Abstract
During the last 20 years, several regional indoor radon assessment campaigns were carried out in Transilvania (Romania), evaluating the conditions in more than 2000 buildings. The area with the highest indoor radon concentration in Transilvania, is represented by Ştei-Băiţa (Bihor County), located in the perimeter of several uranium mines, were values up to 4000Bq/m3 were recorded. Our research meant to identify the radioactive nuclides present in the dental tissues of the native population in the mentioned area. Gamma-spectroscopy was used to identify the nuclides out of the powder resulted from milling extracted teeth. Previously teeth were split into 3 groups according to the individual’s age. No radioactive elements’ nuclides were identified in the teeth structures. Authors assume that either the radiation is too low to induce hard tissue contamination or the locally identified elements (uranium, thorium, radon, radium) don’t affix in these tissues.
Keywords
nuclide, radioactive, radon, uranium, dental, teeth
Introduction
Radon is a radioactive gas, generated by uranium deposits. It is emitted normally by rocks, earth’s crust, and it can delve inside the buildings through planking, wall cracks, or along the pipes [1]. It can be present not only in the air but also in soil and construction materials. In areas with high potential risk (i.e. uranium mines), radon’s air concentration can reach high values due to both soil and construction materials [2]. Recent researches showed that radon is the main source of population’s natural irradiation, contributing with approximately 57% to the effective annual radiation dose and it can rise, in certain areas, to a contribution of 95%, cases in which the exposure to natural radiation is 5-10 times higher than the medium exposure value of 2,2 mSv/year [2,3].
During the last 20 years, several regional indoor radon assessment campaigns were carried out in Transilvania (Romania), evaluating the conditions in more than 2000 buildings [4]. The area with the highest indoor radon concentration in Transilvania is represented by Ştei-Băiţa (Bihor County), located in the perimeter of several uranium mines, were values up to 4000Bq/m3 were recorded [5]. World Health Organization recommends security limits regarding radon exposure inside buildings, between 100-200Bq/m3 [2]. On the upper course of the Black Cris river at approximately 25 km from the city of Ştei, the uranium deposit from Băiţa was exploited between 1950 and 2000, is considered the biggest uranium deposit in Romania.In Băiţa-Plai village there are more dump tailings coming from the mine, containing uranium waste which was used by the locals as construction materials for buildings, houses, annex households, etc. Subsequently, Radon-222, Radium-226, Uranium, Thorium concentrations were found as overcoming the limits allowed by rules in force. About 30% of the measured values are significantly higher than the recommended level of 200Bq/m3. Therefore, Ştei-Băiţa mining area is proposed to be included on the “hot-spot” list by the Ministry of Environment, by the radon contamination point of view [1].
Aim
The population in the above-mentioned area is approximately 700 individuals, adults and children, 99 in Băiţa-Plai, 599 in Băiţa, respectively, according to the last population census in 2012 [6]. Considering the radioactive environment that people from Băiţa and Băiţa-Plai live in, authors assumed that radioactive nuclides from the environment may be captured by human dental tissue and evidenced through specific analysis. Thus, aim of the present study was to determine the presence of these radio-nuclides in human dental tissue, in residential population. Excluding criteria: children who’s exposure time is relatively short compared with adults.
Materials and Methods
82 permanent teeth with severe destruction were extracted from mature people aged between 25 and 73, who worked or lived in the mining area for at least 10 years. Teeth were collected, cleaned in warm water (500C) and dried at room temperature. Three sample groups were created according to patients’ age, as follows: group 1 – individuals below 0-30 years, including 27 teeth, group 2 – individuals between 30 and 60 years including 30 teeth, group 3 – individuals over 60 years including 25 teeth. Thus this study included more than 10% of the population living in the exploitation’s neighborhood.
Teeth from all the 3 groups were milled using Pulverisette 7 ball-mill (Fritsch Laborgeräte GmbH, Idar-Oberstein, Germany) at a relative rotational speed of the grinding bowls of 2200rpm, resulting in a fine powder with particles having 100nm (10-9m). Then sample material was then subjected to gamma spectrometry analysis.
The gamma spectrometer used in this study (Fig.1) consisted in: a detection probe containing thallium-doped sodium iodide NaI(Tl) scintillation counters with photomultipliers that convert the light into electrons and then amplify the electrical signal provided by those electrons; a multichannel analyzer (MCA) with 1024 channels with a PCAP-plus interface; Assayer Oxford WIN-MCA spectra acquisition software; RadiationHelper data analysis software; Desktop computer as data readout device, to generate, display and store the spectrum; the lead shield that isolates the detector from being contaminated by natural radioactivity; Sarpagan boxes which respect the geometry of measuring. This spectrometric ensemble has an efficiency of 3,5% at 662keV and a resolution of 7% at the same voltage. The samples as powder were poured in the Sarpagan box and placed onto the detecting chamber. Considering that the expected amount of nuclides was very small, the reading time for each sample’s gamma spectrum was set to 20 hours. After the mentioned time, the measured spectrum was analyzed searching for uranium, thorium, cesium, and potassium elements and determining the peaks according to their maximum level. Energy is identified for each peak (Ei), meanwhile determining the corresponding isotopes for each energy, with the aid of the energy calibration curve. The activity of each gamma nuclide is computed using the characteristic photo-peaks.
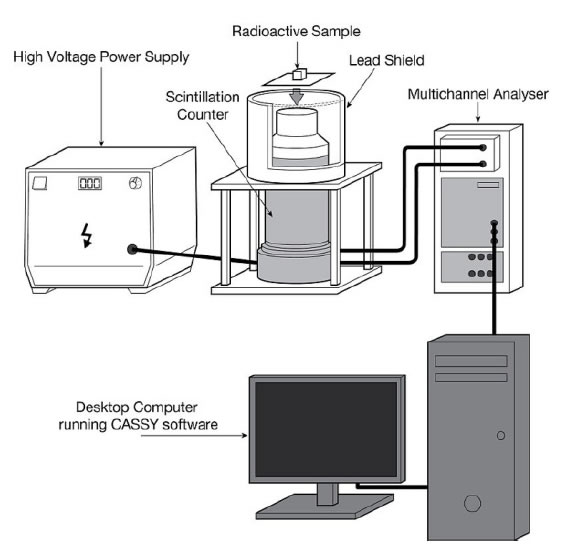
Figure 1. Schematic laboratory equipment for gamma spectroscopy.
Results
The study included more than 10% of the population living in the area of the investigation. The results of the present study are reported in Table 1. The values shows the identity and quantity of gamma emitters present in the gamma source, in this case, the milled tooth hard tissue.
|
Table 1: Valuesiforithe i3isamples |
||||
|
|
ELEMENTS |
|||
|
Sample |
K(Potassium) |
U(uranium) |
Th(thorium) |
Cs(cesium) |
|
1 |
< i9iBq/kg |
< i110iBq/kg |
< i41iBq/kg |
< i30iBq/kg |
|
2 |
< i9iBq/kg |
< i110iBq/kg |
< i41iBq/kg |
< i30iBq/kg |
|
3 |
< i9iBq/kg |
< i110iBq/kg |
< i41iBq/kg |
< i30iBq/kg |
According to our findings, although natural and artificial radiation were identified as exceeding the recommended values in the mentioned area, this kind of pollution did not have an effect on tooth structure, did not affix in dental tissue regardless the age of individuals or the time of exposure at locally measured radioactivity. For all 3 groups the gamma spectrum had similar values and the same graphical area (Fig.2-4). Gamma spectrometry found no significant differences among the 3 groups, as that searched elements and their nuclides are absent in analyzed dental tissues.
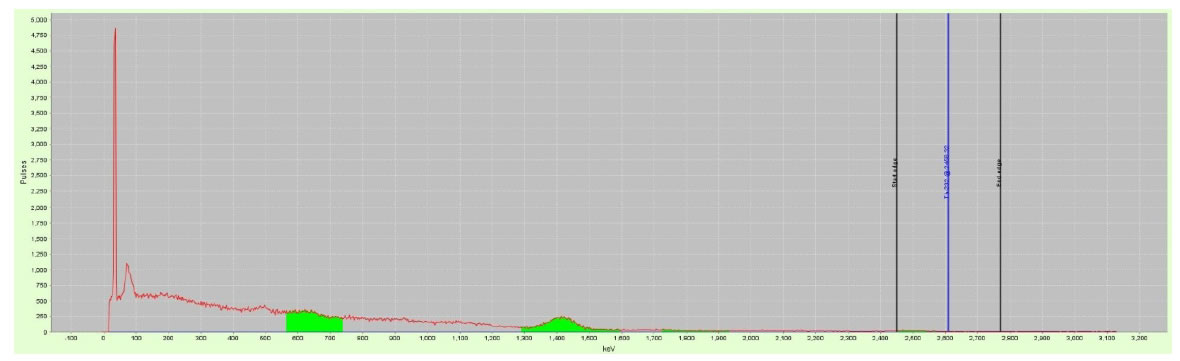
Figure 2. Gamma spectrum of sample group i1.
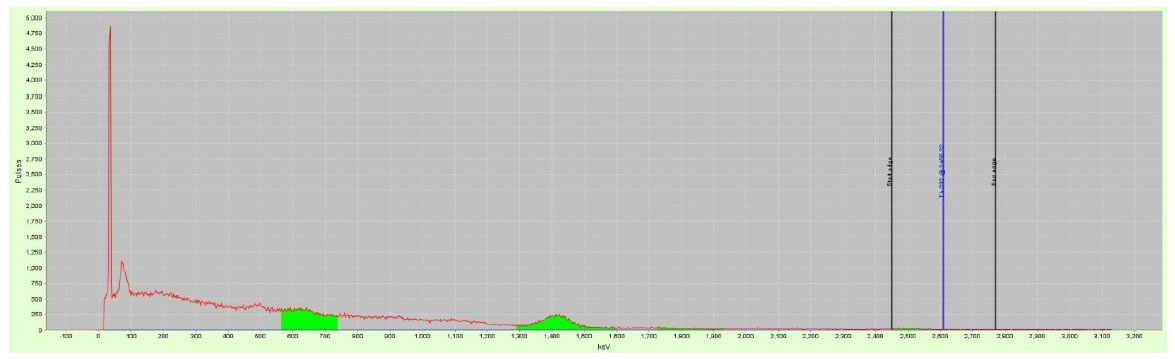
Figure 3. Gamma spectrum of sample group 2.
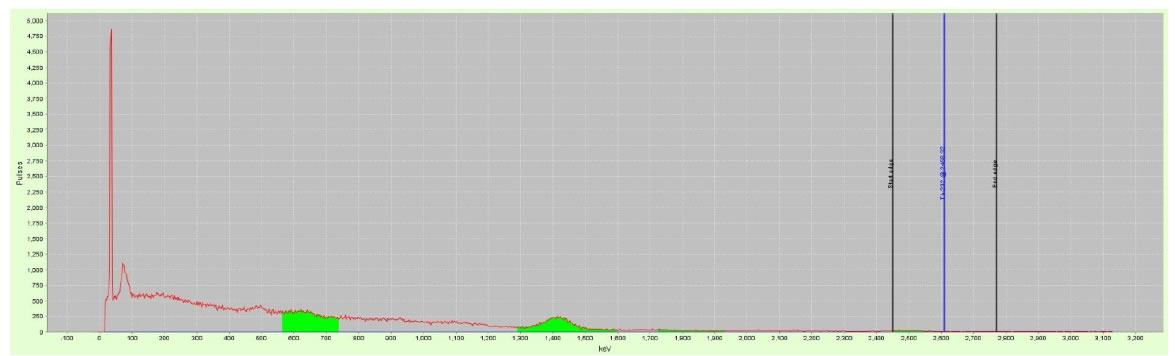
Figure 4. Gamma spectrum of sample group 3.
Although our research didn’t find any signs of nuclides retained in dental tissues, this means that either the radioactivity and environmental pollution with such elements aren’t high enough to leave a mark in human hard tissue, or these elements simply aren’t deposited in these tissues (bones, teeth). Even so, the pollution is registered and proved by systematic measurements. According to the county’s Public Health Department which is periodically surveying the area, numbers of newly detected cancer cases were 27 in 2011, 23 in 2012, 24 in 2013, 16 in 2014, and 6 newly diagnosed cancer cases in 2015. These data include the cities of Stei and Nucet along with the Baita and Baita-Plai villages.
Factors that favor the increase of indoor radon in buildings from Băiţa and Băiţa Plai are:
• rock’s high radioactive potential from the subsoil in that area, porosity, permeability, and their finishing grade;
• use of some materials recovered from the mining chambers, as materials for households(mine wood, rails, pipes) or ornamental rocs kept in the house [2,8].
Measurements were carried out by the Public Health Department over the years, assessing the global-α, global-β, radioactive Radium-226 separation, and natural Thorium radiations. Mine water samples were collected from the following three galleries: 23, 11, and “Good luck”. Surface water was collected from Baita Cris river, which collects the mine watercourses from all around the Baita Plai mines, the Black Cris river, where the mine waters are collected, respectively.
Tap water pipes were checked in Fanate, Campani, Baita, Stei, and Nucet villages, proved to be safe for the population, with values that are consistent with those recommended for consumption (Law 458/2002) [9].
As may be seen in Table 2, increased values of nuclides, compared with tap water, were found in residual water in the mine galleries, and in the Valea Plaiului river which is tributary to Baita Cris river.
|
Table 2: Radioactivity check on environment samples collected in the area of the nuclear facility’siimpact zone |
||||
|
Nr. |
SAMPLEiTYPE |
YEAR |
TotaliNr.iofisamples |
Samplesiwithiexceededivalues |
|
1 |
mineiwater |
2007 |
8 |
8 |
|
2008 |
10 |
10 |
||
|
2009 |
12 |
12 |
||
|
2010 |
15 |
15 |
||
|
2011 |
12 |
12 |
||
|
2012 |
14 |
14 |
||
|
2013 |
3 |
3 |
||
|
2014 |
2 |
2 |
||
|
2015 |
4 |
4 |
||
|
2 |
depositiwater |
2007 |
2 |
2 |
|
2008 |
2 |
2 |
||
|
2009 |
1 |
1 |
||
|
2010 |
2 |
2 |
||
|
2011 |
4 |
4 |
||
|
2012 |
4 |
4 |
||
|
2013 |
4 |
4 |
||
|
2014 |
2 |
2 |
||
|
2015 |
1 |
1 |
||
|
3 |
surfaceiwater |
2007 |
11 |
3 |
|
2008 |
14 |
4 |
||
|
2009 |
23 |
4 |
||
|
2010 |
23 |
3 |
||
|
2011 |
30 |
5 |
||
|
2012 |
30 |
5 |
||
|
2013 |
10 |
2 |
||
|
2014 |
13 |
– |
||
|
2015 |
15 |
2 |
||
|
4 |
spontaneousivegetation |
2007 |
14 |
12 |
|
2008 |
20 |
17 |
||
|
2009 |
18 |
11 |
||
|
2010 |
11 |
6 |
||
|
2011 |
16 |
8 |
||
|
2012 |
35 |
21 |
||
|
2013 |
11 |
5 |
||
|
2014 |
5 |
2 |
||
|
2015 |
6 |
3 |
||
|
5 |
atmosphericideposition |
2010 |
1 |
– |
|
2011 |
5 |
– |
||
|
2012 |
3 |
– |
||
|
2013 |
1 |
– |
||
|
2014 |
2 |
– |
||
|
2015 |
2 |
– |
||
|
6 |
Food |
2010 |
3 |
– |
|
2011 |
13 |
– |
||
|
2012 |
5 |
– |
||
|
2013 |
6 |
– |
||
|
2014 |
2 |
– |
||
|
2015 |
– |
– |
||
|
7 |
drinkingiwater |
2008 |
2 |
– |
|
2009 |
2 |
– |
||
|
2010 |
4 |
– |
||
|
2011 |
6 |
– |
||
|
2012 |
6 |
– |
||
|
2013 |
6 |
– |
||
|
2014 |
6 |
– |
||
|
2015 |
2 |
– |
||
Discussion
Gamma-ray spectroscopy is a non-invasive, quantitative study of the energy spectra of gamma-ray sources, in such as the nuclear industry, geochemical investigation, and astrophysics. Most radioactive sources produce gamma rays, which are of various energies and intensities. When these emissions are detected and analyzed with a spectroscopy system, a gamma-ray energy spectrum can be produced. A detailed analysis of this spectrum is typically used to determine the identity and quantity of gamma emitters present in a gamma source, and is a vital tool in radiometric assay. The gamma spectrum is characteristic of the gamma-emitting nuclides contained in the source, just as in optical spectroscopy, the optical spectrum is characteristic of the material contained in a sample. Gamma spectroscopy detectors are passive materials that wait for a gamma interaction to occur in the detector volume. The most important interaction mechanisms are the photoelectric effect, the Compton effect, and pair production. When a gamma ray undergoes a Compton interaction or pair production, and a portion of the energy escapes from the detector volume without being absorbed, the background rate in the spectrum is increased by one count. This count will appear in a channel below the channel that corresponds to the full energy of the gamma ray. Larger detector volumes reduce this effect. The voltage pulse produced by the detector (or by the photomultiplier in a scintillation counter) is shaped by a multichannel analyzer (MCA). The multichannel analyzer takes the very small voltage signal produced by the detector, reshapes it into a Gaussian or trapezoidal shape, and converts that signal into a digital signal. In some systems, the analog-to-digital conversion is performed before the peak is reshaped [7].
According to our findings, although natural and artificial radiation were identified as exceeding the recommended values in the mentioned area, this kind of pollution did not have an effect of tooth structure, did not affix in dental tissue regardless the age of individuals or the time of exposure at locally measured radioactivity. Considering that teeth belong to all age categories, authors assume that the study is pretty representative and that there is no significant nuclear contamination in researched area. Measured values are even lower than the natural radioactivity.
In a quite similar study carried out in the same geographical area [10], authors used temporary teeth’s(not mentioned how many) enamel to identify radio-nuclides, without any success, assuming that temporary teeth have an insufficient lifetime on the arches to be contaminated by this kind of pollution. Hereby, we can confirm their findings, mentioning that even a long time exposure is insufficient to determine a nuclide accumulation in human hard tissue. It seems that this is a nuclide and radiation level-sensitive issue, assuming that uranium and all the other elements followed here are retained only after a higher level of exposure and that may be an exposure to other radioactive nuclides (ex. Cesium) at the same level of radioactivity is absorbed quicker and deeper in the human organism.
In all phases of the technological processes involved in the exploitation of the uranium ore (exploitation, transport, storing the radioactive materials) high concentration radon is released in the environment [2]. Radon inside buildings represents the main source of human exposure to ionizing radiation in the world. Studies in many countries have shown that high levels of indoor radon increase the risk of lung cancer [1]. Recent epidemiologic studies proved the correlation between lung cancer and radon concentration even in so-considered normal concentrations of 40-300Bq/m3. The conclusion emphasized that radon inside buildings is responsible for lung cancer in 9% of the cases [11,12,13]. In high quantities radon can cause severe respiratory deficiencies, being considered the second cause of lung cancer, after smoking according to IARC, ICRP, WHO, UNSCEAR [2,14,15,16,17]. It is recognized as impossible to eliminate exposure to radon, only to limit the exposure to it. The critical situation requires detailed monitoring of all houses in Bǎiţa area to implement methods to reduce indoor radon levels [1].
The use of uranium waste from the uranium mines that were in use between 1950-1990 as construction materials, constructions on soil with high permeability and foundation structures that allows radon infiltration from the soil towards the inner space of the houses, are the main causes of the increased indoor radon concentrations in this specific area [1]. The magnitude of exposure to radon, in 303 buildings located nearby the mine, is 3,5 times higher than the medium concentration value of indoor radon which is 82,5Bq/m3, reported for Transilvania [1,4,5]. The results are indicating high levels of radon in Baita area, arguing that the percent of mortality caused by lung cancer attributable to radon exposure is the highest from Romania and Europe [1,6,11]. As a result, the population’ health is affected by the environment’s pollution, so that higher mortality rates, raised lung cancer rate, and decreased life expectancy is noticeable in areas like this [2]. Therefore we can conclude that this kind of radiation is exploitation(natural) one, not an artificial one, generated either by nuclear fusion or disruption, which damages more severely the living organisms. Its effect is a long term one, in this case affecting the lungs, due to lung depositing of these elements. Also, it is worthy of mentioning that there are two kinds of radioactive contamination, affixed and un-affixed. In our case we are witnessing un-affixed contamination in teeth and affixed contamination in the lungs.
Conclusion
Therefore we can conclude that this kind of radiation is exploitation (natural) one, not an artificial one, generated either by nuclear fusion or disruption, which damages more severely the living organisms. Its effect is a long term one, in this case affecting the lungs, due to lung depositing of these elements. Also, it is worthy of mentioning that there are two kinds of radioactive contamination, affixed and un-affixed. In our case we are witnessing un-affixed contamination in teeth and affixed contamination in the lungs.
References
- Alexandra CucoşD, Cosma C, Dicu T,Papp B, NiţǎDC et al. (2011). Actual situation of indoor radon measurements and the perspective of remedial actions in Baita-Bihor mining area. Ecottera 8: 25-32
- Constantin Cosma, Sainz C, Alexandra Cucos, Dicu T, Begy R et al. (2011). Implementation of remedial techniques for radon in dwellings from baita uranium mine area. Concept of Radioprotection culture” and its role in population and environment protection- National Confference Bucharest.
- Cosma C, Dicu T, Dinu A, Begy R (2009) Radon and lung cancer, Ed. Quantum, Cluj-Napoca 166.
- Cosma C, Szacsvai K, Dinu A, Ciorba D, Dicu T et al. (2009) Preliminary integrated indoor radon measurements in Transilvana. Isotopes in Environmental and Health Studies 45: 1-10. [crossref]
- Sainz C, Dinu A, Dicu T, Szacsvai K, Cosma C et al. (2009) Comparative risk assessment of residential radon exposures in two radon – prone areas, Stei (Romania) and Torrelodones (Spain). Science of The Total Environment 407: 4452-4460. [crossref]
- INS, http://www.insse.ro/
- Wikipedia https://en.wikipedia.org/wiki/Gamma_spectroscopy
- Dinu A (2009) Correlations between indoor radon and lung cancer incidence in Stei-Baita mining area”. phd thesis, Cluj Napoca.
- http://www.ms.ro/wp-content/uploads/2017/02/Proiect-Lege-modcompl.458.pdf
- Porumb A, Romanul I, Bungău S (2012) The determination of impurities, coming from radioactive pollution, in temporary teeth samples, using the neutrons activation analysis method. AnimalHusbandry and Food Industries Technologies 11: 191-196
- Ferlay J, Autier P, Boniol M, Heanue M, Colombet M et al. (2007) Estimates of the cancer incidence and mortality in Europe 2006. Annals of Oncology18: 581-592. [crossref]
- Field RW, Krewski D, Lubin JH, Zielinski JM, Alavanja M et al. (2006) An overview of the North American case-control studies of residential radon and lung cancer. J Toxicol Environ A 69: 599-631. [crossref]
- Darby S, Hill D, Deo H, Auvinen A, Barros-Dios JM et al. (2006) Residential radon and lung cancer-detailes results of a collaborative analysis of individual data on 7148 persons with lung cancer and 14208 persons without lung cancer from 13 epidemiologic studies in Europe”.Scandinavian Journal of Work Environment and Health32: 1-84. [crossref]
- IARC International Agency for Research on Cancer (1988) Man-made Mineral Fibres and Radon”. Monographs on the Evaluation of Carcinogenic Risks to Humans 43: 309.
- ICRP International Comission on Radiological Protection (1994). Protection against Radon-222 at home and at work, Publication 65 23: 45.
- UNSCEAR United Nation Scientific Commitee on the Effects of Atomic Radiation (2000). Sources and Effects of Ionizing Radiation, Report to General Assembly with Scientific Annexes 1: 654
- World Health Organization http://www.WHO.int/whosis/database/