Abstract
Already in the 1980s, the World Health Organization (WHO) has postulated to analyze in all medical fields differences between the sexes. But until now there is a disturbing lack of scientifically based and meaningful data over the whole area of gender dentistry – for prevention as well as for treatment. The aim of this study was to evaluate the actual situation described as an IS-analysis of literature review on the topic of gender dentistry with the sub-themes periodontal disease and tooth decay in the leading medical databases (Medline, Embase, BIOSIS Previews, Your Journals@Ovid, The Cochrane Library). We discuss these on the basis of an evidence-based guideline. For periodontal diseases we found no clear trend. Some studies showed no gender difference, others showed a higher prevalence for women or a higher prevalence for men. At the juvenile periodontitis and the occurring bacteria of periodontitis there were conflicting results as well. No simple statement can be made with respect to tooth decay, too. Respective studies merely show age as an important item. Totally it has to be noted that the scientific validity of some studies is not without any doubt as they are conducted with a too low number of clinical trials. Several studies are more than 15 years old, therefor providing a serious gender specific treatment in dentistry, future studies must increasingly incorporate and intensively discuss gender specific aspects.
Keywords
Caries, Dentistry, Gender, Men, Periodontitis, Women
Introduction
Already in the 1980s the World Health Organization (WHO) has postulated to analyze differences between sexes in all areas of medicine [1]. In the Vienna Declaration on investment in health of the WHO in 1992 was strongly admonished: “Maximum attention and urgency must be given to women’s health” [2]. Ten years later, in 2002, the WHO gender policy was written. The main objective of this policy is to enable a better health for women and men through modern health research, contributing programs and policies and to give due attention to the gender aspect [3]. And in the action plan 2000, “Gender Mainstreaming was mandatory prescribed in the medicine for all EU countries and decided in consequence” by the Austrian Federal Government as Univ.‐Prof. Dr. Margarethe Hochleitner [4]. The term “Gender Mainstrea-ming” was discussed for the first time in Nairobi already in 1985 on the 3rd UN World Conference of women and ten years later in 1995 the term has been further developed on the 4th UN World Conference of Women [5]. “Gender Mainstreaming” implies according to the BMFSFJ (German Federal Ministry for Family, Senior Citizens, Women and Youth): „… to take into account from the outset and periodically the different life situations and interests of women and men at all social projects, since there is no gender-neutral reality” (Bundesministerium für Familie, Senioren, Frauen und Jugend (Federal Ministry for Family Affairs, Senior Citizens, Women and Youth) 2012). And in the Basic Law was even expressly postulated: “To the actual enforcement of the equality between women and men the Government is expressly obliged by article 3, paragraph 2, sentence 2 Basic Law, it is an integral part of the political action of the Federal Government in all policy areas” [6]. The importance of a differentiated analysis with respect to gender-specific aspects is therefore obvious. Gender-specific considerations are nowadays no longer indispensable from dentistry. However the level of knowledge on this subject is until now surprisingly low. There is a disturbing lack of scientifically founded and reliable data in gender dentistry. “So far only little attention was paid to this topic in the German-speaking world, unlike in other countries. While gender research has found long ago entrance into scientific projects and teaching in medicine, the gender-specific dental, oral and maxillofacial surgery moves only slowly in the awareness of researchers and the practitioners, ladies and gentlemen. This topic is interesting and up to date, because just in dentistry in addition to biological differences, gender plays an important role“, so Priv.-Doz. Dr. Christiane Gleissner, 2011 [7]. To ensure a better dental care for male and female patients in the future, the present study delivers a systematic literature review on the topic of “Gender Dentistry”. The aim of this work is to offer a guideline-oriented, quality-based literature review, based on disease patterns, relevant for “Gender Dentistry”. Additionally all relevant studies have been analyzed, whether they meet the criteria and requirements of the WHO-Guidelines.
Material and Methodology
In the following we describe the preparation, the implementation of the literature review, the selected medicine database and search items as well as the handling of the results. The methodical approach is based on a guideline creation according to recommendation Rec(2001)13 of the Council of Europe (47 European States comprehending European international organizations), the AWMF (Work Community Association of scientific medical companies) [8] and the ZZQ Berlin (Center for dental quality) [9]. The main literature database was chosen to identify the current state of research regarding “gender” dentistry for evidence-based results. The selection was done on five databases: Embase, Your Journals@Ovid, The Cochrane Library, Medline, BIOSIS Previews. Access to these databases was given by the network of the University of Ulm. The search was as follows: for each clinical picture a search item has been set:
- Periodontitis: gender periodontitis
- caries susceptibility: gender caries
Then the specified keyword was given into the database and search started. The number of results was recorded. To narrow this large amount of results step by step, the ability of the program was used to divide the results by relevance. High relevance: 5 stars, low till no relevance: 4 till 0 stars. Then the option “five stars only” was made to observe only items with the highest relevance. The amount of search results, which now appeared, was also recorded. Depending on the number of results, the year of publication was still restricted. This and the new amount of search results were also recorded. Then the search results were read and the relevant publications were saved on RefWorks, a reference management software. The corresponding references, which are identified as possible matches, were downloaded as full text or ordered via interlibrary loan to check their contents in detail. The received information was translated, summarized and explained under results. Sequence and classification in reference 1, 2, are ordered alphabetically by the author’s name. So there is no ranking. To ensure the relevance of the results of the literature review, a further update was carried out in September 2013. Here, all five medicine databases were searched again in the period August 2012 – September 2013, as described above. The newly found references were saved and added to the already existing and edited.
Periodontitis
Keyword: gender periodontitis (Table 1)
Table 1:
Table 1. Gender Periodontitis. Results of the literature review in the five databases BIOSIS Previews, The Cochrane Library, Embase, Your Journals@Ovid und Medline from August 2012 and September 2013 and the total amount of stored references
Results, references = articles
|
Medical database |
Basic Search |
Restriction to five stars |
Stored references August 2012 |
Stored references September 2013 |
Total references |
|
BIOSIS Previews |
8 491 results |
335 results |
16 references |
1 result |
17 references |
|
The Cochrane Library |
5 496 results |
26 results |
1 references |
0 results |
1 reference |
|
Embase |
10 882 results |
824 results 611 results |
14 references |
6 results |
20 references |
|
Your Journals @Ovid |
16 955 results |
17 results |
2 references |
0 results |
2 references |
|
Medline |
10 164 results |
673 results |
7 references |
6 results |
13 references |
Caries
Keyword: gender caries (Table 2)
Table 2. Gender caries. Results of the literature review in the five databases BIOSIS Previews, The Cochrane Library, Embase, Your Journals@Ovid und Medline from August 2012 and September 2013 and the total amount of stored references
Results, references = articles
|
Medical database |
Basic Search |
Restriction to five stars |
Stored references August 2012 |
Stored references September 2013 |
Total references |
|
BIOSIS Previews |
9001 results |
541 results |
14 references |
4 results |
18 references |
|
The Cochrane Library |
5513 results |
73 results |
4 references |
0 results |
4 references |
|
Embase |
16 371 results |
1179 results |
6 references |
3 results |
14 references |
|
Your Journals @Ovid |
17 004 results |
14 results |
0 references |
0 results |
0 references |
|
Medline |
16 716 results |
1125 results |
4 references |
11 results |
15 references |
Results
Periodontitis (Table 3, 4 & Figure 1)
Table 3. Results of the literature review on the topic of periodontitis. The total identified studies and the ultimately evaluated.
|
Amount of articles total |
53 |
|
Amount of evaluated articles |
21 |
Table 4. Results for the articles about periodontal diseases, which appeared before and right/after the year 2000, as well as a subject number higher or equal or lower 500 subjects or any information on the number of the person being tested.
|
Year of publication before 2000 |
5 |
|
Year of publication after/right 2000 |
16 |
|
Number of subjects higher/equal than 500 |
4 |
|
Number of subjects lower than 500 |
7 |
|
No information about the number of subjects |
10 |
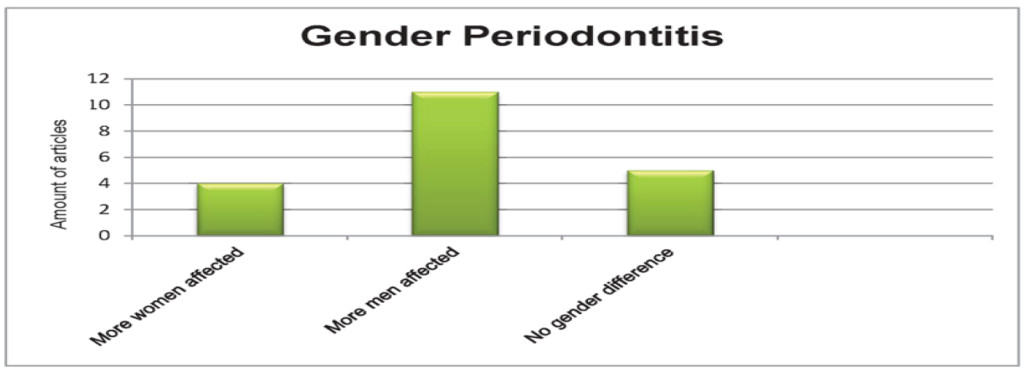
Figure 1. Gender Periodontitis. Gender-specific distribution of the edited articles about periodontal disease.
Caries
(Table 5, 6 & Figure 2)
Table 5. Results of the literature review on the topic of caries. The total identified studies and the ultimately evaluated.
|
Amount of articles total |
51 |
|
Amount of evaluated articles |
29 |
Table 6. Results for the articles about caries, which appeared before and right/after the year 2000, as well as a subject number higher or equal or lower 500 subjects or any information on the number of the person being tested.
|
Year of publication before 2000 |
4 |
|
Year of publication after/right 2000 |
25 |
|
Number of subjects higher/equal than 500 |
14 |
|
Number of subjects lower than 500 |
9 |
|
No information about the number of subjects |
5 |
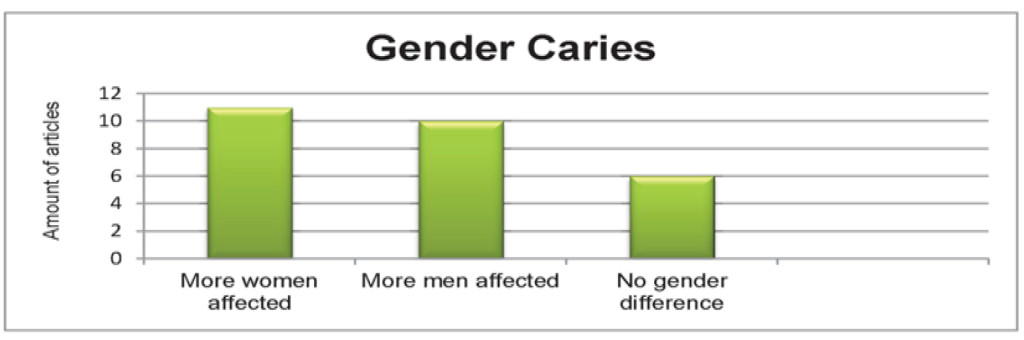
Figure 2. Gender Caries. Gender distribution of the edited articles about caries.
Discussion
Methodology
The current state of research in gender dentistry was collected with the help of a literature review, based on the creation of evidence-based guidelines. These guidelines summarize current knowledge, expert opinions and results of various working groups. Known and respected medical database were analyzed within the period of 10th – 20th of August 2012, and with another search from 12th -14th of September 2013.
Discussion related to the analyzed diseases
We have to notice that no clear result could be found and no simple conclusion for practice and teaching can be drawn. There are still too few studies, which offer enough reliability on gender-specific aspects. Some papers offer inconsistent results lacking of possible general evaluations. Further research seems to be indicated.
Periodontitis
The available results of our investigation of the present studies on periodontal disease are not satisfying. There are eleven studies that have proven that men suffer more frequently from periodontitis than women [10–20] However, there are five studies showing no gender aspect at all [21–24].
There are four further studies that show that women would more often suffer from periodontal diseases than men [13, 23, 25–27] The latest studies show a higher incidence for men. Aggressive periodontitis is more common in women and chronic periodontal disease occurs more often in men [13]. The loss of attachment points towards men [12]. One study indicates juvenile periodontitis more often in women [25], but a different study suggests that the distribution of men and women is equal [21]. Furthermore there shown, that there were differences between men and women related to periodontal disease bacteria [16], another study, however, show no difference [26]. The majority of results indicates a higher incidence in men regarding periodontal disease.
When evaluating the aspect of periodontal disease, many other factors, such as age and hormone levels of women do play an important role, because the periodontal disease is known to be a multifactorial disease. All factors should be detected and examined. These aspects should be included in further studies, observed, presented and evaluated in order to get scientific based information, providing additional value for dental treatment. The evaluated studies are lacking to draw conclusions due to limited numbers of subjects and mixed timelines.
Caries
The examination of the studies on caries does not give a uniform result. There are six studies which show no gender-specific differences [28–33]. In contrary studies have proven that women have a greater rate of caries than men [33, 34–43].
The following studies however showed higher rates of tooth decay in men. Only one of these studies was performed in adults [44]. The other five studies have been conducted on children [37, 38, 45–51]. Therefore, there seems to be a tendency for higher caries rates in women. However, depending on the age of the subjects. There are studies demonstrating that boys have higher levels of tooth decay, but the tendency is expanding in adulthood towards women [37, 38].
Studies that examine a multicausal illness such as caries must include all ages and have to be divided into gender, age, eating habits, socioeconomic background, etc. to obtain useful information. Especially in countries with huge emphasis on prophylaxis and caries prevention, e.g. Germany, this study design is essential. On the subject of dental caries the actuality of the studies is satisfactory, the number of clinical trials however mediocre.
The authors declare that they have no competing interests.
References
- Kautzky-Willer A, Tschachler E (2012) Gesundheit: Eine Frage des Geschlechts. Orac/Verlag Kremayr & Scheriau KG, Wien.
- WHO (1992) (06.12.13) http://www.euro.who.int/__data/assets/pdf_file/0019/ 114238/E93952G.pdf.
- WHO (2002) (06.12.13): http://www.who.int/gender/documents/engpolicy.pdf,
- Hochleitner Margarethe (2013) (6.12.13) http://fgz.imed.ac.at/kongresse/pdf_kongr/saalfelden2013.pdf.
- Meuser Michael, Neusüß Claudia, (2002) Gender Mainstreaming – eine Einführung. In: dies. (Hrsg.): Gender Mainstreaming. Konzepte – Handlungsfelder – Instrumente. Bundeszentrale für politische Bildung S9–22.
- BMFSFJ 2012 (06.12.13): http://www.bmfsfj.de/BMFSFJ/gleichstellung,did= 192702.html.
- Gleissner Christiane (07.12.13) http://gendermed.info/Gerade-in-der-Zahnmedizin-spielt-der.79.0.2.html.
- AWMF (26.10.13) http://www.awmf.org/.
- ZZQ (23.08.2013) http://www.zzq-berlin.de/leit.htm.
- Bain JL, Lester SR, Henry WD, Bishop CM, Turnage AA, et al. (2009) Comparative gender differences in local and systemic concentrations of pro-inflammatory cytokines in rats with experimental periodontitis. J Periodont Res 44: 133–140.
- Desvarieux M, Schwahn C, Volzke H, Demmer RT, Ludemann J, et al. (2004) Gender Differences in the Relationship Between Periodontal Disease, Tooth Loss, and Atherosclerosis. Stroke 35: 2029–2035.
- Persson GR, Persson RE, Hollender LG, Kiyak HA (2004) The impact of ethnicity, gender, and marital status on periodontal and systemic health of older subjects in the trials to enhance elders‘ teeth and oral health (teeth). J Periodontol 75: 817–823.
- Reichert S, Stein J, Gautsch A, Schaller H, Machulla HKG (2002) Gender differences in HLA phenotype frequencies found in German patients with generalized aggressive periodontitis and chronic periodontitis. Oral Microbiology & Immunology 17: 360–368.
- Shiau HJ, Reynolds MA (2010) Sex differences in destructive periodontal disease: a systematic review. J Periodontol 81: 1379–1389. [crossref]
- Candore G, Balistreri CR, Colonna-Romano G, Lio D, Listi F, et al. (2010) Gender-related immune-inflammatory factors, age-related diseases, and longevity. Rejuvenation Research 2010: 13.
- Renk CM, Wilson J (2005) Comparison of age and gender differences in the prevalence of oral pathogens in subjects with periodontitis.
- Wasterlain SN (2012) Sex differences in periodontal disease and caries in a Portuguese identified skeletal sample from the late nineteenth and early twentieth centuries. Am J Phys Anthropol 147: 297–298.
- Borell LN, Talih M (2012) Examining periodontal disease disparities among U.S. adults 20 years of age and older: NHANES III (1988–1994) and NHANES 1999–2004. Public Health Rep 127: 497–506.
- Buchwald S, Kocher T, Biffar R, Harb A, Holtfreter B, et al. (2013) Tooth loss and periodontitis by socio-economic status and inflammation in a longitudinal population-based study. J Clin Periodontol 40: 203–211.
- Rivas-Tumanyan S, Campos M, Zevallos JC, Joshipura KJ (2013) Periodontal disease, hypertension, and blood pressure among older adults in puerto rico. J Periodontol 84: 203–211.
- Hart TC, Marazita ML, Lake KS, Diehl SR, Schenkein HA (1991) Sex Ratio among Individuals with Juvenile Periodontitis Jp S: 555.
- Sewón LA, Parvinen TH, Sinisalo TV, Larmas MA, Alanen PJ (1988) Dental status of adults with and without periodontitis. J Periodontol 59: 595–598. [crossref]
- Melvin WL, Sandifer JB, Gray JL (1991) The prevalence and sex ratio of juvenile periodontitis in a young racially mixed population. J Periodontol 62: 330–334.
- Haisman-Welsh RJ, Thomson WM (2012) Changes in periodontitis prevalence over two decades in New Zealand: evidence from the 1988 and 2009 national surveys. N Z Dent J 108: 134–138. [crossref]
- Hørmand J, Frandsen A (1979) Juvenile periodontitis. Localization of bone loss in relation to age, sex, and teeth. J Clin Periodontol 6: 407–416. [crossref]
- Slots J, Feik D, Rams TE (1990) Age and sex relationships of superinfecting microorganisms in periodontitis patients. Oral Microbiology & Immunology 5: 305–308.
- Mattson JS, Cerutis DR, Parrish LC (2002) Osteoporosis: a review and its dental implications. Compendium of continuing education in dentistry (Jamesburg, N.J.: 1995) 23: 1001–1004.
- Zerfowski M, Koch MJ, Niekusch U, Staehle HJ (1997) Caries prevalence and treatment needs of 7- to 10-year-old schoolchildren in southwestern Germany. Community Dentistry & Oral Epidemiology 25: 348–351.
- Lundegren N1, Axtelius B, Akerman S (2012) Oral health in the adult population of Skåne, Sweden: a clinical study. Acta Odontol Scand 70: 511–519. [crossref]
- Wang X, Willing M C, Marazita M L, Wendell S, Warren J J, Broffitt B, et al. Genetic and Environmental Factors Associated with Dental Caries in Children: The Iowa Fluoride Study. Caries Res.2012; 46: 177–184.
- Fisher E, Divaris K, Shugars D, White R (2012) Risk factors for third molar occlusal caries: A longitudinal clinical investigation. Journal of Oral and Maxillofacial Surgery.Conference: 94th Annual Meeting Scientific Sessions and Exhibition of the American Association of Oral and Maxillofacial Surgeons, AAOMS 2012 San Diego, CA United States.Conference Start: 20120910 Confer(truncated).,70: e-38.
- Dawkins E, Michimi A, Ellis-Griffith G, Peterson T, Carter D, et al. (2013) Dental caries among children visiting a mobile dental clinic in South Central Kentucky: a pooled cross-sectional study. BMC Oral Health 13: 19.
- Wang JD, Chen X, Frencken J, Du MQ, Chen Z (2012) Dental caries and first permanent molar pit and fissure morphology in 7- to 8-year-old children in Wuhan, China. International Journal of Oral Science 4: 157–160.
- Arantes R, Santos RV, Frazao P, Coimbra CE Jr (2009) Caries, gender and socio-economic change in the Xavante Indians from Central Brazil. Ann Hum Biol 36: 162–175. [crossref]
- Haugejorden O (1996) Using the DMF gender difference to assess the „major“ role of fluoride toothpastes in the caries decline in industrialized countries: A meta-analysis. Community Dentistry & Oral Epidemiology 24: 369–375.
- Heyduck C, Meller C, Schwahn C, Splieth CH (2006) Effectiveness of sealants in adolescents with high and low caries experience. Caries Res 40: 375–381. [crossref]
- Lukacs JR (2011) Gender differences in oral health in South Asia: Metadata imply multifactorial biological and cultural causes. Am J Hum Biol 23: 398–411.
- Lukacs JR (2012) Meta-analyses reveal direction and timing of sex and gender differences in oral health. American Journal of Physical Anthropology.Conference: 81st Annual Meeting of the American Association of Physical Anthropologists Portland, OR United States.Conference Start: 20120411 Conference End: 20120414.Conference Publication: (var.pagings). 2012; 147: 197.
- Lukacs JR (2010) Sex differences in dental caries experience: clinical evidence and complex etiology. Clinical Oral Investig 15: 649–656.
- Mantonanaki M, Koletsi-Kounari H, Mamai-Homata E, Papaioannou W (2013) Prevalence of dental caries in 5-year-old Greek children and the use of dental services: evaluation of socioeconomic, behavioural factors and living conditions. Int Dent J 63: 72–79.
- Pechenkina E, Fan W, Ma X (2012) Male-female oral health differences in early Chinese communities. Am J Phys Anthropol 147: 235.
- Pereira C, Veiga N, Chaves C, Nelas P, Amaral O, et al. (2013) Dental caries and oral health behaviours in a portuguese sample of adolescents. Am J Epidemiol 177: 37.
- Lee HY, Choi YH, Park HW, Lee SG (2012) Changing patterns in the association between regional socio-economic context and dental caries experience according to gender and age: a multilevel study in Korean adults. International Journal of Health Geographics [Electronic Resource] 11: 30.
- Unell L, Soderfeldt B, Halling A, Birkhed D (1999) Explanatory models for clinically determined and symptom-reported caries indicators in an adult population. Acta Odontol Scand 57: 132–138.
- Witt-Pawlowski K (2002) [Oral care indices (API, SBI) in young participants of a caries prophylaxis program.]. Roczniki Pomorskiej Akademii Medycznej w Szczecinie 48: 381–393.
- Wyne AH, Al-Ghannam NA, Al-Shammery AR, Khan NB (2002) Caries prevalence, severity and pattern in pre-school children. Saudi Me.J 23: 580–584.
- Ferracane J, Hilton T, Korpak A, Gillette J, McIntyre PS, et al, (2011) Northwest P R E C E D E N T. Use of caries prevention services in the Northwest PRECEDENT dental network. Community Dent Oral Epidemiol 39: 69–78.
- Masood M, Yusof N, Hassan MI, Jaafar N (2012) Assessment of dental caries predictors in 6-year-old school children – results from 5-year retrospective cohort study. BMC Public Health 12: 989.
- Matulaitiene ZK, Zemaitiene M, Zemgulyte S, Milciuviene S (2012) Changes in dental caries and oral hygiene among 7–8 year-old schoolchildren in different regions of Lithuania 1983–2009. Stomatologija / issued by public institution “Odontologijos studija” …[et al.] 14: 53–59.
- Khare V, Koshy A, Rani P, Srilatha S, Kapse SC, et al. (2012) Prevalence of dental caries and treatment needs among the orphan children and adolescents of Udaipur district, Rajasthan, India. Journal of Contemporary Dental Practice [Electronic Resource] 13: 182–187.
- Stephenson J (2012) A model for the analysis of caries occurrence in primary molar tooth surfaces. Caries Res 46: 452–459. [crossref]