JA, Roach JW, Johnston CE (1990) Use of the Pavlik harness in congenital dislocation of the hip. An analysis of failures of treatment. J Bone Joint Surg Am 72: 238-244. [crossref]
- Rombouts JJ, Kaelin A (1992) Inferior (obturator) dislocation of the hip in neonates. A complication of treatment by Pavlik harness. J Bone Joint Surg Br 74: 708-710. [crossref]
- Merchant R, Singh A, Dala-Ali B (2021) Principles of Bracing in early management of Developmental Dysplasia of Hip.Indian Journal of Orthopaedics 55: 1417-1427. [crossref]
- Tiruveedhula M, Reading I, Clarke N (2015) Failed Pavlik harness treatment for DDH as a risk factor for avascular necrosis. Journal of Pediatric Orthopedics 35: 140-143. [crossref]
- Pool RD, Foster BK, Paterson DC (1986)Avascular necrosis in congenital hip dislocation. The significance of splintage. J Bone Joint Surg Br 68: 427-430. [crossref]
- Lloyd-Roberts GC, Swann M (1966)Pitfalls in the management of congenital dislocation of the hip.J Bone Joint Surg Br 48: 666-681. [crossref]
- Mubarak S, Steven G, Raymond V, Bert McKinnon, David Sutherland D (1981) Pitfalls in the Use of the Pavlik Harness for Treatment of Congenital Dysplasia, Subluxation, and Dislocation of the Hip. J Bone Joint Surg 63: 1239-1248. [crossref]
- Mendez AA, Keret D, MacEwen GD (1990) Obturator dislocation as a complication of closed reduction of the congenitally dislocated hip: a report of two cases.J Pediatr Orthop 10: 265-269. [crossref]
- Langkamer V, Clarke G, Witherow P (1991) Complications of splintage in congenital dislocation of the hip. Archives of Disease in Childhood 66: 1322-1325.
- Ramsey PL, Lasser S, MacEwen GD (1976) Congenital dislocation of the hip. Use of the Pavlik harness in the child during the first six months of life. J Bone Joint Surg 58: 1000-1004. [crossref]
- Dindo D, Demartines N, Clavien PA (2004)Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey.Ann Surg 240: 205-213.
- Emara K, Kersh MA, Hayyawi FA (2019) Duration of immobilization after developmental dysplasia of the hip and open reduction surgery. Int Orthop 43: 405-409. [crossref]