Abstract
Mind Genomics can be used to study language-based frontotemporal dementia (FTD) by synthesizing the cognitive and behavioral profiles of individuals. This personalized approach helps identify challenges and tailor interventions to each person’s needs. By recognizing the diversity of mind-sets within the FTD population, more effective strategies for diagnosis, treatment, and care can be developed. The paper shows how to use AI (Socrates as a Service) to synthesize a user-defined number of mind-sets, here three FTD mind-sets: Apathetic Mind-Set, Disinhibited Mind-Set and Compulsive Mind-Set. The combination of Mind Genomics and AI has the potential to revolutionize research, diagnosis, and care for FTD, leading to better outcomes and improved quality of life.
Introduction
Frontotemporal dementia (FTD) is a neurodegenerative disease which primarily affects the frontal and temporal lobes of the brain. FTD leads to changes in behavior, personality, and language skills. Common symptoms include changes in behavior, personality, and language abilities. Sufferers may exhibit apathy, social disinhibition, impulsivity, and emotional bluntness. The speech of FTD sufferers may become fluent but lack meaning, or they may struggle to find the right words. As the disease progresses, patients may develop memory loss and lose the ability to perform daily activities. It is important for nurses to understand these language changes in order to communicate with, and care for FTD patients [1-4]. Talking to people who have frontotemporal dementia is an important part of giving them good care and support. When working with these people, nurses need to be patient, kind, and understanding. It is best to speak slowly, use simple words, and give the patient a lot of time to answer. Body language, such as gestures, facial expressions, and the tone of one’s voice, can also help get the point across. To start a therapeutic relationship and look out for the patient’s well-being, one needs to build trust and a relationship with them. Patients may have trouble expressing their needs, feelings, and thoughts because their language skills are affected. It is helpful to use simple words, speak slowly and clearly, and show things to help people understand. It’s important to build trust and a relationship with patients so they feel safe and understood. Getting into a routine and being consistent with how one talks to them can help FTD patients feel less anxious and confused and improve their overall quality of life [5-8]. Artificial intelligence (AI) can help us learn a lot about how to help FTD sufferers. AI can help researchers find patterns, predict how the disease will progress, and come up with personalized treatment plans by looking at data from people who have FTD. AI can also create virtual simulations which tutor healthcare professionals as they practice talking to FTD patients, learning how to do it better. Incorporating AI into nursing may be a strong positive step in the evolution of medicine in this age of intelligent computing [9-11]. AI may be able to help nurses gain insight and information about how FTD suffers think and reason, giving the nurses a way to come up with better ways to talk to the FTD sufferer. By looking at data and putting it all together. AI can help nurses guess what might happen, allowing the nurse to modify their approach to fit the needs of each FTD sufferer. Nurses can learn more about how to care for people with FTD by using AI to look at huge amounts of data and then simulate different situations [12-14].
Learning about FTD by Using Mind Genomics Discoveries Regarding Mind-Sets
Mind Genomics is an emerging science focusing on how people perceive and react to the world of the everyday. Mind Genomics has a long history of application in the social sciences, marketing, and consumer research to better understand human behavior. Researchers can better connect with various groups of people by dividing populations according to their mindsets. Research has demonstrated that this customized method outperforms generic messaging when it comes to achieving desired responses from specific audiences. Mind Genomics works by developing questions about a topic, these questions telling a story, and then creating answers to the questions. The process takes the answers (aka elements, stand-alone phrases which paint a word picture), combining them into short vignettes, presenting the vignettes to survey takers (respondents). The ratings assigned by the respondents are then deconstructed by statistics (ordinary least squares regression). The output of regression, coefficients showing the ‘driving power’ of the elements, is subject to cluster analysis [15]. The output of the foregoing statistical journey are sets of people who think differently about the same specific topic, and thus who should be treated differently through communication. The Mind Genomics studies continue to reveal different clusters of people, different mind-sets. The vignettes were set up so that each respondent evaluated a totally different set of vignettes. The most recent design calls for four questions, and four answers to each question, but earlier versions called for four questions and nine answers to each question (60 vignettes), or six questions and six answers to each question). It was impossible to game the system. The mindsets ended up being coherent, interpretable, and often meaningful for subsequent communication. The outcome was thus the development of specific, granular knowledge about aspects of a topic, as well as the precise words to which the different mind-sets would react [16-18].
The Mind Genomics Process and the Introduction of AI to Help Coach the Users
As stated above, Mind Genomics was created to help users (e.g., researchers) discover how people think about the world of the ordinary, doing so by creating questions and then answers to those questions (elements). Whereas on the surface this requirement seems fairly easy, the reality in practice was anything but that. The reality turned into the recognition that structured thinking to do the seemingly simple task was more elusive. At first in 2015 and later the answer was extensive training. The training, however, was also an inhibitor, converting the satisfaction of learning into the pain of learning a new tool. The development of AI around 2022-2023 which generated the breakthrough, shown descriptively in Panel A as Idea Coach. Idea Coach was the link to AI. A specific program was developed to create questions and answers. This program used AI, and was called, not surprisingly, Socrates as a Service.
Figure 1 shows the process which led to the AI, and in turn to this paper.
- Panel A shows the request to develop four questions. The topic is communicating with and helping patients with FTD. As just noted, the response to providing the questions was eventually the creation of four questions, but with a great deal of angst, insecurity, and often simple frustration. It was at this point that many prospective users simply abandoned the process.
- Panel B shows the input to AI (Idea Coach). The user types the request into the box. The AI in Mind Genomics is a programmed set of queries (SCAS, Socrates as a Service). SCAS is programmed using ChatGpt 3.5 [19,20] to provide the questions, and the answers, depending upon the information provided to it. The imortant thing is that SCAS is quick, returning in 15 seconds, allows for numerous iterations so the user can get an education at the time when SCAS is used, and finally returns with additional post-use analyses, also in depth, serving as a way to increase learning.
- Panel C shows the output from SCAS. SCAS is programmed to provide 15 questions for each iteration. Subsequent iterations generate new sets of questions. When the user runs 10 iterations, it is likely that the result will be a set of 100+ unique questions embedded in the total of 150 questins returned by SCAS. The 100 or so questins creates an extensive reference library of questions, each one of which can be addressed.
- Panel D shows the selection of a random set of four questions to be entered into the templated sytem for Mind Genomics. These questions can be selected ‘as is’ from the SCAS output, or edited, and sometimes the questions can be inserted manually by the user, without any help from AI.
- Panel E shows the request for four answers for Question 1 of 4. The question comes directly from the first question in Panel D.
- Panel F shows the first eight of 15 answers for Question 1. Each iteration of SCAS answers one of the four questions selected, and generates 15 answers. As before, the answers can be edited, the request for answers can be iterated, and the question itself can be edited to shape the nature of the answers.
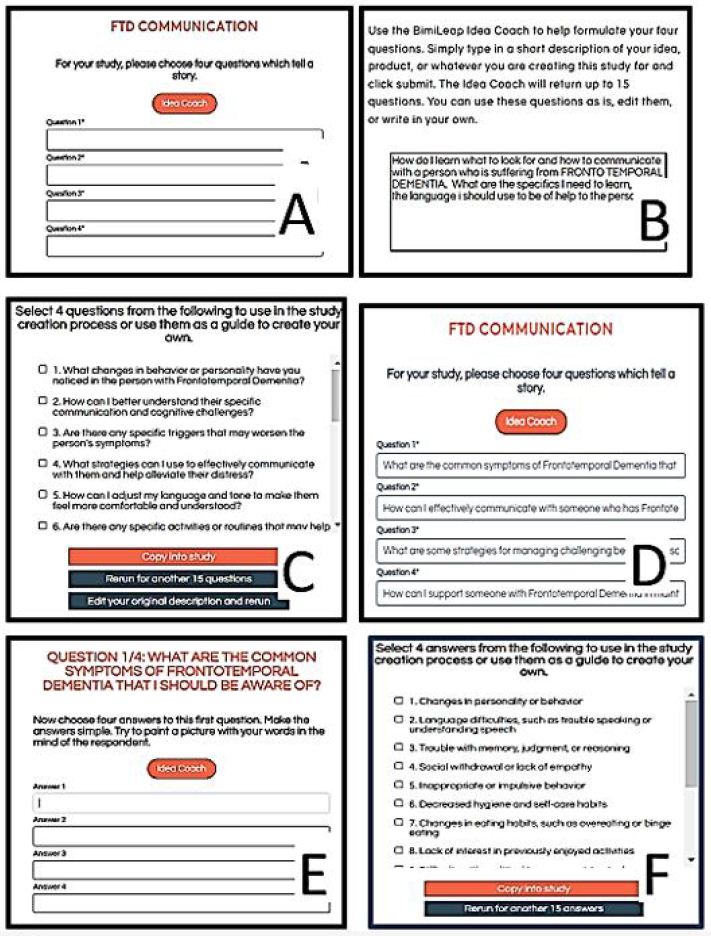
Figure 1: The process of Mind Genomics. Panel A shows the request for four questions. Panel B shows the squib, viz., the background to SCAS (the programmed AI). Panel C shows a subset of the 15 questins which emerge from each iteration. Panel D shows the selected questons automatially entereed into the Mind Genomics template. Panel E shows the request for 15 answers to questin 1, with the text of the quetisn at the top of the screen shot. Panel F shows some of the 15 answers emergng from SCAS.
Moving Beyond User-generated Questions to AI Generated Questions
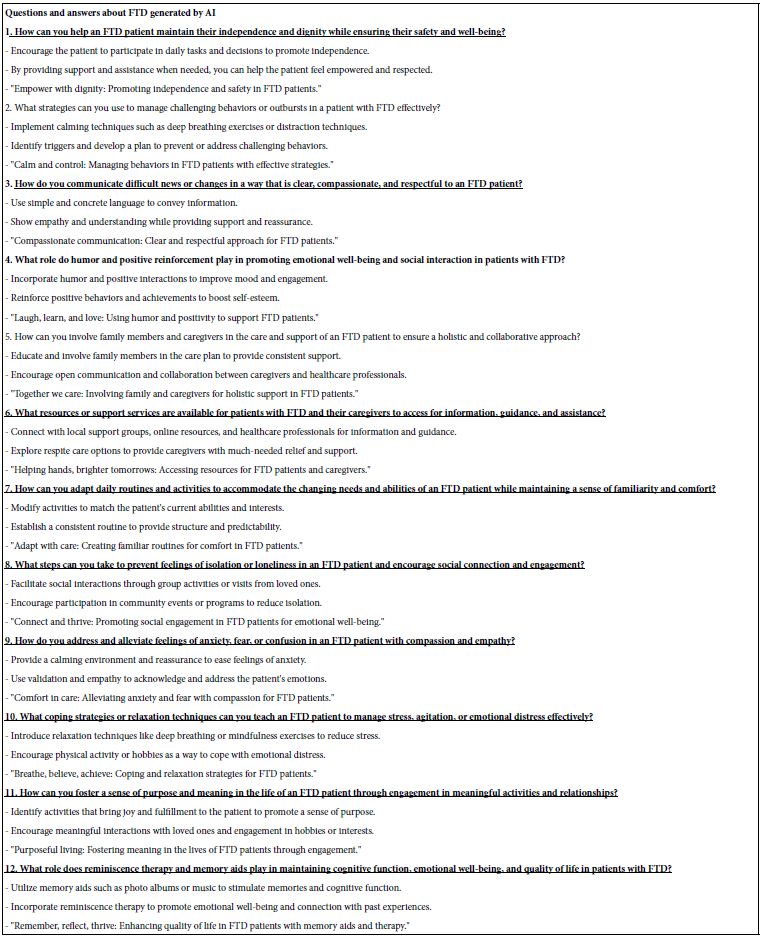
The introduction of AI into the Mind Genomics platform was done with the idea that the SCAS approach would be a source of additional learning. To that end, the creation of 15 questions was made a standard feature of the in Figure 1, Panel B. Any time that the user would engage SCAS through the user-provided squib, there outcome would be a set of 15 questions. As part of using the system, several times the 15 questions emerging from SCAS were ‘accidentally’ copied and then used for the next iteration of SCAS. The SCAS dutifully returned with an answer to each question. When this happy state of affairs was recognized, it was not long before the questions were ‘imported’ into SCAS, with requests to provide more than just a single answer. Table 1 shows the results of tentative steps to push SCAS to provide two answers and a ‘slogan’ for each of 12 questions which had had emerged from SCAS in the previous iteration. It is virtually impossible to detect the fact that these questions and answers all come from AI.
Table 1: Questions and answers about FTD, all generated by AI, with the requested information alone coming from the human user.
Introducing Mind Genomics Thinking into AI by Hypothesizing the Nature of Three FTD Mind-sets
It was the discovery that the AI embedded in SCAS could do more than simply respond to questions which generated the next step. The question was what AI would do when given specific background information assumed to be ‘true,’ and then instructed to provide information to ‘flesh out’ the background information. The AI would be given specific information and specific requests. The ‘test’ began by telling AI that for FTD (language loss variety) there are three major mind-sets. We do not specify what they are, nor anything else. The only information that the AI receives is the specification of three mind-sets, followed by the instruction to answer specific questions. The actual information provided to the AI was thus minimal. The statement that there were three mind-sets for SCAS to ‘create’ the mind-sets in detail: Apathetic, Disinhibited, and Compulsive, respectively. Table 2 describes the Apathetic Mind-Set, Table 3 the Disinhibited Mind-Set, and Table 4 the Compulsive Mind-Set.
The final simulation effort appears in Table 5. Table continues the effort of answering a series of questions, moving beyond simple answers by directing SCAS to provide two answers and a memorable slogan.
Table 2: AI-synthesized characteristics of the Apathetic Mind-Set
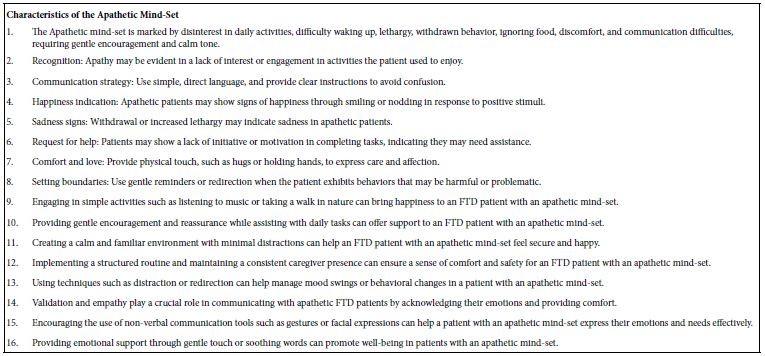
Table 3: AI-synthesized characteristics of the Disinhibited Apathetic Mind-Set
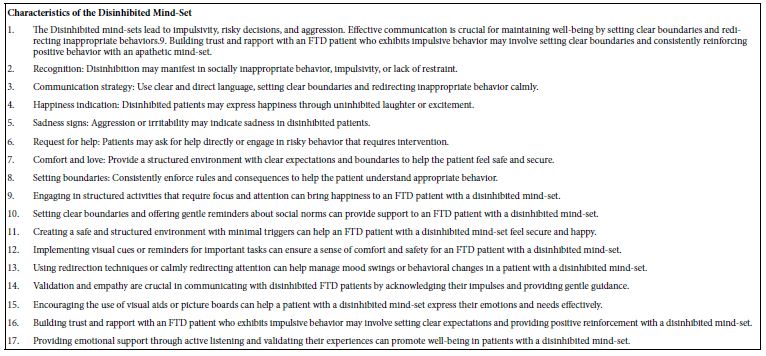
Table 4: AI-synthesized characteristics of the Compulsive Mind-Set
Table 5: Answers to direct questions posed by the user (Part 1) and then additional information ‘volunteered’ by SCAS afterwards. The table is constructed from several iterations.
Discussion and Conclusions
By employing Mind Genomics in the study of FTD, researchers can uncover valuable insights into the cognitive and behavioral profiles of individuals with the disease. This personalized approach can help identify specific challenges and tailor interventions to address the individual needs of each person living with FTD. By recognizing the diversity of mind-sets within the FTD population, we can better understand the complexities of the disease and develop more effective strategies for diagnosis, treatment, and care. Through the application of Mind Genomics in the field of FTD research, we can gain a deeper understanding of the cognitive and behavioral changes associated with the disease. By identifying distinct mind-sets within the FTD population, we can tailor interventions to address the specific challenges faced by individuals with different profiles. This personalized approach can lead to more targeted and effective care strategies to improve the quality of life for individuals living with FTD and their caregivers. In summary, Mind Genomics offers a powerful tool for understanding the diverse ways in which individuals with language-based FTD experience and navigate the world. By recognizing and synthesizing the unique mind-sets present within the FTD population, we can develop more personalized and effective interventions that address the diverse needs of individuals affected by the disease. This approach has the potential to revolutionize the way we approach research, diagnosis, and care for individuals with FTD, ultimately leading to better outcomes and improved quality of life.
Acknowledgement
Howard Moskowitz gratefully acknowledges the ongoing of help of Ms Hilda Varnum in this effort, and the contribution of Ms Arlene Gandler who provided the original stimulation to write this paper.
References
- Bang J, Spina S, Miller BL (2015) Frontotemporal dementia. The Lancet 386: 1672-1682.
- Onyike CU, Diehl-Schmid J (2013) The epidemiology of frontotemporal dementia. International Review of Psychiatry 25: 130-137. [crossref]
- Weder ND, Aziz R, Wilkins K, Tampi RR (2007) Frontotemporal dementias: a review. Annals of General Psychiatry 6: 1-10. [crossref]
- Young JJ, Lavakumar M, Tampi D, Balachandran S, Tampi RR (2018) Frontotemporal dementia: latest evidence and clinical implications. Therapeutic Advances in Psychopharmacology 8: 33-48. [crossref]
- Caceres BA, Frank MO, Jun J, Martelly MT, Sadarangani T, et al. (2016) Family caregivers of patients with frontotemporal dementia: An integrative review. International Journal of Nursing Studies 55: 71-84. [crossref]
- Schmid J, Schmidt EM, Nunnemann S, Riedl L, Kurz A, et al. (2013) Caregiver burden and needs in frontotemporal dementia. Journal of Geriatric Psychiatry and Neurology 26: 221-229. [crossref]
- Edberg AK, Edfors E (2008) Nursing care for people with frontal-lobe dementia–difficulties and possibilities. International Ppsychogeriatrics 20: s 361-374. [crossref]
- Rasmussen H, Hellzen O, Stordal E, Enmarker I (2019) Family caregivers experiences of the pre-diagnostic stage in frontotemporal dementia. Geriatric Nursing 40: 246-251. [crossref]
- Li R, Wang X, Lawler K, Garg S, Bai Q, Alty J (2022) Applications of artificial intelligence to aid early detection of dementia: A scoping review on current capabilities and future directions. Journal of Biomedical Informatics 127. [crossref]
- Merkin A, Krishnamurthi R, Medvedev ON (2022) Machine learning, artificial intelligence and the prediction of dementia. Current Opinion in Psychiatry 35: 123-129. [crossref]
- Ranson JM, Bucholc M, Lyall D, Newby D, Winchester L, et al. (2023) Harnessing the potential of machine learning and artificial intelligence for dementia research. Brain Informatics 10. [crossref]
- Osaki NT, Ghosh S, Palaniappan SK, Maeda K (2024) Enabling personalization for digital cognitive stimulation to support communication with people with dementia: Pilot intervention study as a prelude to AI developm JMIR Formative Research 8. [crossref]
- Rasmussen HEGE, Hellzen OVE (2013) The meaning of long-term caregiving for patients with frontal lobe dementia. International Journal of Qualitative Studies on Health and Well-being 8. [crossref]
- Wylie MA, Shnall A, Onyike CU, Huey ED (2013) Management of frontotemporal dementia in mental health and multidisciplinary settings. International Review of Psychiatry 25: 230-236. [crossref]
- Likas A, Vlassis N, Verbeek JJ (2003) The global k-means clustering algorithm. Pattern recognition 36: 451-46. [crossref]
- Moskowitz HR (2012) ‘Mind Genomics’: The experimental, inductive science of the ordinary, and its application to aspects of food and feeding. Physiology & Behavior 107: 606-613. [crossref]
- Moskowitz HR, Gofman A, Beckley J, Ashman H (2006) Founding a new science: Mind Genomics. Journal of Sensory Studies 21: 266-307.
- Porretta S, Gere A, Radványi D, Moskowitz H (2019) Mind Genomics (Conjoint Analysis): The new concept research in the analysis of consumer behaviour and choice. Trends in Food Science & Technology 84: 29-33.
- Wu T, He S, Liu J, Sun S, Liu K, et al. (2023) A brief overview of ChatGPT: The history, status quo and potential future development. IEEE/CAA Journal of Automatica Sinica 10: 1122-1136.
- Rosness TA, Haugen PK, Engedal K (2008) Support to family carers of patients with frontotemporal dementia. Aging and Mental Health 12: 462-466. [crossref]