Abstract
Dentine hypersensitivity (DH) appears to be increasing in prevalence over time, both in the UK and across the world. As many of our patients are living longer and retaining their natural dentition later into life, dentine hypersensitivity may become a more pressing challenge for dentists to manage. The management of dentine hypersensitivity can be difficult, and the evidence and advice are developing quickly. This article explores the aetiology of DH on all tooth surfaces and subsequently provides greater detail on abrasion as well as discussing the importance of erosion. There is also a detailed section on Non-Carious Cervical Lesions. Finally, the management of DH is discussed with recommendations for clinical practice.
Introduction
Dentine hypersensitivity (DH) is defined as a “short, sharp, pain arising from exposed dentine in response to stimuli, typically thermal, evaporative, tactile, osmotic or chemical, which cannot be ascribed to any other form of dental defect or pathology” [1] and may influence the Quality of life (QoL) of those who suffer with the problem [2]. The most accepted theory of dentine hypersensitivity is the hydrodynamic theory, whereby on stimulus of exposed dentine, dentine fluid displaces and stimulates the nerves in the odontoblast layer [3] although other mechanisms cannot be ruled out [4]. The reported prevalence of DH in the population is high, with the largest and most recent cross- sectional study of seven European countries demonstrating 75.9% of participants were suffering from dentine hypersensitivity, using the Schiff cold air sensitivity scale [5]. In the UK, the prevalence again remains high, with a study showing DH prevalence at 89 % in 2024 [5]. The Schiff test involves application of a cold stimulus to the tooth and records a score based on the individual patient’s response [5]. ‘The Cumulative Hypersensitivity Index (CHI) has been validated as a method for recording the severity of DH for a patient. It uses the recognised Schiff sensitivity score as a sextant cumulative score and is likened to the method of recording a BEWE or BPE for tooth wear and periodontal screening respectively [6]. Dentine hypersensitivity can profoundly affect quality of life (QoL), with one study demonstrating interference with speaking, eating, social interaction and DH made toothbrushing difficult for a small number of patients [2,7]. There was also a significant emotional impact, with many reporting they felt they could not participate in everyday life as they would wish [2]. This article further expands on the latest aetiologies and management for DH, further to the previous BDJ article in 2017 [8]. Since then, there have been several advances in our understanding of the condition, related terminologies and management strategies. We focus primarily on advances in aetiology, management and the term Non-Carious Cervical Lesions in this article.
Aetiology
Exposure of Dentine
Dentine hypersensitivity occurs sometimes when dentine is exposed. Dentine exposure can be caused by tooth wear, such as erosion, abrasion, and attrition [3], although often it is a combination of these [9]. Abrasion and erosion often work synergistically, with abrasion more likely to occur following erosive attacks [10] There is increasing concern that some toothpastes may be causing abrasion, [10] particularly charcoal toothpastes in recent years [11].
There is also concern regarding erosion following carbonated drink consumption, [12] with a recent study showing that one tenth of University students in the UK were consuming carbonated drinks at least once per day and 30% were consuming them twice per week [13]. Further to this, since the recent Soft Drink Industry levy, consumption of sugar free alternatives, which may still be erosive, has increased by 40% [14].
Gingival recession can also lead to root dentine exposure [15]. The prevalence of recession in the population is high, with a 2023 systematic review and meta-analysis showing an 85% prevalence [16]. Gingival recession can be caused by numerous factors, for example periodontitis [5] and it has been demonstrated that patients with periodontitis are found to be increasingly affected by DH [9]. Furthermore, gingival recession can follow periodontal treatment [17], other clinical studies have also shown that DH is more prevalent in situations with gingival recessional and without gingival inflammation [6].
Trauma from toothbrushing has been suggested to be a cause of gingival recession. Brushing frequency and a horizontal scrubbing method of toothbrushing (inappropriate or overzealous techniques) may create recession, although there is little high-quality evidence to support this [18]. Some para-functional habits can cause exposure of dentine, such as pipe-smoking (9), as can the wearing of both lip and tongue piercings [19] Tooth position, orthodontic movement, high muscle attachments and gingival biotype can also lead to recession [20].
Dentine Tubule Exposure and Signs of Progressive Wear
Evidence suggests that areas of exposed dentine causing dentine hypersensitivity to have more and wider patent dentine tubules and it is now well understood that removal of the smear layer at the surface of dentine leads to the opening of the dentine tubules [21].
The smear layer therefore acts as a protective agent to mask dentine hypersensitivity symptoms by occluding dentinal tubules, with studies suggesting that the smear layer prevents approximately 86% of fluid flow through the dentine tubules [22].
It is postulated that both chemical or mechanical agents may lead to loss of the smear layer, this can include toothbrushing, toothpastes and erosive agents in the diet or intrinsic erosive sources [23]. The presence of DH is an indicator of a possible active or progressive tooth wear issue and more recent acidic episodes have been shown in another novel study to increase the chance of DH the more recently acidic intake is consumed [24]. This study was conducted on incisal/ occlusal surfaces demonstrating DH is not always on buccal or labial cervical tooth surfaces.
Dentine Whitening
Dental bleaching can also cause DH, with studies demonstrating that both hydrogen peroxide and carbamide peroxide can lead to sensitivity [15,25]. The mechanism of this sensitivity however is different, as the peroxide travels quickly through the enamel and dentine, reaching the pulp. Therefore, this can be described as more like symptoms of pulpitis [26]. This may make treatment in these cases more challenging.
Causes
Abrasive Toothpastes
There has been considerable development in toothpastes on the market. Charcoal toothpastes are becoming increasingly common and are now readily available on the Highstreet [27]. A 2022 systematic review of in-vitro studies found that charcoal toothpastes had some of the highest abrasive potential of all whitening treatments and the study concluded that these products are potentially able to damage the hard tissues of the teeth [28]. Interestingly, a study by Franco et al. in 2020 showed that charcoal toothpastes do not have any bleaching properties and are therefore unable to change the intrinsic colour of the dentine [29] consequently the whitening effects of charcoal toothpastes are due to its abrasive properties removing extrinsic staining [28]. Further to this, an in-vitro study demonstrated that there were again limited whitening effects of charcoal toothpastes. However, the study showed that these products do increase surface roughness, which could potentially lead to dentine hypersensitivity if dentine is exposed [30].
In contrast to this, the relative dentine and enamel abrasivity of charcoal toothpastes were like other toothpastes [31]. However, as discussed in the study, RDA/REA is only one of many factors to consider when looking at abrasivity. In addition, a brushing machine was used, which may not replicate exactly how abrasive the toothpaste would be in-vivo [31]. Nonetheless, a similar study, using hand brushing instead of machine brushing on acrylic, found that toothpastes containing charcoal caused a similar amount of abrasion to those without a charcoal abrasive [32]. A study concerning human enamel samples reported that toothpaste with a higher RDA has been shown to have little effect on wear of enamel, although dentine wear increased by a statistically significant amount [33]. However, a 2023 study using bovine enamel reported that wear increased relative to regular toothpaste (containing sodium bicarbonate) for products containing charcoal [34]. The data regarding charcoal toothpastes and its effect on enamel or dentine clearly differs across studies, although it does appear that there is definite potential for these toothpastes to cause damage, particularly to dentine. Some studies are also laboratory based and although helpful, may not always relate to a clinical situation. Considering this and the fact that the aesthetic outcomes of these toothpastes appear poor at best, with the possibility that they may even cause marginal staining of resin composites [35], it would be sensible to advise patients to avoid these products.
Brushing Force
A 2015 laboratory study on human dentine samples, investigated for the first time the effect of brushing force on the patency of dentinal tubules and in-turn the effect brushing force may have on dentine hypersensitivity [36]. It demonstrated that an increased brushing force (400g) leads to a large increase in the number of patent dentine tubules. Importantly, and in contrast, lower brushing forces closer to 100 g had therapeutic effects on the dentine and resulted in the development of a smear layer irrespective of whether a toothpaste was used. Patent dentinal tubules are a prerequisite for dentine hypersensitivity and therefore demonstrated that an over-zealous brushing force could lead to increased sensitivity [36]. Lower brushing forces are not always obtained and the author reported that lower forces of 100g occur when the toothbrush bristles do not bend [36]. It would therefore appear sensible to advise patients not to brush firmly. Anecdotally, many patients believe that a firm brushing style will lead to improved oral hygiene and therefore we should be counselling our patients on this. Perhaps suggesting an electric toothbrush with a pressure sensor is a sensible compromise or suggesting that the toothbrush bristles do not bend on brushing.
Bristle Stiffness
With reference to bristle stiffness, a recent laboratory study using bovine dentine found that with increased brushing force, there is a statistically significant increase in dentine wear. This was concluded for both soft and medium toothbrush bristle stiffness. It was observed that medium-stiffness bristle toothbrushes, do cause an increase in dentine wear, however, this was only at an increased brushing force (4N equivalent to 400g). At lower brushing forces (1N-3N), the wear between the brushes was not statistically significant [37].
Regarding human enamel samples, Turssi et.al reported that medium and hard stiffness bristles caused more wear than softer bristles [38]. However, the toothbrushes used did have different bristle diameters/ number of bristles per tuft, which may have affected the results. Anecdotally, it may also be inferred that due to the diameter of filaments within softer brushes being less, they may by default carry more toothpaste and may in fact bend and contact more the dentine surface.
Bristle Arrangement and Shape
When using human dentine samples, a study observed that the arrangement of the toothbrush bristles and brushing mode can affect the amount of dentine wear [39]. The study investigated the following toothbrushes a) sonic toothbrush, b) oscillating-rotating, c) flat manual brush and d) rippled manual toothbrush. A standard brushing force of 2N and same toothpaste was used. It was observed that the sonic brush produced the most wear, followed by oscillating, then flat manual and rippled manual toothbrushes. It has been surmised that the bristles of the power brush may travel a longer distance over the tooth, thereby increasing the wear. The rippled bristles of the manual brush produced less wear, possibly since less bristles were in contact with the tooth. The increased movement frequency of the sonic brush, together with its wiping movement may apply increased shear forces to the dentine [39]. A 2022 study from the University of Zurich reported that the shape of the bristles can affect the amount of dentine wear. The study used bovine dentine samples and examined both tapered bristles and round ended bristles. It was determined that the round ended bristles caused a statistically significant increase in wear, compared to the tapered bristles. This was the outcome for all brushing forces applied. There is also evidence to suggest that the cleaning efficacy of tapered brushes is an improvement on round ended bristles [40].
Similarly, a study compared the relative dentine abrasivity of toothbrushes with different tuft arrangements – looking specifically at crossed and parallel tufts. It was observed, using bovine dentine samples, that parallel tufts caused significantly more wear. This was the outcome regardless for the slurry abrasivity and bristle stiffness. Soft crossed toothbrushes also caused more wear than the medium crossed toothbrushes [41]. It appears that the data regarding bristle stiffness is conflicting, and that bristle shape, arrangement and mode of brushing all play a part in the aetiology of wear and DH. It is likely impractical to advise patients to buy toothbrushes with specifically shaped bristles as this information is not readily available to the lay consumer. It appears sensible, based on the information we have, to advise patients to avoid using a charcoal dentifrice and make use of a gentle brushing habit (or make use of a pressure sensor). Further, research is needed regarding bristle stiffness.
Brushing Frequency
A study on self-reported DH, indicated that there was no association between both brushing frequency and time spent brushing on the prevalence of DH [42]. However, again based on clinical experience many patients feel compelled to brush their teeth more than twice a day to achieve optimal oral hygiene and they should be advised that this is not necessary.
Erosion – Intrinsic and Extrinsic Sources of Acid
A 2020 systematic review of 53 cohort and cross-sectional studies demonstrated that carbonated drinks, energy drinks and fruit juices are heavily implicated in dental erosion. Furthermore, it was observed that those who had a high intake of carbonated drinks between meals or those who hold drinks in their mouth prior to swallowing, had an increase in the prevalence of erosion. Drinking carbonated/ acidic drinks at bedtime was also reported to be an additional risk factor for erosion [43]. Frequent consumption of dietary acids throughout the day is associated with erosive tooth wear [44].
A 2017 study demonstrated greater self-reported DH in those drinking more than three dietary acids per day, particularly between meals. What was of particular interest was the strong association between habits such as sipping/ swishing dietary acids in the mouth, which was independent of frequency of consumption. This indicated that contact time with dietary acids may be even more vital in the aetiology of DH [42].
The largest European study investigating DH demonstrated a strong link between an erosive diet and dentine hypersensitivity. Patients were clinically assessed for dentine hypersensitivity, and this was cross referenced with a questionnaire detailing erosive acid intake. There was a strong correlation between erosive drinks (isotonic/ energy drinks) and dentine hypersensitivity [45].
Consumption of erosive drinks has been demonstrated to be associated with wear on both the incisal and occlusal surfaces of the teeth. There is a positive relationship between the severity of this wear and the severity of reported DH. In addition, DH was associated with acidic beverage consumption and was more prevalent the less time there had been since the last consumption of such beverages [24]. This is likely due to the effect of recent interruption of the smear layer by erosion.
Gastric reflux is significantly associated with both erosive tooth wear and DH [6]. Often this presents as wear on the palatal surface of the anterior maxillary teeth. Patients with reflux should be advised to seek medical care with their general medical practitioner (GMP). It is important to note that reflux may be silent, and patients may be unaware of their reflux, therefore practitioners should keep this in mind and refer patients to the GMP as necessary [46].
Erosive acids within the diet, particularly acidic drink consumption, leads to erosive tooth wear and subsequent dentine hypersensitivity. Patients must be instructed that these foods/ drinks should be limited in the diet and drunk at mealtimes only.
Non-Carious Cervical Lesions (NCCLs) and Toothwear
NCCLs are tooth wear lesions located at the cervical region of teeth, known as the Cemento Enamel Junction (CEJ), without the presence of caries. They are usually wedge shaped [47]. It has long been suggested that these lesions may be a result of tensile stress in the cervical area, because of occlusal forces [48]. This historically has been termed abfraction, defined as hard tissue loss because of ‘cyclic and non-axial loading of teeth that leads to biomechanical stress’, that is theorized to cause wedge defects at the CEJ [49]. There is a great deal of debate regarding if abfraction is a major cause of tooth wear and if it could therefore be an indirect cause of dentine hypersensitivity. Often studies fail to control for other possible causative factors including toothpaste abrasivity, toothbrushing habits and erosive factors in the diet. Currently there appears to be little clinical evidence that occlusal factors are contributing to NCCL development [50].
A 2012 systematic review demonstrated that there is currently limited high-quality evidence linking occlusal forces with the formation of NCCLs [51]. Many of the studies looking into abfraction have used computer algorithms to analyse these forces, however they do appear to have limitations. Often in these studies the forces are shown to be equally applied lingually [52], however this contradicts the clinical evidence that most of these lesions are observed buccally [53], which is where abrasion from toothbrushing is normally identified by a clinician.
Furthermore, studies have demonstrated that NCCLs can be replicated in a laboratory setting using both abrasive and erosive challenges, without occlusal forces [54]. ‘However, abfraction type lesions have not been replicated in laboratory settings. Interestingly, from an anthropological point of view NCCLs were not prevalent before the introduction of toothbrushing and dentifrice use [55].
It appears that evidence regarding abfraction is limited and the available studies are not able to demonstrate a conclusive link between occlusal forces and NCCLs. Therefore, it remains prudent that both erosion and abrasion contribute to development of NCCL’s, at least early on, and to concentrate preventative advice with our patients around these aetiologies. Figure 1 provides an example of abfraction lesions on multiple teeth, caused by erosion and brushing abrasion. Please note not all teeth are in occlusion.

Figure 1: Non-carious cervical lesions caused by erosion and abrasion.
Management
The most important aspect of management is prevention of aetiologies, as discussed above. There have been numerous suggested treatments to alleviate dentine hypersensitivity. Often these treatments will focus on blocking the neural transmission or act as an occluding agent i.e. blocking the dentine tubules [56]. The latter has allowed better management by focusing on the aetiology i.e. dentine tubule exposure as follows. Figure 2 demonstrates the surface of dentine with dentine tubules occluded and covered following tubule occluding toothpaste application (Table 1).
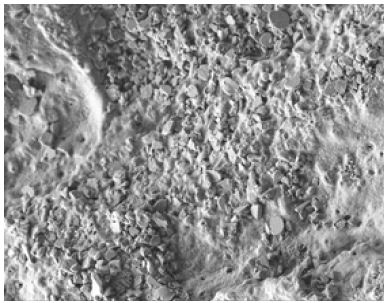
Figure 2: 1000x scanning electron microscopy image of the surface of dentine following dentine tubule occluding toothpaste application.
Table 1: Summary on the management of dentine hypersensitivity.
|
Preventive |
Reinforce good oral hygiene |
| Identify any causes of tooth wear or recession and keep thorough records of their site and severity using recognised indices such as a CHI or Schiff scores for DH’. | |
| Patients should avoid the use of abrasive dentifrices such as charcoal toothpastes and similarly avoid overloading toothbrush heads with toothpaste. | |
| Use gentle force when brushing or make use of a toothbrush with a pressure sensor. | |
| Softer bristled brushes may provide additional protection, although evidence is limited. | |
| Toothbrushes with tapered bristles may reduce the risk of abrasion, although this advice may be impractical to implement. | |
| Reduce consumption of acidic drinks and food | |
| Avoid habits such as swishing or holding drinks in the mouth | |
| Patients with suspected gastric reflux should be advised to see their GMP, it should be remembered that reflux may be silent. | |
| Toothpaste and restorative interventions as required | Conventional brushing and dab-on techniques with stannous fluoride may be beneficial |
| Calcium sodium phosphosilicate dentifrices such as NovaMin provide protection through dentinal tubule occlusion. | |
| Strontium and arginine-based dentifrices are also beneficial, although strontium is more acid resistant. | |
| Restorative treatment such as composite build ups/covering may be required in areas of tooth wear | |
| Restorative treatment of gingival recession may be considered as appropriate, such as gingival veneers, restorative restoration of recession defects and soft tissue grafting for local defects. |
Stannous Fluoride and Dab On
Dentine tubule patency has been shown recently to decrease after brushing with a stannous fluoride dentifrice and the effect was statistically significant [57]. Moreover, dab-on techniques using both stannous fluoride and sodium fluoride were found to have an even greater reduction on dentine tubule patency (over an equivalent brushing time of 4-6 weeks), with stannous fluoride being superior. There was a statistically significant decrease in patent dentine tubules when applying stannous fluoride brushing/ dab-on and sodium fluoride dab-on compared to when using sodium fluoride when brushing [57]. Sodium fluoride is mentioned further, below. This study was novel in that it demonstrated the importance of dab on and its mechanism of action [57].
Other Toothpastes When Brushing
Calcium sodium phosphosilicate (CSPS) has been suggested as a treatment for DH and is included in some toothpastes. It acts to occlude dentinal tubules and is marketed as NovaMin [58]. A 2016 study has shown that twice daily use of 5% CSPS dentifrice significantly reduces DH [56]. Novamin toothpastes have been shown to significantly decrease dentine tubule patency [59]. A systematic review and meta- analysis found similar results, indicating that CSPS use reduces DH symptoms compared to a control group [60].
Strontium based toothpastes have also been shown to be efficacious in the treatment of DH. A study has demonstrated that 8% strontium acetate toothpastes achieved a significantly greater level of tubule occlusion compared to 8% arginine. It was also reported to provide an acid-resistant layer after use, which was not found in the use of arginine [61].
A systematic review has demonstrated that arginine containing toothpastes also have positive efficacy in the reduction of dentine hypersensitivity. This was after 8 weeks of constant use [62]. Furthermore, a study investigating a twice daily use of a pro-argin mouthwash for eight weeks, found that it led to a significant reduction in DH symptoms [63].
It was demonstrated in a 2012 study that arginine-based toothpastes lead to a significant increase in tubule occlusion compared to a control group, although as discussed previously strontium performed better over a long time [61]. A 2015 study has demonstrated that arginine dentifrices may occlude tubules beneath the surface, though, once again the strontium dentifrice performed better over less time [64].
The toothpastes only work within the outer microns of teeth (up to 9 micrometres below the dentine surface) therefore very aggressive wear, e.g. lots of vomiting/very acidic drinks etc., or scaling in a dental surgery, are likely to rinse away the occluded section of dentine and require repeated toothpaste applications to help continually occlude the dentine and reduce DH symptoms [64].
Sodium Fluoride and Dab On
Sodium fluoride toothpastes have and continue to often be advised for acute management of DH, although the efficacy of fluoride as sodium fluoride is modest as it does not have substantial occluding properties [65]. It should be noted that Duraphat 2800 ppm or 5000 ppm Sodium Fluoride toothpaste is not marketed for DH but is still mistakenly prescribed for this condition.
A novel study showed that sodium fluoride used repeatedly over a longer time has been shown to create precipitation of a smear layer at the surface of the tubules when ‘dabbed’ on [57]. This is perhaps due to some Calcium Fluoride precipitates at the surface of the dentine. Nonetheless, this was not fluorapatite, which is important for greater acid resistance and as shown by other papers, above, active ingredients for DH such as Stannous Fluoride, Novamin, Strontium Acetate and Arginine, may also work in a quicker time scale.
Practitioners should bear in mind that desensitising toothpastes may be masking an underlying problem i.e. dietary acid and the importance of reducing dietary acid. Therefore, although not useful as a mode of treatment for DH symptoms, NaF used over time may be appropriate as a routine toothpaste, provided the aetiology of DH is managed.
It should be acknowledged that it is not acceptable to simply provide a toothpaste or apply an in- office procedure or application without removing the underlying predisposing features that were implicated in the initiation of DH. The importance of prevention, education and management of the condition cannot be understated. It may be sensible therefore to consider management strategies based on three specific conditions associated with DH namely 1) a patient with gingival recession, 2) a patient with periodontal disease or the impact of periodontal treatment and 3) a patient with tooth wear [66,67].
Conclusion
The prevalence of DH is high and likely to be an increasing challenge to manage for the dental profession. DH may occur on tooth surfaces occlusally or cervically. The latter is associated with NCCLs. Abfraction is a misnomer and NCCL is a better term, caused at least initially by erosion and or erosion and abrasion. Sodium fluoride is not recommended for the management of DH, patients should be counselled on the use of NovaMin, arginine, stannous fluoride and strontium dentifrices. Patients should avoid charcoal toothpastes and not overload their toothbrush head with toothpaste. Limiting the frequency and amount of extrinsic acid consumed and intrinsic erosion, the latter in liaison with the medical team, is therefore, important. Further research is needed regarding bristle stiffness, diameter, arrangement and shape as currently advising patients regarding this matter is challenging, however, reducing brushing force (whilst brushing effectively) is possibly the most important factor to consider.
The authors declare they have no conflicts of interest.
Author Contributions
Charlie Rose – Conceptualisation, drafting, editing, revisions and final approval.
Ryan Olley – Conceptualisation, editing, revisions, supervision and final approval.
David Gillam – Editing, revisions and supervision.
References
- Dowell P, Addy M (1983) Dentine hypersensitivity‐A review: Aetiology, symptoms and theories of pain J Clin Periodontol 10: 341-50. [crossref]
- Gibson BJ, Boiko O V, Baker SR, Robinson PG, Barlow APS, et (2015) The everyday impact of dentine sensitivity: personal and functional aspects. In: Dentine hypersensitivity. Elsevier; 2015. P: 89-107.
- Borges A, Barcellos D, Gomes C (2012) Dentin hypersensitivity-etiology, treatment possibilities and other related factors: a literature World Journal of Dentistry 3: 60-7.
- Chabanski MB, Gillam DG (1997) Aetiology, prevalence and clinical features of cervical dentine J Oral Rehabil 24: 15-9. [crossref]
- West NX, Davies M, Sculean A, Jepsen S, Faria-Almeida R, et al. (2024) Prevalence of dentine hypersensitivity, erosive tooth wear, gingival recession and periodontal health in seven European countries. J Dent. [crossref]
- Olley RC, Wildon, R., Moazzez R., Bartlett D. (2013) Validation of a Cumulative Hypersensitivity Index (CHI) for dentine hypersensitivity Journal of Clinical Periodontology. [crossref]
- Gillam D (2021) The impact of dentine hypersensitivity on the quality of life: an Clinical Oral Science and Dentistry. [crossref]
- Olley RC, Sehmi H (2017) The rise of dentine hypersensitivity and tooth wear in an ageing population. Br Dent J 223: 293-7. [crossref]
- Dababneh RH, Khouri AT, Addy M (1999) Dentine hypersensitivity—An enigma? A review of terminology, mechanisms, aetiology and Br Dent J 187: 606-11. [crossref]
- Addy M (2005) Tooth brushing, tooth wear and dentine hypersensitivity—are they associated? Int Dent J 55: 261-7. [crossref]
- Greuling A, Emke JM, Eisenburger M (2021) Abrasion behaviour of different charcoal toothpastes when using electric Dent J (Basel) 9: 97. [crossref]
- Inchingolo AM, Malcangi G, Ferrante L, Del Vecchio G, Viapiano F, et al. (2023) Damage from carbonated soft drinks on enamel: a systematic review. Nutrients 15:1785. [crossref]
- Qutieshat A, Aouididi (2020) Carbonated beverage consumption among UK university students. Expert journal of marketing 8: 73-81.
- Bandy LK, Scarborough P, Harrington RA, Rayner M, Jebb SA (2020) Reductions in sugar sales from soft drinks in the UK from 2015 to BMC Med 18: 1-10. [crossref]
- Dionysopoulos D, Gerasimidou O, Beltes C (2023) Dentin hypersensitivity: etiology, diagnosis and contemporary therapeutic approaches—a review in Applied Sciences 13: 11632. [crossref]
- Yadav VS, Gumber B, Makker K, Gupta V, Tewari N,et (2023) Global prevalence of gingival recession: A systematic review and meta‐analysis. Oral Dis 29: 2993-3002. [crossref]
- Fischer C, Fischer RG, Wennberg A (1992) Prevalence and distribution of cervical dentine hypersensitivity in a population in Rio de Janeiro, J Dent 20: 272-6. [crossref]
- Heasman PA, Holliday R, Bryant A, Preshaw PM (2015) Evidence for the occurrence of gingival recession and non‐carious cervical lesions as a consequence of traumatic J Clin Periodontol 42: S237-55. [crossref]
- Plessas A, Pepelassi E (2012) Dental and periodontal complications of lip and tongue piercing: prevalence and influencing factors. Aust Dent J 57: 71-8. [crossref]
- Tugnait A, Clerehugh (2001) Gingival recession—its significance and management. J Dent 29: 381-94. [crossref]
- Bubteina N, Garoushi S (2015) Dentine hypersensitivity: a Dentistry 5: 330-6.
- Pashley DH (2013) How can sensitive dentine become hypersensitive and can it be reversed? J Dent 41: S49-55. [crossref]
- Addy M (2002) Dentine hypersensitivity: new perspectives on an old Int Dent J 52: 367-75.
- Olley RC, Moazzez R, Bartlett (2015) The relationship between incisal/occlusal wear, dentine hypersensitivity and time after the last acid exposure in vivo. J Dent 43: 248-52. [crossref]
- Martin J, Fernandez E, Bahamondes V, Werner A, Elphick K, et al. (2013) Dentin hypersensitivity after teeth bleaching with in-office Randomized clinical trial. Am J Dent 26: 10-4. [crossref]
- Haywood VB, Sword RJ (2017) Tooth bleaching questions answered. Br Dent J 223: 369-80. [crossref]
- Greenwall LH, Greenwall-Cohen J, Wilson NHF (2019) Charcoal-containing Br Dent J 226: 697-700. [crossref]
- Tomas DBM, Pecci-Lloret MP, Guerrero-Girones J (2023) Effectiveness and abrasiveness of activated charcoal as a whitening agent: A systematic review of in vitro Annals of Anatomy-Anatomischer Anzeiger 245: 151998. [crossref]
- Franco MC, Uehara JLS, Meroni BM, Zuttion GS, Cenci MS (2020) The effect of a charcoal-based powder for enamel dental bleaching. Oper Dent 45: 618-23. [crossref]
- Koc Vural U, Bagdatli Z, Yilmaz AE, Yalçın Çakır F, Altundaşar E et (2021) Effects of charcoal-based whitening toothpastes on human enamel in terms of color, surface roughness, and microhardness: an in vitro study. Clin Oral Investig 25: 5977-85. [crossref]
- Zoller MJ, Hamza B, Cucuzza C, Gubler A, Attin T, et al. (2023) Relative dentin and enamel abrasivity of charcoal toothpastes. Int J Dent Hyg 21: 149-56. [crossref]
- Ghajari MF, Shamsaei M, Basandeh K, Galouyak MS (2021) Abrasiveness and whitening effect of charcoal-containing whitening toothpastes in permanent teeth. Dent Res J (Isfahan) 18: 51. [crossref]
- Franzo D, Philpotts CJ, Cox TF, Joiner A (2010) The effect of toothpaste concentration on enamel and dentine wear in J Dent 38: 974-9. [crossref]
- Carneiro BT, Kury M, Lopes JC, Goncalves RS, Suzuki TYU, et (2023) Effect of whitening toothpastes and activated charcoal powder on enamel wear and surface roughness. Braz Oral Res 37: e092. [crossref]
- Bragança GF, Soares PBF, Simeão Borges J, Fernandes Vilela AB, Santos Filho PC, et (2022) Effects of charcoal toothpaste on the surface roughness, color stability, and marginal staining of resin composites. Oper Dent 47: 214-24. [crossref]
- Sehmi H, Olley RC (2015) The effect of toothbrush abrasion force on dentine hypersensitivity in-vitro. J Dent 43: 1442-7. [crossref]
- Hamza B, Tanner M, Körner P, Attin T, Wegehaupt FJ (2021) Effect of toothbrush bristle stiffness and toothbrushing force on the abrasive dentine Int J Dent Hyg 19: 355-9. [crossref]
- Turssi CP, Binsaleh F, Lippert F, Bottino MC, Eckert GJ, et (2019) Interplay between toothbrush stiffness and dentifrice abrasivity on the development of non- carious cervical lesions. Clin Oral Investig 23: 3551-6. [crossref]
- Bizhang M, Schmidt I, Chun YHP, Arnold WH, Zimmer S (2017) Toothbrush abrasivity in a long-term simulation on human dentin depends on brushing mode and bristle PLoS One 12: e0172060. [crossref]
- Hamza B, Svellenti L, Körner P, Attin T, Wegehaupt FJ (2022) Effect of tapered-end and round-end bristles on the abrasive dentine wear applying increasing brushing Acta Odontol Scand 80: 465-9. [crossref]
- Hamza B, Niedzwiecki M, Körner P, Attin T, Wegehaupt FJ (2022) Effect of the toothbrush tuft arrangement and bristle stiffness on the abrasive dentin Sci Rep 12: 840.
- O’Toole S, Bartlett D (2017) The relationship between dentine hypersensitivity, dietary acid intake and erosive tooth wear. J Dent 67: 84-7. [crossref]
- Chan AS, Tran TTK, Hsu YH, Liu SYS, Kroon J (2020) A systematic review of dietary acids and habits on dental erosion in Int J Paediatr Dent 30: 713-33. [crossref]
- Lussi A, Schaffner M (2000) Progression of and risk factors for dental erosion and wedge-shaped defects over a 6-year period. Caries Res 34: 182-7. [crossref]
- West NX, Sanz M, Lussi A, Bartlett D, Bouchard P, et (2013) Prevalence of dentine hypersensitivity and study of associated factors: a European population-based cross- sectional study. J Dent 41(10): 841-51. [crossref]
- Olley RC, Frost BEM PM (2019) Clinical and academic recommendations for primary dental care Br Dent J 227: 451-5. [crossref]
- Villamayor KGG, Codas-Duarte D, Ramirez I, Souza-Gabriel AE, Sousa-Neto MD, et (2024) Morphological characteristics of non-carious cervical lesions. A systematic review. Arch Oral Biol 106050. [crossref]
- Lee WC, Eakle WS (1984) Possible role of tensile stress in the etiology of cervical erosive lesions of J Prosthet Dent 52: 374-80. [crossref]
- Grippo Abfractions (1991) a new classification of hard tissue lesions of teeth. Journal of Esthetic and Restorative Dentistry 3: 14-9. [crossref]
- Bhundia S, Bartlett D, O’Toole S (2019) Non-carious cervical lesions-can terminology influence our clinical assessment? Br Dent J 227: 985-8. [crossref]
- Senna P, Del Bel Cury A, Rösing C (2012) Non‐carious cervical lesions and occlusion: a systematic review of clinical J Oral Rehabil 39: 450-62. [crossref]
- Rees JS (2022) The effect of variation in occlusal loading on the development of abfraction lesions: a finite element J Oral Rehabil 29: 188-93. [crossref]
- Sarode GS, Sarode SC (2013) Abfraction: A Journal of Oral and Maxillofacial Pathology 17: 222-7. [crossref]
- Dzakovich JJ, Oslak RR (2008) In vitro reproduction of noncarious cervical lesions. J Prosthet Dent 100: 1-10. [crossref]
- Bhundia S, Bartlett D, O’Toole S (2019) Non-carious cervical lesions-can terminology influence our clinical assessment? Br Dent J 227: 985-8. [crossref]
- Mason S, Kingston R, Shneyer L, Harding M (2017) Clinical study to monitor dentinal hypersensitivity with episodic use of a desensitising dentifrice. BDJ Open 3: 1-6. [crossref]
- Olley RC, Mohsen BM, Alhaij S, Appleton PL(2020) Measurement of eroded dentine tubule patency and roughness following novel dab-on or brushing abrasion. J Dent 98: 103358. [crossref]
- Mohammed A, Ofuonye I (2017) Dentine hypersensitivity: review of a common oral health J Dent Craniofac Res 2: 16.
- Mullan F, Paraskar S, Bartlett DW, Olley RC (2017) Effects of tooth-brushing force with a desensitising dentifrice on dentine tubule patency and surface J Dent 60: 50-5. [crossref]
- Zhu M, Li J, Chen B, Mei L, Yao L, et (2015) The effect of calcium sodium phosphosilicate on dentin hypersensitivity: a systematic review and meta-analysis. PLoS One 10: e0140176. [crossref]
- Olley RC, Pilecki P, Hughes N, Jeffery P, Austin RS, Moazzez R, et al. (2012) An in situ study investigating dentine tubule occlusion of dentifrices following acid challenge. J Dent 40: 585-93. [crossref]
- Sharif MO, Iram S, Brunton PA (2013) Effectiveness of arginine-containing toothpastes in treating dentine hypersensitivity: a systematic J Dent 41: 483-92. [crossref]
- Hu D, Stewart B, Mello S, Arvanitidou L, Panagakos F, et (2013) Efficacy of a mouthwash containing 0.8% arginine, PVM/MA copolymer, pyrophosphates, and 0.05% sodium fluoride compared to a negative control mouthwash on dentin hypersensitivity reduction. A randomized clinical trial. J Dent 41: S26-33. [crossref]
- Olley RC, Moazzez R, Bartlett D (2015) Effects of dentifrices on subsurface dentin tubule occlusion: an in situ International Journal of Prosthodontics 28: 2. [crossref]
- Petersson (2013) The role of fluoride in the preventive management of dentin hypersensitivity and root caries. Clin Oral Investig 17: 63-71. [crossref]
- Gillam DG, Chesters RK, Attrill DC, Brunton P, Slater M, et (2013) Dentine hypersensitivity-guidelines for the management of a common oral health problem. Dent Update 40: 514-24. [crossref]
- Gillam DG (2017) A new perspective on dentine hypersensitivity-guidelines for general dental Dent Update 44: 33-42. [crossref]