DOI: 10.31038/CST.2023831
Abstract
Prostate cancer is a cancer of the elderly: it rarely appears before the age of 50, and the incidence increases very rapidly with age. Age is the main risk factor identified for prostate cancer. This risk is 1% to 7% between 50 and 64 years of age, and rises from 14% to 26% between 65 and 74 years of age. These risks increase by 40% between the ages of 75 and 79 and reach 50% at the age of 80. The most common problems are: prostatitis or inflammation of the prostate, urinary urgency, urinary frequency, dysuria, acute retention of urine, or more rarely, initial hematuria. The objective of this study was to describe the epidemiological, clinical and histological aspects of prostate cancer in the Thiès region. Our study was conducted between January 2020 and December 2022 with a population of 165 patients with prostate cancer in the urology department of the regional hospital of Thiès and the Saint Jean de Dieu hospital of Thiès. The variables studied were age, PSA levels, Gleason score and histological grades. The mean age of the patients was 71.18 years with extremes ranging from 47 years to 90 years, and the mean PSA level was 965.33 ng/ml with extremes from 5 ng/ml to 5000 ng/ml. Our results show that 87% of our patients were older than 65 years. Gleason score 7 (4+3) was more represented with a rate of 37% corresponding to grade III according to WHO-ISUP 2016. The incidence is in average decline between 2020 and 2022.
Keywords
Prostate, Cancer, Epidemiology, Senegal
Introduction
In 2020, according to the World Health Organization (WHO), prostate cancer is the third most common diagnosed malignancy. With 1,414,259 cases (7.3% of the total), prostate cancer is preceded only by lung and colorectal cancer with 2,206,771 and 1,148,515 cases (11.4 and 10.0%), respectively [1]. It is the most commonly diagnosed cancer in more than 50% of the world’s countries (112 out of 185) and its incidence varies considerably between high and low human development index (HDI) countries, 37.5 versus 11.3 per 100,000 population respectively. Mortality rates are less variable (8.1 vs. 5.9 per 100,000 people). respectively. Mortality rates are less variable (8.1 vs. 5.9 per 100,000 people). Despite the significant burden of prostate cancer, established risk factors for this malignancy are limited to age, ethnicity, and a positive family history of the disease [2,3]. In fact, cancer incidence and mortality rates are strongly associated with increasing age, with a mean age at diagnosis of 66 years [4]. They also vary considerably by region and population, with higher rates among men of African descent and lower rates among those of Asian descent [3,5,6]. Epidemiological studies have also found that first-degree relatives of a patient with prostate cancer have two to three-fold increased risk of developing the disease compared to the general population, and the risk further increases with the number of affected relatives [7]. The aim of this prospective study was to investigate the clinical and histological characteristics of prostate cancer in the Thies region.
Material and Methods
This is a prospective descriptive study including 165 patients with prostate cancer. These patients were recruited from the urology department of the Thiès regional hospital and the Saint Jean de Dieu hospital in Thiès between January 2020 and December 2022. Inclusion criteria were a suspicious digital rectal exam with a PSA level above 4 ng/ml, then biopsies were performed for histopathological diagnosis. All histologically confirmed malignant prostate tumors were included in this study. Data were collected by consulting the hospitalization records, which are kept in the archives on a pre-established sheet, we collected in current family records the demographic data (name, surname, age, ethnicity, reason for consultation) and medical history. Data entry and analyses were performed using Microsoft Office Excel.
Results
Our epidemiological survey was conducted in a regional population of one hundred and sixtyfive (165) prostate cancer patients from January 2020 to December 2022. The mean age was 71.18 years with extremes ranging from 47 years to 90 years, and the mean PSA level was 965.33 ng/ml with extremes from 5 ng/ml to 5000 ng/ml. Only 16.36% of patients were less than or equal to 65 years of age (27/165). 82% of the patients were between 60 and 80 years of age and 11.5% were older than 80 years (Figure 1). In this study, the most common reasons for consultation were: urinary urgency, urinary frequency, dysuria, acute retention of urine, or more rarely, initial hematuria. The incidence of prostate cancer decreased with the years with 67 cases in 2020, 55 in 2021 and 47 cases in 2022 (Figure 2).
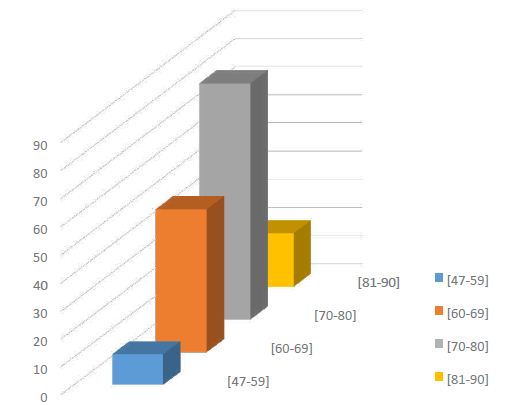
Figure 1: Distribution of patients by age group
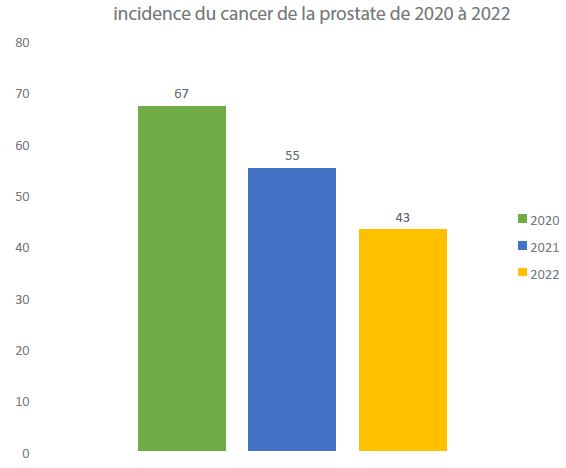
Figure 2: Incidence of prostate cancer from 2020 to 2022
When examining histopathologic differentiation, patients with Gleason score 7 (4+3) prostate adenocarcinoma were more represented with a total of 61 individuals out of 165. According to WHO-ISUP 2016 grade, grade III was more frequent with 37% of cases, followed by grade IV with a frequency of 27%; only 2% of cases were grade V (Figure 3).
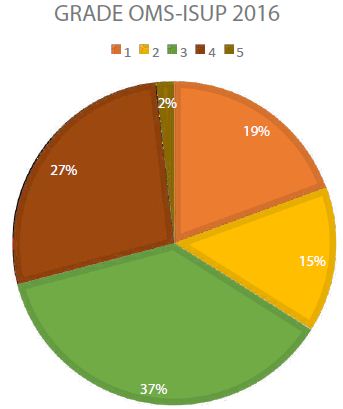
Figure 3: Distribution of patients by WHO-ISUP Grade 2016
Discussion
We recruited 165 patients newly diagnosed with prostate cancer. These cases of prostate cancer, which made it possible to study the epidemiological and histopathological aspects of these cancers in Thiès, could not be considered as the totality of prostate cancers at the regional level because only anatomopathological specimens received in the laboratory were considered. The mean age of the patients was 71.18 years, comparable to those reported in the African literature, particularly that observed in Senegal by Gueye et al. and in Congo-Brazzaville by Peko et al. which is 69 years [8,9]. In the statistical studies of Amégbor et al. and Brawley et al. the average age of onset of prostate cancer is respectively 70 and 71 years [10,11]. In our study, the age range between 60 and 80 years was more represented with a frequency of 82%, this age range is found in Amegbor et al. and Ndoye et al. [12]. All these data confirm that prostate cancer is a disease of the elderly. According to Boyle, it is the most frequent cancer in men over 50 years old [13].
Moreover, the frequency of prostate cancer increases with age [14]. In our study 84% of the patients were older than 65 years. In addition, the low incidence rate in men under 50 years of age (0.06%) provided further evidence that the prevalence of prostate cancer is closely related to the increasing age of the patients [15,16]. The average age at diagnosis was high, hence the presence of these very advanced forms beyond any therapeutic resources. The delay in diagnosis is related to the natural history of prostate cancer but also to the apprehension that men had to come to the urologist. In addition, there is a lack of information and awarenessraising policy for the population about this condition, and difficulties in accessing health services. Contrary to the work carried out in the West where the average PSA level oscillates between 15 and 25 ng/ml [17], we note an elevation of the PSA level with an average PSA of 965.33 ng/ml, which is in line with the results of Nzamba et al. in Ivory Coast [18]. This PSA profile is consistent with the litterature, as several studies have reported a higher PSA level in African Americans than in Caucasian Americans [19-21]. This high PSA value could indicate early metastatic extension. In this study, Gleason score 7 (4+3) was the most represented with 61 out of 165 cases or 37%. This result is different from that of Jalloh et al. [22] and Amégbor et al. who found score 6 with a rate of 52% and 60% of cases. The patients in our study present a high proportion of advanced stage tumors (stage III and stage IV), i.e. 64% of cases; these results are matched with those of Gueye et al. and Benseba et al. in Algeria [23]. Only 2% of patients are stage V, these results confirm the progress of screening We note in this study population a relatively small decrease in the incidence of diagnosed cancers over the years, from 67 cases in 2020 to 43 cases of cancer in 2022. This relative decrease could be explained by a more targeted screening practice and improved diagnostic tools. Mass screening is not recommended. Early individual diagnosis is based on an annual PSA test associated with digital rectal examination in men between 50 and 75 years of age with a life expectancy of more than 10 years.
Conclusion
Prostate cancer in this study population is characterized by an advanced age at diagnosis that can lead to an advanced tumor grade correlated with a high PSA level and a huge frequency of metastasis.
The results of this study showed a relatively small decrease in the incidence of prostate cancer in the Thiès population for the period from 2020 to 2022. However, the relatively declining incidence in the Thies region indicates the need to optimize methods of timely diagnosis of prostate cancer by focusing on high-risk incidence groups.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A. Statistiques mondiales sur le cancer 2020: Estimations GLOBOCAN de l’incidence et de la mortalité dans le monde pour 36 cancers dans 185 pays. CA: Un Journal Sur le Cancer Pour les Cliniciens. 2021. [crossref]
- Pernar CH, Ebot EM, Wilson KM, Mucci, LA. The Epidemiology of Prostate Cancer. [crossref]
- Cold Spring Harb Perspect Med 2018;8: a030361
- Taitt, HE Tendances mondiales et cancer de la prostate: examen de l’incidence, de la détection et de la mortalité en fonction de la race, de l’ethnicité et de l’emplacement géographique. Un m. J. Men’s Heal. 2018, 12, 1807-1823.
- Brandt A, Bermejo JL, Sundquist J, Hemminki, K. Âge au diagnostic et âge au décès dans le cancer de la prostate familial. Oncologue. [crossref]
- Rebbeck TR, Devesa SS, Chang, B.-L, Bunker CH, Cheng, JE, Cooney K, Eeles R, Fernandez P, Giri VN, Gueye SM, et coll. Tendances mondiales de l’incidence, de l’agressivité et de la mortalité du cancer de la prostate chez les hommes d’ascendance africaine. Cancer de la prostate. [crossref]
- Odedina FT, Akinremi TO, Chinegwundoh F, Roberts R, Yu D, Rames RR, Freedman ML, Rivières BM, Vert BL, Kumar, N.-B. Disparités du cancer de la prostate chez les hommes noirs d’ascendance africaine: Une revue comparative de la littérature sur le fardeau du cancer de la prostate chez les hommes noirs aux États-Unis, dans les Caraïbes, au Royaume-Uni et en Afrique de l’Ouest. Agents infectieux Cancer. [crossref]
- Carter BS, Bova GS, Beaty TH, Steinberg GD, Childs B, Isaacs WB, Walsh, PC Cancer de la prostate héréditaire: caractéristiques épidémiologiques et cliniques. J Urol. [crossref]
- Gueye SM, Jalloh M, Labou I, Niang L, Kane R, Ndoye M. Profil clinique du cancer de la prostate au Sénégal. Afr J Urol 2004;10: 203-207.
- Peko JF, Bouya P, Kokolo J, Ngolet A. Cancers de la prostate au CHU de Brazzaville: épidémiologie et histopronostic. Med Afr Noire. [crossref]
- Amégbor K, Seddoh T Y, Tengué K, Songne-Gnamkoulamba B, Napo-Koura G, James K. Épidémiologie et histopronostic du cancer de la prostate au Togo: à propos de 202 cas diagnostiqués au laboratoire d’anatomie pathologique du CHU Tokoin de Lomé. Progrès En Urologie. [crossref]
- Brawlay O, Knopf K, Merill R. The epidemiology of prostate cancer, part 1: descriptive epidemiology. Semin Urol Oncol. [crossref]
- Ndoye M, Niang L, Gandaho K, Jalloh M, Labou I, Gueye S et al. (2013) Cancer avancé de la prostate au Sénégal. Aspects diagnostiques à l’hôpital de Grand Yoff. [crossref]
- Boyle P, Maisonneuve P, Napalkof P. Geographical and temporal pattern of incidence and mortality from prostate cancer. Urology. [crossref]
- Meikle AW, Smith JA. Epidemiology of prostate cancer: early detection and treatment of localized carcinoma of the prostate. Urol Clin North Am. [crossref]
- Houston KA, King J, Li J, Jemal A. Trends in prostate cancer incidence rates and prevalence of prostate specific antigen screening by socioeconomic status and regions in the United States, 2004 to 2013. Journal of Urology. [crossref]
- Daniyal M, Siddiqui ZA, Akram M, Asif HM, Sultana S, Khan A. Epidemiology, etiology, diagnosis and treatment of prostate cancer. Asian Pacific Journal of Cancer Prevention. [crossref]
- Hermabessiere J, Taillander J. Physiologie de la prostate. Encycl MedChir (Elsevier, Paris). France, Nephrol Urol. [crossref]
- NZAMBA B, Paul L, ODO B A, NZIENGUI T C, KOUASSI K Konan Y, KAGAMBEGA Zoewendbem A G, TOURE et al., 2020M Cancer de la prostate chez le sujet de race noire en Côte d’Ivoire
- Morgan TO, Jacobsen SJ, McCarthy WF, Jacobson DJ, McLeod DG? Moul JW. Agespecific reference ranges for serum prostate specific antigene in black men. N Eng J Med. [crossref]
- Freedland SJ, Sutter ME, Naitoh J, Dorey F, Csathy GS, Aronson WH. Clinical characteristics in black and white men with prostate cancer in an equal acces medical center. Urology. [crossref]
- Jalloh M, Thiaw G, Bathily EHAL, Dial C, Ndoye M, Diallo A et al. Corrélation entre Score de Gleason biopsique et métastases osseuses à la scintigraphie dans le cancer de la prostate. Revue Africaine d’Urologie et d’Andrologie. [crossref]
- Benseba S, Azem L, Mouaici K et al. (2021) Étude épidémiologique et physiopathologique du cancer de la prostate.