Abstract
Objective: To know the degree of fulfilment of the treatment goals for DM2 patients.
Methods: Adult DM2 patients. Descriptive, observational and transversal design. Study variables: Process: % of patients with determination of BMI, abdominal perimeter, foot exploration, arterial pressure, EKG, ophthalmoscopy and HbA1c, lipid profile, microalbuminuria, glomerular filtration rate. Intermediate results: % of patients with overweight/obesity, active smokers, HbA1c value <7%, blood pressure <140/90, normal lipid profile, negative microalbuminuria. Final results: % of patients with foot ulcers, amputation, diabetic retinopathy, renal failure, coronary disease, cerebrovascular disease, peripheral arteriopathy and acute complications.
Results: The study include 1,029 DM patients 55% male, mean age 67 ± 0.8 years old. The % of patients with overweight, obesity, hypertension, dyslipemia, were 32.5%, 59.4%, 63.8%, and 64% respectively. The 94% have HbA1c determination, 47% ophthalmoscopy, while only 2.2% foot examination. The percent of patients with <HbA1c, blood pressure <140/90, normal lipid profile, and active smokers were 72.6%, 54.5%, 50% and 26% respectively. While 11.5%, 5%, 3.5%, 2.1% and 8.6% had cardiovascular disease, ictus, peripheral arteriopathy, foot ulcers and renal failure respectively.
Conclusions: The present study shows that in the primary care centers in northwestern Spain, a high percent of patients had good metabolic control and almost all the objectives of the treatment for patients with DM2 are met except the examination of the feet. Actions need to be promoted in order to meet the mentioned objective, including recording educational activities.
Keywords
Type 2 diabetes, Primary care centers, Compliance therapeutic objectives
Introduction
Type 2 diabetes mellitus (T2DM) is a chronic and progressive disease with high prevalence in the general population worldwide. In Spain, the Di@bet.es study [1] estimated the prevalence of DM at around 13.8% in the adult population, with 43.5% of cases not known. DM2 is associated with high morbidity and mortality due to associated vascular disease, both microvascular (retinopathy, nephropathy and neuropathy) and macrovascular disease (cerebral stroke, peripheral arthropathy and ischemic heart disease) [2]. Several years before the diagnosis of T2DM, there is already endothelial dysfunction, insulin-resistance and hyperinsulinemia in patients with DM2, factors that accelerate atherogenesis [3,4]. Therefore, since the main cause of mortality in patients with T2DM is cardiovascular disease, many clinicians think that T2DM is a cardiovascular disease [5]. In addition, T2DM is associated with factors that increase the risk of cardiovascular disease such as obesity, hypertension and dyslipidemia [6]. The UKPDS study showed that intensive glycemic control in people with type 2 diabetes reduced the incidence of microvascular disease, but macrovascular disease did not [7]. For all the above, patients with DM2 in addition to glycemic control require treatment of other cardiovascular risk factors. Several studies in Spain have observed a high percentage of patients with DM2 with poor glycemic control [8,9]. Previous studies have shown that the prevalence of cardiovascular risk factors is higher in long-term patients compared to newly diagnosed patients [10] and that their control was insufficient [11]. More recent studies show that this situation persists [12] or shows slight improvement [13].
The objective of this research was to know the degree of compliance with the treatment objectives of patients with DM2 treated in primary care centers in Northwestern Spain, with special emphasis on the degree of metabolic control and classic cardiovascular risk factors or comorbidities.
Subjects and Methods
The present is a cross-sectional descriptive observational study, which includes a randomized sample of patients with DM2, treated and followed by Primary Care (PC) physicians from the health area of Vigo, territory of southern Galicia, autonomous community of northwestern Spain.
The population of the Vigo Health Area, according to the Municipal Register of Inhabitants of January 1, 2017, was 608,841 inhabitants, of which 48.3% were men and 51.7% women. Of these, 511,724 were over the age of 18. In the computerized registry of the health area, Electronic Medical Record of Galicia (IANUS), there were 41,450 patients with DM2 over 18 years of age. Therefore, the target population includes the aforementioned 41,210 that met the inclusion criteria: Reside in the Vigo area, at least 12 months before the start date of the study, be over 18 years old, be type 2 diabetics receiving antidiabetic treatment. 240 were excluded from the study because they had some exclusion criteria: Patients with diabetes 2 who have not attended their nursing doctor in the last year. Immobilized or bedridden patients. Terminal patients (metastatic cancer, terminal heart failure, highly advanced COPD). Advanced dementias.
Sampling and Calculation of Sample Size
We want to estimate the prevalence of good control of diabetes mellitus and set up a cohort for monitoring micro- and macro-vascular events. With an estimated number of people with diabetes in the Vigo Area of 41,000, for an event ratio of 20%, and with an error of ±3% in the estimation and a confidence level of 95% (alpha=0.05), the necessary number of subjects to study was 672. Estimating data losses of 15% of the total, 773 patients would have to be selected. From the database of Electronic Medical History of Galicia (IANUS) a list was prepared, which included patients who included the episode or clinical problem of diabetes or who had prescribed an antidiabetic drug.
Once the list was cleaned, the sample of patients was randomly selected with replacement.
Study Variables
The study aims to obtain information on the different aspects of the follow-up and control of patients with type 2 diabetes in Primary Care:
Variables of Process
Body Mass Index (BMI) assessment in the last year. Assessment of the Abdominal Perimeter (BP) in the last year. Existence of two determinations of glycohemoglobin (Hb1Ac) in the last year. Performing an electrocardiogram (ECG) in the last year. Measurement of blood pressure in the last year. Measurement of blood pressure in the last year. Realization of a lipid profile in the last year. Determination of glomerular filtration rate and microalbuminuria in the last year. Existence of an eye fundus or ophthalmologist consultation in the last 2 years. Diabetic foot assessment in the last year. % correctly vaccinated against influenza and pneumococcus.
Intermediate Variable
Percentage of patients with obesity or overweight (BMI > 25 Kg/m2). Percentage of patients Smokers in the last year, percentages of patients with adequate HbA1c levels (HbA1c <7%), percentage of patients with controlled blood pressure in the last year (Blood Pressure ≤140/90), percentage of patients with good lipid control in the last year (LDL<100), percentage of patients with normal glomerular filtration rate (>60 mi/min) in the last year. Percentage of patients with negative microalbuminuria in the past year.
Final Outcome
Percentage of patients with foot ulcers, amputees, diabetic retinopathy, renal failure, coronary heart disease, cerebrovascular disease, peripheral artery disease, or acute complications (hospitalizations for hypoglycemia or hyperosmolar coma).
Statistical Analysis
For the analysis of the data, the statistical package SPSS v19.0 (SPSS, Chicago, IL) and the Epidat v4.2 package were used. Initially, a descriptive analysis of all the variables recorded in the study was performed. The numerical variables will be described by mean and standard deviation if they have normal or median distribution and quartile deviation if they do not. Categorical variables will be described by absolute frequency and percentage.
The numerical variables will be compared using the t-student test or the non-parametric Mann-Whitney U test. Categorical variables were compared using the chi-square test or Fisher’s exact test. Multivariate binary logistic regression analysis was performed to describe the variables associated with good diabetes control, establishing this as a dichotomous variable.
Ethical and Legal Aspects
The study was conducted according to the standards of good practice in research. During the preparation of this study, the fundamental principles of the Declaration of Helsinki and the Oviedo Convention of the Council of Europe on Human Rights and Biomedicine, as well as all existing legislation, were respected. The current legislation was complied with at all times (Law 3/2001, of March 28 -modified by Law 3/2005 of March 7-, regulating informed consent and the rights of patients and Decree 29/2009, of February 5, which regulates the use and access to electronic medical records) and no personal identification data will be included in the data collection notebook (CRD), that will be dissociated, so the analysis will be carried out in a completely anonymized way, the subjects cannot be identified, in accordance with Organic Law 15/1999, of December 13, on the Protection of Personal Data.
Results
The sample of patients studied was 1,029 people with DM2, 55% of who were males, the mean age of the patients was 67± 0.8 years, being significantly higher in women (Table 1). Thirty-two point 5% of the patients were overweight and 59.4% obese. Sixty-three point eight % of patients were hypertensives and 64 % had dyslipidemia, 26% were active smokers and 20% were former smokers (Table 1).
Table 1: Main characteristic of the sample of T2DM patients
|
Sample characteristics |
||
| Number of patients | 1029 | |
| Men (n/%) | 563/55 | P<0.001 |
| Women (n/%) | 466/45 | |
| Age (years) | 67 (±0.8) | |
| Men | 6.4 (±1.0) | P<0.001 |
| Women | 69.0 (±1.1) | |
| HbA1c mean (%) | 6.7 (±0.1) | |
| BMI (kg/m2) | 31.5 (±0.4) | |
| Men (kg/m2) | 31.1 (±0.25) | p: 0.03 |
| Women (kg/m2) | 32.0 (±0.34) | |
| Normal weight (%) | 8.1 | |
| Overweight (%) | 32.5% | |
| Obesity/BMI 30-39 (%) | 54.3% | |
| Morbid obesity/IMC ≥40 (%) | 5.1% | |
| Hypertension (%) | 63.8 (±3.0) | |
| Dyslipidaemia (%) | 64.2 (±3.0) | |
| Total cholesterol (mg/dl) | 183. 0 (±2.6) | |
| LDL-cholesterol (mg/dl) | 105.4 (±2.2) | |
| HDL-chol (mg/dl) | 48,7 (±0,8) | |
| Triglycerides (mg/dl) | 151.0 (±6.3) | |
| Smoking (%) | ||
| Non smoker | 54 (±4.1) | |
| Former smoker | 20 (±2.9) | |
| Smoker | 26 (±4.2) | |
| Ischemic heart disease (%) | 11.5 (±1.9) | |
| Stroke (%) | 5.0 (±1.5) | |
| Peripheral arterial disease (%) | 3.5 (±1.3) | |
| Heart failure (%) | 5.4 (±1.6) | |
| Renal insufficiency (%) | 8,6 (±1,9) | |
| Creatinine (mg/dl) | 0.92 (±0.4) | |
| Glomerular filtration (ml/min) | 79.2 (±1.0) | |
| Alb/Cr urine > 30 mg/gr (%) | 33.8 (±2.9) | |
| Foot ulcer (%) | 2.1 (±0.7) | |
| Cancer (%) | 10.2 (±1.8) | |
| Mental illness (%) | 8.4 (±1.8) | |
| Thyroid disease (%) | 7.1 (±1.7) |
Regarding the process indicators, 94% of the patients had at least 2 HbA1c determinations in their history, while 47% of the patients had undergone ophthalmological examination in the last 2 years, 40.6% had registered body weight control, while the examination of the feet was the indicator of lower compliance in only 2.2% of the patients (Figure 1).
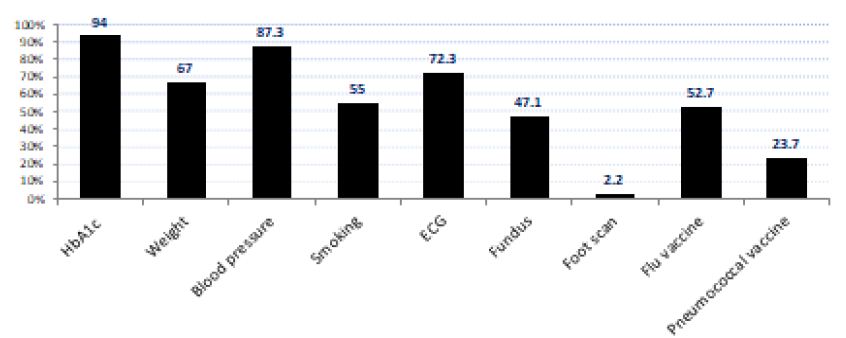
Figure 1: Fulfillment of the process objectives (%)
Regarding the intermediate outcome indicators, 72.6% of patients had mean HbA1c values lower than 7% (Table 2), good blood pressure control 54.5%, with 26% of the sample being active smokers, while good control of dyslipidemia was evident in about 50% of patients (Figure 2).
Table 2: Degree of glycemic control and its relationship with the number of antidiabetic drugs used
|
HbA1c |
||
|
% of patients |
Number of antidiabetic drugs |
|
| < 6.5% | 57.0 (±3.0) | 0.9 ± 0.7 |
| 6.6 -7% | 17.9 (±2.6) | 1.2 ± 0.7 |
| 7.1 – 7.5% | 7.1 (±1.8) | 1.6 ± 1.1 |
| 7.6 – 8% | 5.4 (±1.6) | 1.8 ± 0.8 |
| >8% | 12.6 (±2.4) | 1.8 ± 2.6 |
| P < 0.001 | ||
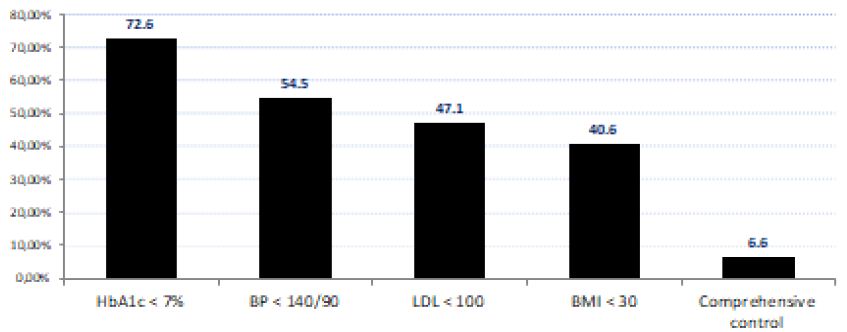
Figure 2: Fulfillment of the intermediate objectives (%)
Most patients had their blood pressure monitored by determining clinical blood pressure (Table 3).
Table 3: Degree of blood pressure control in the whole sample of patients
|
% |
SBP day mmHG |
DBP day mmHG |
SBP night mmHG |
DBP night mmHG |
Good daytime control % |
Good night control % |
|
| ABPM | 8,4 (±1,8) | 138,6 (±4,1) | 83,0 (±2,6) | 125,7 (±4,7) | 72,9 (±3,1) | 52 (±10,3) | 81,2 (±7,1) |
| SMPM | 3,5 (±1,2) | 139,2 (±5,7) | 83,6 (±2,9) | 36,7 (±15,8) | |||
| CBP | 87,3 (±1,9) | 135,6 (±1,1) | 79,2 (±0,7) | 54,5 (±3,2) |
ABPM: Ambulatory blood pressure monitoring, CBP: Clinical blood pressure, DBP: Diastolic blood pressure, SBP: Systolic blood pressure, SMBP: Self-monitoring blood pressure.
Finally, with regard to the final indicators, 11.5% of our patients had ischemic heart disease, 5% stroke, 3.5% peripheral artery disease, foot ulcers in 2.1% and 8.6% renal failure (Table 1).
Another objective of the present study was to know the frequency of the different vascular risk factors. Dyslipidemia and hypertension were the most prevalent factors, 64.2% and 63.8% respectively, followed by obesity in 59% of cases and active smoking in 26.1%. 14% of patients had 3 or 4 CVR factors in addition to diabetes (Table 4).
Table 4: Presence of cardiovascular risk factors (CVRF) in the sample of T2DM patients
|
CVRF |
|
|
% |
|
| Diabetes | 100.0 |
| Hypertension | 63.8 (±3.2) |
| Dyslipidemia | 64.2 (±2.8) |
| Obesity | 59.0 (±3.0) |
| Smoking | 26.1 (±3.9) |
| Diabetes + | |
| 1 CVRF | 34.8 (±3.2) |
| 2 CVRF | 37.6 (±2.4) |
| 3 CVRF | 13.0 (±2.0) |
| 4 CVRF | 1.0 (±0.8) |
Discussion
In the present observational, descriptive and cross-sectional study, a representative sample of patients with DM2 treated in the health area of northwestern Spain was obtained through the random selection of patients with DM2, these data being similar to those found in previous studies in our country [9-13]. The objectives of the study were to know the main socio-demographic and clinical characteristics of patients with type 2 diabetes mellitus (DM2), as well as to obtain information on the degree of compliance with the parameters of the treatment protocol and follow-up of patients attended in primary care centers in the health area of Vigo, with special emphasis on the degree of metabolic control and classic cardiovascular risk factors or comorbidities.
The pillars in the treatment and prevention of comorbidities in patients with T2DM are based on lifestyle changes, pharmacotherapy and education. The available evidence suggests that intensive treatment, mainly from the moment of diagnosis, is effective in preventing microangiopathic complications and cardiovascular events [14].
The variables analyzed in this study are the indicators of quality of care in diabetes mellitus recommended by the Network of Diabetes Study Groups in Primary Health Care (redGDPS) [15], based on the Declaration of Saint Vincent [16]. The comparison with previous studies carried out in our country showed greater compliance with respect to HbA1c measurements, similar results on eye fundus examination, and lower compliance with weight control, and especially with systematic examination of the feet [11,15,17-19]. As the authors of the guide of the GDPS network point out, the indicators are not a direct measure of quality, but allow to detect problems that require an in-depth analysis, in this case the reason for the low compliance of the foot scan.
Compared to the aforementioned studies [15,17-19], there was a clear improvement in glycemic control, while hypertension control was slightly lower, and control of dyslipidemia and smoking habits frankly improvable. Only 6.6% of our patients had a correct comprehensive control, which included glycemic control and the rest of CVRF. In this sense, it should be noted that 72.4% of patients had 1 or 2 associated cardiovascular risk factors and only 14% 3 or more risk factors.
The frequency of macrovascular and microvascular complications was similar to that of previous studies, with less frequent ulcerated lesions on the feet.
The frequency of dyslipidemia and hypertension was lower than that observed in two recent studies conducted in Catalonia and Cantabria health areas in Spain [20,21]. While the frequency of obesity and smoking habit was higher [11,20,21]. The results indicate some improvement, but still far from desirable for our patients. A factor that may condition the comparability of different studies is the fact that the frequency of risk factors depends on the time of evolution of diabetes [10].
The main limitation of the present research is that the study is cross-sectional and we cannot analyze the evolution of the degree of compliance with the treatment objectives in the same sample of patients, however, since the selection of patients has followed a rigorous selection process, it makes the sample representative of the patients seen in our Primary Care Centers, and the review of the history represents an audit of our work, which allows us to draw conclusions about the aspects that we must improve.
In conclusion, our study shows that in the health area of Vigo, a high percentage of patients have good metabolic control and generally meet the treatment objectives, But with regard to the continuous improvement of the quality of the care process, in the section on process indicators, specifically the annual examination of the feet, it is necessary to introduce actions that improve this parameter, as well as the registration of educational interventions and achieve a decrease in the percentage of patients with obesity and active smokers.
References
- Soriguer F, Goday A, Bosh-Comas A, Bordiu E, Calle-Pascual A, et al. (2022) Prevalence of diabetes mellitus and impaired glucose regulation in Spain. The Dia@bet.es Study. Diabetologia 55: 88-93. [crossref]
- Kannel WB, McGee DL (1979) Diabetes and cardivascular disease- The Framinghan study. JAMA 241: 2035-2038. [crossref]
- Hedblad B, Nilsson P, Janzon L, Bergland G (2000) Relationship between insulin resistance and carotid intima media thickness and stenosis in non diabetic subjects. Results from a cross sectional study in Malmo, Sweden. Diabetic Med 17: 299-307. [crossref]
- Beck-Nielsen H, Groop LC (1994) Metabolic and genetic characterization of prediabetes states. Sequence of events leading to non-insulin-dependent diabetes mellitus. J Clin Invest 94: 1714-1721. [crossref]
- Haffner SM, Letho S, Rönnemaa T, Pyörala K, Laaskso M (1998) Mortality from coronary heart disease in subjects with type 2 diabetes and in non-diabetic subjects with and without prior myocardial infarction. N Eng J Med 33: 229-234. [crossref]
- De Fronzo R, Ferranini E (1991) Insulin resistance. A multifaceted syndrome responsible for NIDDM, obesity, hypertension, dislipemia and atherosclerotic cardiovascular disease. Diabetes Care 14: 173-194. [crossref]
- UK Prospective Diabetes Study (UKPDS) Group (1998) Intensive blood glucose control with suphonilureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 352: 837-853. [crossref]
- Mata-Cases M, Benito-Badorrey B, Roura Olmeda P, Coll de Tuero C, Pepio-Vilarubí JM, et al. (2010) Fifteen years of improvement in process and outcome indicators in the management of type 2 diabetes mellitus in primary care centers in Catalonia, Spain. Diabetologia 53: 407 S. [crossref]
- De Pablos P, Franch J, Banegas JR, Fernández Anaya S, Sierras Mainard A, et al. (2009) Estudio epidemiológico del perfil clínico y control glucémico del pacientes diabético atendido en centros de atención primaria en España (estudio EPIDIAP). Endocrinol Nutr 56: 233-240.
- García-Mayor RV, Benito P, Faure E, Pallardo LF, Puig-Domingo M, et al. (2003) Cardiovascular risk factors in type 2 diabetic patients in Spain. Av Diabetol 19: 161-165.
- Benito López P, García-Mayor RV, Puig-Domingo M, Mesa Menteca J, Pallardo Sánchez LF, et al. (2004) Perfil de los pacientes con diabetes mellitus tipo 2, en la atención primaria españ Rev Clin Esp 204: 18-24.
- Vázquez LA, Rodríguez A, Salvador J, Ascaso JF, Petto H, et al. (2014) Relationships between obesity, glycemic control, and cardiovascular risk factors: a pooled analysis of cross-sectional data from Spanish patients with type 2 diabetes in the proinsulin stage. BMC Cardiovas Dis 14: 153-160. [crossref]
- Vinagre I, Mata-Cases M, Hermosilla E, Morros R, Fina F, et al. (2012) Control of glycemia and cardiovascular risk factors in patients with type 2 diabetes in Primary Care in Catalonia (Spain). Diabetes Care 774-779. [crossref]
- Patel A, MacMahon S, et al. (2008) ADVANCE Collaborative Group, Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 358: 2560-2570. [crossref]
- Franch J, Artola S, Díez J, Mata M, redGDPS (2010) Evolución de los indicadores de calidad asistencial al diabético tipo 2 en Atención primaria (1996-2007). Programa de mejora continua de calidad de la Red de Grupos de Estudio de la Diabetes en Atención Primaria de la Salud. Med Clin (Barc) 135: 600-607.
- Krans HMJ, Porta M, Keen H (1992) Diabetes Care and Research in Europe. The Saint Vincent Declaration Action Programme. Ginebra: WHO Regional office for Europe.
- ELIPSE (2005) Efectividad en el control de factores de riesgo cardiovascular en diabéticos tipo 2 de la provincia de Ciudad Real. Rev Clin Esp 2005: 218-222. [crossref]
- De la Calle H, Costa A, Diez-Espiño J, Franch J, Goday A (2003) Evaluación del cumplimiento de los objetivos de control metabólico de la diabetes mellitus tipo 2. Esudio TransSTAR. Med Clin (Barc) 120: 446-450.
- Orozco-Beltrán D, Gil Guillen VG, Quirce F, Navarro-Pérez J, Pineda M, et al. (2007) Collaborative Diabetes Study investigators. Control of diabetes and cardiovascular risk factors in patients with type 2 diabetes in primary care. The gap between guidelines and reality in Spain. Int J Clin Pract 61: 909-915. [crossref]
- Díaz Vera AS, Abellán Alemán J, Segura Fragoso A, Martínez de Esteban JP, Lameiro Couso FJ, et al. (2020) Prevalencia y factroes de riesgo asociados a la dislipidemia en pacientes diabéticos tipo 2 de la Comunidad de Cantabria. Endocrinol Diabetes Nutr 67: 102-112.
- Mata-Cases M, Franch Nadal J, Real J, Cedenillo M, Mauricio D (2019) Prevalence and coprevalence of chronic comorbid conditions in patients with type 2 diabetes in Catalonia: a population-based cross-sectional study. BMJ Open 9: e031281. [crossref]