Abstract
Objective: The purpose of this study was to evaluate the immediate effects of task-oriented training on walking and balancing in-patient clients with chronic stroke.
Design: A randomized trial with pre-training and post-training evaluations.
Subjects: Ten participants were randomly assigned to an experimental group (N=6) or a control group (N=4).
Methods: The GAITRite (GAITRITE)? The system was used to assess the spatial and temporal walking parameters and the “Timed Up & Go” Test (TUG) was used to assess functional mobility. The Berg Balance Scale (BBS) was used to assess balance. Both groups received a single session of exercise training. Patients in the experimental group received task-oriented training that involved task-specific activities and functional tasks. Patients in the control group received conventional physical therapy training focused on facilitation and normalization of movement.
Results: Analysis of the data indicates that the experimental group performed significantly better than the control group with respect to walking speed (p<0.001) and stride length (p<0.001). Following intervention, the task-oriented training group exhibited a statistically significant (p<0.04) decrease in TUG scores compared with the control group. There was no significant difference in BBS scores between the two groups after intervention.
Conclusions: Task-oriented training can improve walking and functional mobility in patients with stroke. The findings of this study provide preliminary evidence supporting the short-term benefits of task-oriented training for patients with chronic stroke.
Keywords
Stroke, Hemiplegia, Exercise, Rehabilitation
Introduction
It is estimated that each year about 1.2 million people experience a new or recurrent stroke in Europe and 700,000 in the United States [1,2], making it by far the most common cause of long-term disability [3,4]. About one-third of stroke survivors are functionally dependent at one year post stroke and are unable to walk without assistance; and of those who are independent ambulators, 60% of them experience limitations in community ambulation [5,6].
Walking and balance disorders have been reported to be common impairments in people with stroke [5,7,8], and are frequently the common cause of long-term disability and handicap, which contributes to overall increased risk of falls [7]. Improving walking and balance has been the primary goal in the rehabilitation of patients with stroke [4]. Many of the traditional neurofacilitation approaches have been designed to target walking and balance, with many of these approaches focused on managing impairments [9]. Since improvements in impairments may not be generalized to function, the effectiveness of these approaches in improving walking and balance is limited [9].
Current evidence suggests that rehabilitation training is most effective when the related task is specific to the intended outcome [9], and the training allows patients to perform activities in real-time situations [10]. Numerous recent studies have demonstrated that task-oriented training is a critical rehabilitation strategy to improve the functional status of individuals with stroke [11-16]. A published systematic review [17] analyzed 151 trials on the effects of physical therapy on functional outcomes in patients with stroke and found that there is strong evidence that patients with stroke benefit from task-oriented training intervention in which functional asks are directly trained [17].
Relatively, very few studies have explored the effects of task-oriented training on walking and balance in individuals with chronic stroke. A Cochrane review conducted by Pollack et al. [18] reported that there is a need for high quality randomized trials to determine the efficacy of task-oriented training. Although improvements in walking and balance in people with stroke have been reported as the results of participation in a task-oriented program over a period of time, evidence regarding the immediate effect of a task-oriented training on walking and balance has not been reported in the literature. Therefore, the purpose of this study was to examine the immediate effects of task-oriented training on walking and balance in people with chronic strokes.
Methods
Study Design
A randomized controlled trial with pre-training and post-training evaluations was used. All participants completed the pre-training evaluation and then were randomly assigned to the experimental (n=6) or control (n=4) group. The randomization process was carried out by a person independent of the study. The investigator who collected the data is a physical therapist who is a Neurology Certified Clinical Specialist with 12 years of clinical experience working with patients with neurological disorders.
Participants
The participants included ten community-dwelling individuals with a first-time stroke who were recruited from outpatient physical therapy clinic in a university setting. The volunteer convenience sample was selected based on the following criteria: (1) a stroke experienced more than 6 months prior to study enrollment; (2) age between 35 and 80 years; (3) able to walk 10 meters independently with or without walking aids or orthotics; and (4) able to follow verbal commands. Exclusion criteria included: (1) debilitating illness before or during the study; (2) surgical procedure up to six months prior to the study; (3) inability to follow commands; or (4) a medical condition that precluded exercising. All subjects were blinded to their group assignment. All the assessment and intervention procedures were carried in the same treatment area. After having been informed about the study procedures, each participant signed an informed consent before enrolling in the study. The study was reviewed and approved by the Institutional Review Board of …………BLINDED…………………. University.
Examination
Subjects were evaluated twice, immediately before (pre-test) and immediately after (post-test) the intervention. The outcome measures included a self-paced walk over the GAITRite system, the “Timed Up & Go” Test (TUG), and the Berg Balance Scale (BBS).
GAITRite System
Temporal and spatial parameters of walking were measured using the GAITRite system (CIR Systems, Havertown, PA). The GAITRite system is a computerized system developed to measure and record temporal and spatial walking parameters. The GAITRite system uses an electronic walkway approximately four meters long with grids of embedded pressure sensors that detect footfalls as the subject walks the length of the walkway. It is a valid and reliable clinical measure for spatial and temporal walking parameters [19]. Each subject was instructed and then asked to practice one walking trial before the actual data were collected. Each subject was instructed to walk over the walkway at a comfortable walking speed. Subjects started walking at a point one meter in front of the walkway and stopped at a point one meter behind the walkway to eliminate the effects of acceleration and deceleration. Subjects who were using walking aids were allowed to use their preferred walking aid. Temporal and spatial parameters of walking including walking speed and stride length were recorded.
The “Timed Up & Go” Test
The TUG is a performance-based test designed to assess functional mobility. The TUG test is a useful tool to monitor the progress of mobility function in ambulant patients with chronic stroke. This test demonstrated good (ICC=.99) and interrater (ICC=.99) reliability as well as validity for people after stroke [20]. The examiner first demonstrated how to perform the TUG test and then instructed the participant to rise from a standard armchair, walk to a line on the floor three meters away, cross the line, turn, walk back to the chair, and sit down again while being timed with a stopwatch. Each participant was allowed to practice one trial before the actual data were collected. Participants performed the test at their own pace, and those who were using walking aids were allowed to use their preferred walking aid.
Berg Balance Test
The BBS was identified as one of the most commonly used assessment tools to measure balance function across the continuum of stroke rehabilitation [20,21]. The BBS is a task-oriented performance-based test that has been used to assess balance function in people after stroke and evaluate response to treatment. The scale consists of 14 functional tasks frequently performed in everyday life. The BBS has strong psychometric properties and has been shown to be a valid test with excellent interrater (ICCs=0.95-0.99) and intrarater reliability (ICC=0.97) for people with stroke [20,21].
Intervention
Both groups received a single session (60 minutes in length) of physical therapy intervention designed to improve walking and balance. Subjects in the control group received conventional intervention focusing on improving walking and balance through facilitation and normalization of movement patterns. Subjects in the experimental group practiced task-oriented activities that focused on walking and balance. The task-oriented training included overground walking, standing up, sit to stand, rising from a chair then walking a short distance, performing step-ups/step-downs, stepping forward, backwards and sideways, walking through an obstacle course, walking while carrying an object, walking at maximal speed, walking backwards and sideways, tandem stance, single leg stance, and functional weight shifting exercises. In all cases, activities were set up on an individual basis and were adapted to the individual’s performance and ability. Assistance or manual guidance was provided, if required, and participants received feedback as needed. Participants were allowed to use their assistive devices as needed. Throughout the therapy session, the therapist emphasized the importance of speed, the number of repetitions was modified according to the participants’ ability. During the testing time, participants were allowed to rest as needed.
Data Analysis
Frequency distributions as well as means and standard deviations were used for descriptive purposes. At the baseline, differences in age and time since the onset of stroke between the two groups were analyzed with an independent 2-sample t-test. Differences in gender and side of hemiplegia were compared between intervention groups using chi-square. The 2-way repeated measure analysis of variance (ANOVA) for repeated measures on the time factor was used to compare the difference between groups (experimental and control) and timing (preintervention, postintervention) for each studied outcome. The alpha level of statistical significance was set at p<0.05. The SPSS statistical software package was used for the analysis.
Results
Ten subjects participated in this study. Participant demographic information, group assignment, side of stroke, and time since strokes are shown in Table 1. There were no statistically significant differences between groups at baseline with respect to demographic, characteristics, or outcome measures. Table 2 shows the group means, and standard deviations of the pre and post scores for time and distance walking parameters, the TUG scores, and the Berg Balance Scale scores. Analysis of the data indicates that the experimental group performed significantly better than the control group with respect to walking speed (p<0.001), and stride length (p<0.001) (Figure 1). Following the intervention, the task-oriented training group exhibited statistically significant (p<0.04) decrease in TUG scores compared with the control group (Figure 2). There was no significant difference in BBS between the two groups after intervention.
Table 1: Subject demographics, characteristics and group assignments
|
Subject |
Group |
Age (year) |
Gender |
Side of Hemiplegia |
Time Since Stroke (month) |
| 1 | Experimental |
72 |
Male | Right |
22 |
| 2 | Experimental |
49 |
Male | Left |
6 |
| 3 | Experimental |
55 |
Female | Left |
9 |
| 4 | Experimental |
68 |
Male | Right |
15 |
| 5 | Experimental |
62 |
Female | Left |
18 |
| 6 | Experimental |
71 |
Male | Right |
17 |
| 7 | Control |
65 |
Male | Right |
11 |
| 8 | Control |
53 |
Female | Left |
14 |
| 9 | Control |
69 |
Female | Right |
13 |
| 10 | Control |
79 |
Male | Left |
25 |
Table 2: Pre-test, post-test, and change scores, means, standard deviations, and mean changes by group
|
Variable |
Score |
Change scores |
|||||
|
Experimental |
Control |
Experimental |
Control |
P-value |
|||
|
Pre |
Post |
Pre |
Post |
Post-pre |
Post-pre |
||
| Walking speed (m/s) |
0.43 ± 0.14 |
0.55 ± 0.14 |
0.49 ± 0.16 |
0.55 ± 0.15 |
±0.12 |
±0.06 |
< 0.001 |
| Stride length (m) |
0.59 ± 0.15 |
0.70 ± 0.14 |
0.61 ± .15 |
0.62 ± 0.15 |
±0.11 |
±0.01 |
< 0.001 |
| TUG (s) |
60.8 ± 10.6 |
55.67 ± 10.83 |
58.7 ± 14.0 |
56.25 ± 13.70 |
-5.53 |
-2.45 |
0.04 |
| BBS |
32.5 ± 4.85 |
35.5 ± 6.06 |
34.5 ± 5.32 |
35.75 ± 5.38 |
±3 |
±1.25 |
0.17 |
TUG: Timed “Up & Go” test; BBS: Berg Balance Scale
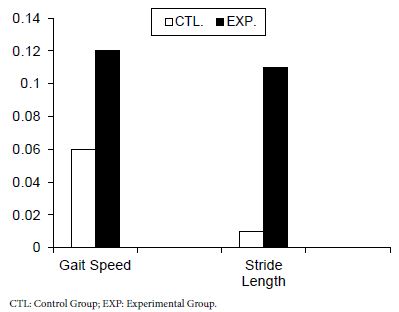
Figure 1: Mean changes for walking speed and stride length for both groups
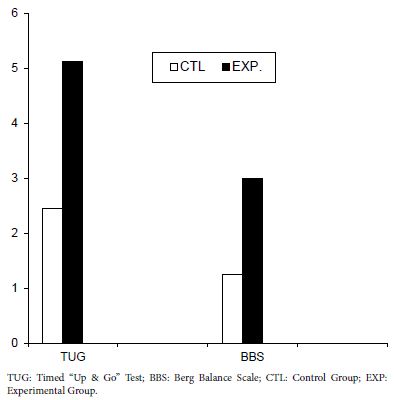
Figure 2: Mean changes for the Timed “Up & Go” test and the Berg Balance Scale for both groups
Discussion
There is a growing body of evidence that supports task-oriented training as a beneficial intervention for patients with stroke. The purpose of this study was to examine the immediate effects of task-oriented training on walking and balance in subjects with chronic strokes. The findings of this study demonstrate that task-oriented training is associated with improvements in walking and balance in people with chronic stroke.
Spatial and temporal walking variables were significantly improved with task-oriented training. The results of the present study are in agreement with the findings of Knox et al. Salbach et al. and Dean et al. [11,15,16], who reported significant improvements in walking speed of individuals with stroke who participated in task-oriented training relative to participants in the control groups. Knox et al. [11] showed improvements in participants following participation in task-oriented circuit gait training as compared to the control group. Salbach et al. [15] showed that 6 weeks of task-oriented training induced an increase in walking speed as compared to the control group. Dean et al. [16] evaluated the effects of task-oriented training, including circuit training, on a small sample of individuals with chronic stroke and found a significant effect on walking speed after 4-week of task-oriented training.
Following the intervention, the task-oriented training group required less time to perform the TUG. Improvement in the TUG scores was statistically significant between the experimental and control groups. This result came in agreement with the finding of Knox et al. Leroux et al,. and Malik et al. [11,14,22] who examined the effect of an 8-week exercise program aimed at improving balance and mobility through various functional tasks in 10 subjects with chronic stroke. Knox et al. [11] reported improvements in TUG score in the experimental group who participated in task-oriented circuit gait training. Malik et al. [22] reported improvements in four weeks of task-oriented training. TUG scores following participation in Leroux et al. [14] concluded that task-oriented exercise program significantly improved the TUG scores in subjects with stroke. In contrast to the improvement in the TUG scores in the present study, Chan et al. Salbach et al. and Dean et al. [13,15,16] reported that task-oriented training did not have statistically significant improvement in the TUG scores. In the Dean et al. study [16], the results reflect a ceiling effect for this measurement tool for two subjects from the experimental group (N=5), these two subjects were able to obtain scores comparable with healthy subjects; in contrast, one subject from the control group (N=4) improved by 10 seconds and this may account for lack of significance in the TUG scores in the Dean et al. study [16]. Several factors may account for the improvements in the TUG scores in the task-oriented training group. Perhaps the most important aspect of task-oriented training is the specificity of training, the task-oriented training in the present study involved rising from a chair and walking this activity which was similar to testing conditions during training was specifically targeting the TUG scores, and may account for the improvement seen in this variable. In addition, previous studies [21,23] showed that there is high correlation between the TUG scores and walking speed in patients with chronic stroke. This high correlation is not surprising since TUG test incorporates walking speed. Given the association between walking speed and the TUG, improvements in walking speed were partially responsible for the improvement seen in the TUG scores in the experimental group.
Although changes in the BBS scores were not statistically significant between the study groups, there were trends toward greater gains in the balance scores in the experimental group compared with the control group. This result is similar to the findings of Salbach et al. study [15] who found no significant effects of task-oriented training on BBS. This is in contrast with the results of Knox et al. Chan et al. and Leroux et al. [11,13,14] who reported significant improvement in the balance following task-oriented training. The differences in the amount of practice and stages of recovery between the present study and Chan et al. and Leroux et al. [13,14] studies may be responsible for the lack of significance in the BBS reported in the present study. However, given the small number of subjects, lack of statistical significance between groups in regard to the BBS scores may be due to a lack of statistical power rather than a lack of effect.
Evidence has shown that task-oriented training is an effective intervention strategy to promote meaningful improvement in motor function [14,18,24] The effect of intervention involving task-oriented training is highly specific and the effectiveness of the training is related to the training parameters used with the maximum training occurs when training activities are similar to real-life tasks [18,22,25]. The intervention activities used in this study were specific and included walking and balance activities. The intervention activities used in the task-oriented group allowed the participants to practice functional tasks used in everyday activities, in real-time situation taking into consideration normal biomechanics, strength, balance, and lower limb function. The improvements in walking and balance may be related to the specificity of training used in this study.
In interpreting the results of this study, several limitations must be considered. The sample size was small in the current study. The results of this study are preliminary for this small sample size, limiting external validity. There was potential for bias since the researcher was not masked to the group assignments. In the present study we did not consider a single-session of task-oriented training to be a major study weakness, because the purpose of the present study was to determine the immediate effects of the task-oriented training, rather than the additive effects of multiple sessions.
The findings of this study demonstrated that task-oriented walking and balance intervention improved walking function in people after stroke. The application of task-specific activities may promote improvements in spatial and temporal walking parameters and functional mobility. The results of the present study suggest that people with chronic stroke may benefit from a task-oriented training program. Further research with a larger sample size is warranted to see if the results of the current study can be replicated. Further study is needed to document the efficacy of a task-oriented home program in people after stroke. Further research is necessary to document the effect of multi-sessions and different schedules of task-oriented training on walking and balance functions. The results of the present study concern the immediate effects of task-oriented training, research should be performed to examine the long-term effects after a training period on recovery of walking and balance functions after stroke.
Conclusions
The findings of this study provide preliminary evidence supporting the short-term benefits of task-oriented training for patients with chronic stroke. Although the generalization of the results of this study is limited due to the small sample size, this study provided preliminary data for a larger controlled trial to examine the effects of task-oriented training in people after stroke. The intervention activities in this study included repetitive practice of functional activities used in everyday activities and did not involve the use of any specific exercise equipment; these activities can be easily incorporated into a home exercise program. The results of the present study indicate that patients with chronic stroke would benefit from task-oriented training.
References
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, et al. (2020) Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 141: e139-e596. [crossref]
- Wafa HA, Wolfe CDA, Emmett E, Roth GA, Johnson CO, et al. (2020) Burden of Stroke in Europe: Thirty-Year Projections of Incidence, Prevalence, Deaths, and Disability-Adjusted Life Years. Stroke 51: 2418-2427. [crossref]
- Center for Disease Control and Prevention (CDC) Stroke Facts. 2022. Accessed November 3, 2022. https: //www.cdc.gov/stroke/facts.htm
- Hatem SM, Saussez G, Della Faille M, Prist V, Zhang X, et al. (2016) Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front Hum Neurosci 10: 442. [crossref]
- Johnston TE, Keller S, Denzer-Weiler C, Brown L (2021) A Clinical Practice Guideline for the Use of Ankle-Foot Orthoses and Functional Electrical Stimulation Post-Stroke. J Neurol Phys Ther 45: 112-196. [crossref]
- Tashiro H, Isho T, Takeda T, Nakamura T, Kozuka N, et al. (2019) Life-Space Mobility and Relevant Factors in Community-dwelling Individuals with Stroke in Japan: A Cross-sectional Study. Prog Rehabil Med 4: 20190014. [crossref]
- Choo YJ, Chang MC (2021) Effectiveness of an ankle-foot orthosis on walking in patients with stroke: a systematic review and meta-analysis. Sci Rep 11: 15879. [crossref]
- Salbach NM, Mayo NE, Robichaud-Ekstrand S, Halney JA, Richards CL, et al. (2005) The effect of a task-oriented walking intervention on improving balance self-efficacy poststroke: a randomized, controlled trial. Journal of the American Geriatric Society 53: 576-582. [crossref]
- Rensink M, Schuurmans M, Lindeman E, Hafsteinsdóttir T (2009) Task-oriented training in rehabilitation after stroke: systematic review. J Adv Nurs 65: 737-54. [crossref]
- Lennon S, Ashburn A, Baxter D (2006) Gait outcome following outpatient physiotherapy based on the Bobath concept in people post stroke. Disability and Rehabilitation 28: 873-881. [crossref]
- Knox M, Stewart A, Richards CL (2018) Six hours of task-oriented training optimizes walking competency post stroke: a randomized controlled trial in the public health-care system of South Africa. Clin Rehabil 32: 1057-1068. [crossref]
- Kim B, Park Y, Seo Y, Park S, Cho H, et al. (2016) Effects of individualized versus group task-oriented circuit training on balance ability and gait endurance in chronic stroke inpatients. J Phys Ther Sci 28: 1872-5.
- Chan D, Chan C, Au D (2006) Motor relearning programme for stroke patients: A randomized controlled trial. Clinical Rehabilitation 20: 191-200. [crossref]
- Leroux A, Pinet H, Nadeau S (2006) Task-oriented intervention in chronic stroke: Changes in clinical and laboratory measures of balance and mobility. American Journal of Physical Medicine and Rehabilitation 85: 820-830. [crossref]
- Salbach NM, Mayo NE, Wood-Dauphinee S, Hanley JA, Richards CL, et al. (2004) A task-orientated intervention enhances walking distance and speed in the first year post stroke: a randomized controlled trial. Clinical Rehabilitation 18: 509-519. [crossref]
- Dean CM, Richards CL, Malouin F (2000) Task-related circuit training improves performance of locomotor tasks in chronic stroke: a randomized, controlled pilot trial. Archives of Physical Medicine and Rehabilitation 81: 409-417. [crossref]
- Van Peppen RPS, Kwakkel G, Wood-Dauphinees S, Hendricks HJM, Van der Wees PhJ, et al. (2004) The impact of physical therapy on functional outcomes after stroke: what’s the evidence? Clinical Rehabilitation 18: 833-862. [crossref]
- Pollack A, Baer G, Pomeroy V, Langhorne P (2007) Physiotherapy treatment approaches for the recovery of postural control and lower limb function following stroke. Cochrane Database of Systematic Review CD001920. [crossref]
- Scully A, Tan D (2019) Within-Assessment Variability of the GAITRite System in People with Stroke. Am J Phys Med Rehabil 98: 446-449. [crossref]
- Alghadir AH, Al-Eisa ES, Anwer S, Sarkar B (2018) Reliability, validity, and responsiveness of three scales for measuring balance in patients with chronic stroke. BMC Neurol 18: 141. [crossref]
- Blum L, Korner-Brtnsky N (2008) Usefulness of the Berg balance Scale in stroke rehabilitation: a systematic review. Physical Therapy 88: 559-566,. [crossref]
- Malik AN, Masood T (2021) Task-oriented training and exer-gaming for improving mobility after stroke: A randomized trial. J Pak Med Assoc 71: 186-190. [crossref]
- NG SS, Hui-Chan CW (2005) The Timed Up & Go test: its reliability and association with lower-limb impairments and locomotor capacities in people with chronic stroke. Archives of Physical Medicine and Rehabilitation 86: 1641-1647. [crossref]
- Bayona NA, Bitensky J, Salter K, Teasell R (2005) The role of task-specific training in rehabilitation therapies. Topics in Stroke Rehabilitation 12: 58-65. [crossref]
- Lewthwaite R, Winstein CJ, Lane CJ, Blanton S, Wagenheim BR, et al. (2018) Accelerating Stroke Recovery: Body Structures and Functions, Activities, Participation, and Quality of Life Outcomes From a Large Rehabilitation Trial. Neurorehabil Neural Repair 32: s150-165. [crossref]