Abstract
Facial paralysis has many etiologies, the most frequent is the idiopathic cause, which is a diagnosis of elimination, then infectious, traumatic, and tumoral causes, dominated by the parotid tumor. Breast cancer rarely gives a perineural metastasis, estimated at 0.6%, of all secondary localizations, with a suggestive clinical presentation, especially the slow and progressive mode of appearance, the involvement of multiple cranial nerves, recurrent paresis, and a history of cancer. Perineural metastases of breast cancer are rare, but can occur, and this case demonstrates that any symptomatology in the patient with breast cancer must be considered in the overall context.
Keywords
Breast cancer, Facial nerve, Perineural metastasis
Introduction
Breast cancer is the leading cause of cancer death in women. The main metastatic sites are bone, lung, liver, brain and lymph nodes. Perineural metastases are extremely rare [1-3].
Observation
A 62-year-old woman, who was treated 10 years ago for invasive bifocal ductal carcinoma of the right breast, by mastectomy with lymph node dissection and chemotherapy. She reported a progressive and painless left facial deviation, with paresthesia of the lower extremities for 3 months. A brain scan with PDC injection showing nodular enhanced in the left cerebellopontine angle. A complementary cerebro-medullary magnetic resonance imaging showed bilateral micronodular thickening of the facial nerve and nodular thickening of the left trigeminal nerve, without any spinal cord abnormality, suggesting secondary localizations of breast carcinoma (Figures 1-3).
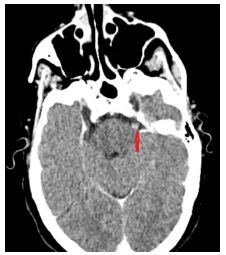
Figure 1: Brain scan with injection of PDC, axial section showing a centimetric nodular lesion in the prepontine cistern on the trajectory of the left trigeminal nerve.
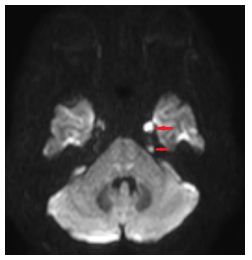
Figure 2: Axial section of the brain MRI, diffusion sequence, showing a nodular perineural hypersignal of the left cranial nerves (V and VI).
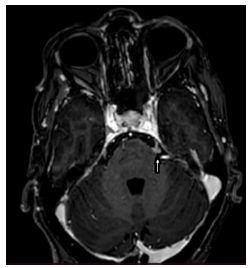
Figure 3: Brain MRI T1 enhanced, axial section, showing nodular contrast of the left trigeminal nerve.
Discussion
There are many etiologies of facial paralysis, the most common is idiopathic etiology, that is diagnosis of exclusion, followed by infectious, traumatic, and neoplastic etiologies, mainly parotid gland tumors. Breast cancer rarely causes neuronal metastases, estimated at 0.6%, and has an impressive clinical presentation, particularly slow and progressive onset, polycranial onset, recurrent paralysis, and a history of cancer.
Conclusion
Perineural metastases of breast cancer are rare but can occur, and the present case demonstrates that any chronic symptomatology in the breast cancer patient must be analyzed in the overall medical context.
References
- Gasperini J, Black E, Van Stavern G (2007) Perineural metastasis of breast cancer treated with optic nerve sheath fenestration. Ophtalmique Plast Reconstr Surg 23: 331-3. [crossref]
- Raghavan P, Mukherjee S, Phillips CD (2009) Imaging of the facial Neuroimaging Clin N Am 19: 407-425. [crossref]
- Delattre JY, Krol G, Thaler HT, Posner JB (1988) Distribution of brain metastases. Arch Neurol 45: 741-4. [crossref]