A 85-year-old woman, with a previous history of pericarditis was admitted to the ED for dyspnoea with evident signs of congestive heart failure. The patient underwent two-dimensional transthoracic echocardiography that showed left ventricular ejection fraction of 40% with an akinetic postero-lateral wall. The postero-lateral wall shows a discontinuity of the myocardium at the apical segments with the evidence of a giant pseudoaneurysm (Ps): multiloculated in three different sac connected each other (Figure 1 panel A, online video 1).
The color-Doppler visualized at the neck of the Ps showed a systo-diastolic turbulent jet filling the multiloculated structure (Figure 1 panel B; online video 2). The apical 3-chamber view confirmed the large neck of the multiloculated Ps (Figure 2 panel A).

Figure 1: A. 2D transthoracic echocardiography, apical 4-chamber view. LV=left ventricle; LA=left atrium; RV=right ventricle; Numbers 1 to 3 are the multiple locations of the pseudoaneurysm. B. Color-Doppler echocardiography shows the communication with the Ps sac.
The previous patient history of pericarditis could have play a role, saving from dramatic rupture a silent myocardial infarction and leading to creation of a multiloculated sac. This case presents some complications of an untreated sub-acute myocardial infarction as Ps and mitral regurgitation secondary to the tethering of the mitral posterior leaflet. (Figure 2 panel B).
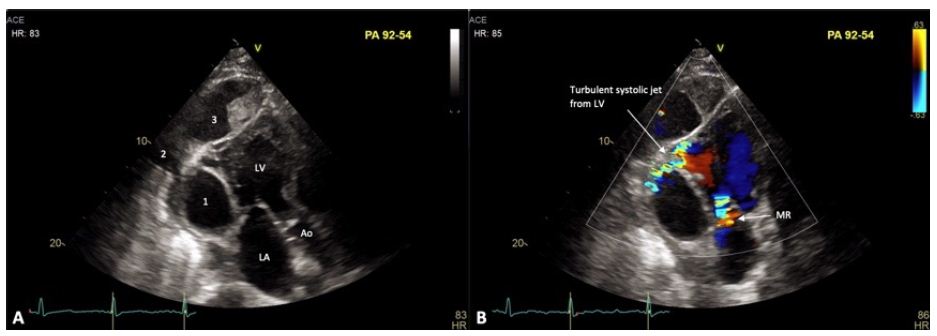
Figure 2: A. 2D transthoracic echocardiography, apical 3-chamber view. LV=left ventricle; LA=left atrium; Ao=aorta; Numbers to 3 are the multiple locations of the giant pseudoaneurysm. B. Color-Doppler echocardiography at apical 3-chamber view.
Considering the prohibitive surgical risk leading by age and co-morbidities after discussion at Heart Teem the patient was stabilized on optimal medical therapy and discharged. Untreated left ventricular Ps leads to loss of anterograde stroke volume and systemic cardioembolic events [1,2]. After myocardial infarction other common causes of Ps are: cardiac surgery, bacterial endocarditis and chest trauma [3].
Keywords
Acute myocardial infarction, Echocardiography, Left ventricular pseudoaneurysm
References
- Hung MJ, Wang CH, Cherng WJ (1998) Unruptured left ventricular pseudoaneurysm following myocardial infarction. Heart 80: 94-97. [crossref]
- Altinier A, Negri F, Belgrano M, Gianfranco Sinagra (2015) The eight-shaped heart: an incidental giant left ventricular pseudoaneurysm. Eur Heart J 36: 1488. [crossref]
- Frances C, Romero A, Grady D (1998) Left Ventricular Pseudoaneurysm. J Am Coll Cardiol 32: 557-561. [crossref]