Abstract
Hypothalamic hamartoma is a well-known neurological rare cause of central precocious puberty and gelastic seizures and may be asymptomatic for long period. It is rare and non-progressive tumor like congenital malformation. Precocious puberty defined as children attained the puberty before age of 8 years in girls and 9 years in boys. We present such a case of precocious puberty due to hypothalamic hamartoma in 5 year old boy and its radiological imaging findings.
Keywords
Hamartoma, hypothalamic, precocious, puberty, central cause
Introduction
Hypothalamic hamartoma is a rare non progressive tumor like well-organized congenital malformation of tuber cinereum in the floor of third ventricle [1-4]. It causes the classical spectrum or trait of gelastic seizures, precocious puberty and developmental delay or behavioral disorder [1,3]. It is most usual neurological cause of central precocious puberty.2 This condition may be asymptomatic for long period, or may present with clinical appearance and symptoms of precocious puberty and complex partial seizures refectory to anticonvulsant drugs [1,2]. One third of patients with hypothalamic hamartoma can be present with precocious puberty and it is defined as children attained the puberty before age of 8 years in girls and 9 years in boys [1,4,5]. Furthermore precocious puberty is divided into gonadotropin releasing hormone (GnRH)-dependent/central and gonadotropin releasing hormone (GnRH)-independent / peripheral precocious puberty [4]. Contrast enhanced MRI is investigation of choice and play important role in diagnosis of hypothalamic hamartoma [2,3] It appears as well-defined non enhancing lesion in floor of third ventricle showing similar signal intensity to the grey matter of brain parenchyma [3,4,6]. Gold standard treatment option for isolated central precocious puberty due to hypothalamic hamartoma is long acting analogs agonists of GnRH (GnHas) with good efficacy and safety [4,7].
Case Report
5 Years old boy came in paediatric outpatient department of Liaquat National Hospital with complain of faster growth of child than expected according to his father. On further questioning child has also history of epileptic laughter (gelastic seizures) 1-2 times, 2-3 months back for which he has taken antiepileptic drugs from local doctor in periphery of Afghanistan.
On local examination there were axillary and pubic hair and enlargement of penis measured about 4-5 cm in length. This was classified as TANNER stage (sexual maturity rating) 04 (Figure 1). Neurological examination was normal with Glasgow coma scale (GCS) of 15/15. Electroencephalogram (EEG) was recommended to see the cause of previous history of epileptic seizures was negative. His baseline laboratory investigations turned out to be within normal limits. On the basis of clinical and examination diagnosis of precocious puberty was made. His endocrinology related laboratory investigations were deranged. Follicle Stimulating Hormone (FSH) 4.11 (N= 1.9 mIU/ml), Luteinizing Hormone (LH) 9.82 (N1.3 mIU/ml) Testosterone 1500 ng/dL and Testosterone/Estradiol T/E2 ratio 45 pg/ml. All these investigations are raised and not normally corresponding to the patient’s age. Thyroid Function Tests (TFT) were within the normal limit.

Figure 1: Enlarged penis and appearance of pubic hair not corresponding to the patient’s actual age
He underwent the contrast enhanced MRI brain which showed abnormal signal intensity mass arising from the tuber cinereum in the region of hypothalamus. It appeared iso-intense to grey matter on T1 and T2 weighted images and showed no post contrast enhancement. It measured about 0.9 x 1.1 cm. The lesion was very small in size and has no mass effect or compression over the adjacent brain parenchyma. This was diagnosed as hypothalamic hamartoma. (Figures 2 and 3). Patient also underwent the X-ray right hand and elbow according to the radiological protocol to see the exact age of patient which showed 15 years reported by the experienced radiologist (Figure 4). During hospital stay course patient was asymptomatic and discharged on long acting analogs agonists of GnRH (GnHas). Follow-up was recommended in outpatient department of endocrinology.
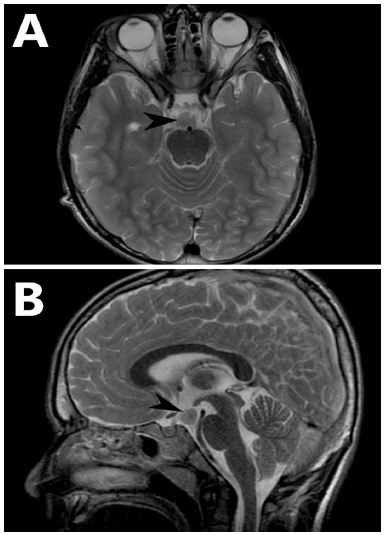
Figure 2: A Axial T2 weighted image and B sagittal T2 weighted image show abnormal signal intensity mass arising from the tuber cinereum in the region of hypothalamus. It appears iso-intense to the brain parenchyma (black arrow head)
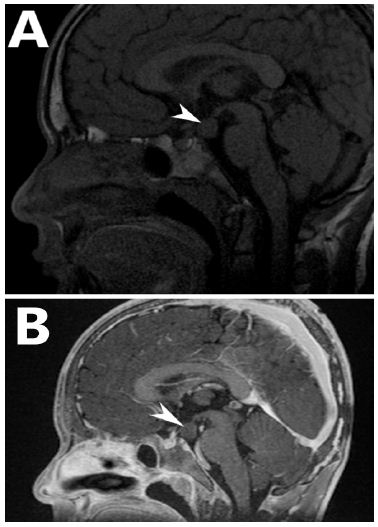
Figure 3: A sagittal plain T1 weighted image and B sagittal contrast enhanced T1 weighted image show abnormal signal intensity mass arising from the tuber cinereum in the region of hypothalamus. It appears iso-intense to brain parenchyma and show no post contrast enhancement (White arrow head)

Figure 4: A anterior-posterior elbow, B lateral elbow and C anterior-posterior wrist X-rays show bone age of 15 years
Discussion
Previously Hypothalamic hamartoma used to be an uncommon finding and was estimated to occur in one person per one million population,1 however with timely advancement in the field of Radiology and better clinical recognition, the early diagnosis has now become possible and its incidence has significantly decreased [1,2].
Most patients usually present in the first or second decade of life [1-3]. Precocious puberty is the most common presentation, however larger hamartomas are less likely to produce precocious puberty [2,3]. Other clinical presentations include developmental delay, attention deficit or hyperactivity disorder and anxiety [1-4]. A very specific feature of hypothalamic hamartoma is Gelastic seizure [1-3]. In our case, hamartoma measured up to 1cm on MRI brain (Figure 2) and patient was presented with complaints of both precocious puberty and laughing fits (Gelastic seizures).
On MRI, hypothalamic hamartomas produce soft tissue intensity masses which are isointense to grey matter on T1WI and hyperintense on T2WI [2,3]. They are homogeneous and sharply marginated by the surrounding CSF with no post contrast enhancement [2,3,6]. Calcification is rare and hemorrhage is not described in these lesions [2,3]. This classical appearance of soft tissue intensity mass in the region of hypothalamus was also observed in our patient (Figure 2).
Patients with central precocious puberty are usually managed conservatively [2], for progressive central precocious puberty, treatment with a depot GnRH agonist is suggested and is generally continued for 11 years [2-4]. However, surgery including resection or disconnection through craniotomy or trans-spheroidal approach can be helpful in cases of poorly controlled epilepsy [2-6], to our patient, we advised long acting analogs agonists of GnRH (GnHas) with a follow up in OPD.
Conclusion
Hypothalamic hamartomas are rare congenital malformation seen in floor of third ventricle. Precocious puberty is most usual presenting feature. MRI brain play important role in diagnosis of these lesions. Radiologist should aware of imaging findings of hypothalamic hamartoma and should examine the hypothalamic region properly in suspected cases as they can be easily missed due to small size. Bone age can be assessed by using the wrist X-ray and we can also observe the slowing of bone growth after treatment by X-ray wrist recommendation in every 6th month.
References
- Qasim BA, Mohammed AA (2020) Hamartoma of hypothalamus presented as precocious puberty and epilepsy in a 10-year-old girl. International Journal of Surgery Case Reports 77: 170-173. [crossref]
- Mahmood R, Al Taei TH, Samah Al Obaidi MD (2019) Hamartoma of the Hypothalamus. Bahrain Medical Bulletin 41.
- Kalekar T (2015) Hypothalamic Hamartomas: Two Cases. Open Journal of Medical Imaging 5: 20.
- Sharma P, Acharya N, Guleria TC (2020) Hypothalamic hamartoma presenting as central precocious puberty: a rare case report. International Journal of Contemporary Pediatrics 7: 1634.
- Mahajan ZA, Mehta SR (2020) Central precocious puberty: A case report. Medical Journal of Dr. DY Patil Vidyapeeth 13: 413.
- Boyko OB, Curnes JT, Oakes WJ, Burger PC (1991) Hamartomas of the tuber cinereum: CT, MR, and pathologic findings. American Journal of Neuroradiology 12: 309-314. [crossref]
- Eugster EA (2019) Treatment of central precocious puberty. Journal of the Endocrine Society 3: 965-972. [crossref]