Abstract
Introduction: Coronavirus disease 2019 (COVID-19) is a pandemic and public health emergency caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Our study evaluated the impact of the COVID-19 on patients with Charcot-Marie-Tooth (CMT), the most common genetic neuromuscular disorder.
Methods: A simple online questionnaire for CMT patients diagnosed with COVID-19 was developed to investigate how much the COVID-19 impacted the community of CMT patients and its consequences on the progression of CMT. With the support of the Italian CMT patient Association (ACMT-Rete) and the American CMT Association (CMTA), the survey was distributed electronically through the INC Contact Registry and the web-based Contact Registry in the US, and in Italy through the Italian CMT Registry, ACMT-Rete members newsletter and social networks.
Results: 152 individuals completed the survey. Approximately 59% of completers were female, and the average age was 49.96 (SD 12,65, range 22-76 years). 13.8% of the respondents had a COVID diagnosis and 2% (n=3) of them were health workers. Symptoms of COVID-19 were typically mild and none went to the ICU.
Discussion: These results do not show a clear increased risk of COVID in people with CMT.
Keywords
Charcot Marie Tooth, CMT, COVID-19, Survey
Introduction
Coronavirus disease 2019 (COVID-19) is a pandemic and public health emergency caused by the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). COVID-19 symptoms include fever, cough, fatigue, shortness of breath, sore throat, headache, diarrhea, anosmia and ageusia/dysgeusia. Severe manifestations, including pneumonia, acute respiratory distress syndrome, cytokine storm, myocardial injury, and death are more common in older patients and those with medical comorbidities [1-6]. Our study evaluated the impact of the COVID-19 on patients with Charcot-Marie-Tooth (CMT), the most common inherited neuromuscular disorder [7,8]. The COVID-19 pandemic has resulted in the reorganization of health-care settings affecting clinical care delivery to patients with CMT as well as other inherited neuromuscular disorders [6,9]. How much this public health emergency has impacted the care of patients with CMT is unclear, although there is a concern that the lockdown measures impacted on patient activity [10]. There are also concerns that people with CMT and other neuromuscular diseases are at an increased risk for severe presentations of COVID-19.
We investigated how many participants in our online cohort were diagnosed with COVID-19, the symptoms they presented with, the presence of risk factors, and how the COVID-19 impacted the progression of their CMT.
Methods
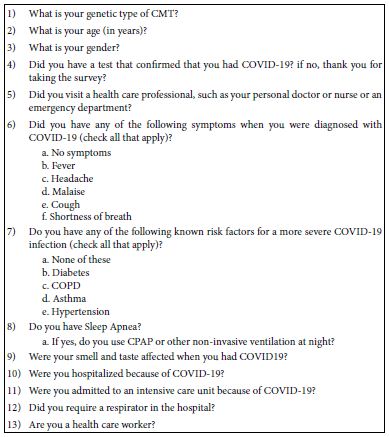
The study was approved by the Institutional Review Board of the University of Iowa. A simple online questionnaire for CMT patients (Table 1) was developed to investigate how much COVID-19 impacted the community of CMT patients and its consequences on the progression of CMT. Then with the support of the Italian CMT patient Association (ACMT-Rete) and the American CMT Association (CMTA), the survey was distributed electronically through the INC Contact Registry and the web-based Contact Registry in the US, and in Italy through the Italian CMT Registry (http://www.registronmd.it/), ACMT-Rete members newsletter and social networks. In the US contact registry, 53.45% have CMT1A, 3.77% have CMT1B, 4,93% have CMT1X, 9,69% have CMT 2A and 26,19% have CMT without a subtype or genetic classification. Nearly 3500 individuals participate in the registry. All registry participants between the ages of 18 to 90 were invited and provided consent to participate in this survey. Data regarding age, gender, CMT type and if participants were health workers were collected. The CMT-COVID Survey was anonymous and included COVID-19 related questions, accessible only if the participants had both CMT and have been diagnosed with COVID-19. Participants specifically diagnosed with CMT were asked to complete the survey. The specific questions regarding COVID-19 concerned 1) symptoms from COVID-19, 2) the presence of pre-existing risk factors, 3) the presence of sleep apnea and, if so, whether CPAP or non-invasive ventilation was required, 4) if hospitalization and, if so, admission to an intensive care unit (ICU) occurred, 5) if a respirator/ventilator was required in the hospital. Demographic information on gender, age, and genetic diagnosis of the participants was obtained. Percentages were determined for all questions for each response category.
Table 1: The Survey
Results
A total of 153 patients completed the survey between May 2020 and January 2021. Approximately 59% (n=90) of responders were female, and the average age was 49.96 (SD 12.65, range 22-76 years). CMT types were represented as follows: CMT1A 46% (n=71), CMT1B 8% (n=12), CMTX1 6% (n=9), CMT2 16% (n=25), CMT4 2% (n=3), HNPP 2.6% (n=4) and 19% (n=29) did not specify the type of their CMT. Twenty-one patients (13%) had a diagnosis of COVID-19 (17 female); two of these were health workers. The remaining 124 individuals completed the survey even though they had not been diagnosed with COVID-19. Queried symptoms included fever, headache, fatigue, cough, shortness of breath, sore throat, muscular or joint pain and diarrhea (Table 2): 76% of the 21 patients (n=16) reported all symptoms, 5% (n=1) all symptoms except shortness of breath, diarrhea, and sore throat, 14% (n=3) only fever, headache, and cough, 5% (n=1) fever, headache and sore throat. Smell or taste affected 62% (n=13). We queried diabetes, COPD, asthma, and hypertension as potential risk factors: 85% (n=18) of participants had none of these risk factors, 9% (n=2) had diabetes and 5% hypertension (n=1). One also reported sleep apnea. All those with COVID-19 were evaluated by health care professionals, but none of the participants were hospitalized.
Table 2: Symptoms/Risk Factors
| Symptom/Risk Factor | # Responded Yes |
| Cough | 20 |
| Fever | 21 |
| Headache | 21 |
| Fatigue | 17 |
| Sore throat | 17 |
| Shortness of Breath | 16 |
| Muscular or joint pain | 17 |
| Diarrhea | 16 |
| No Symptoms | 0 |
| Smell and/or taste affected | 13 |
| Have Risk Factor Asthma | 0 |
| Have Risk Factor COPD | 0 |
| Have Risk Factor Diabetes | 2 |
| Have Risk Factor Hypertension | 1 |
| No Risk Factors | 18 |
| Sleep Apnea | 1 |
Discussion
The COVID-19 pandemic impacts lives in many ways, affecting work, relationships, ability to obtain healthcare and health perception [10]. Thus, there are concerns for populations such as those with CMT as to whether they are at increased risk of contracting COVID-19 and, if they do, whether they are at risk for developing the severe complications of the disease requiring hospitalization and ICU care. Our results do not support an increased risk for patients with CMT to contract COVID-19. They also do not support an increased risk of severe complications from the disease if individuals are infected with SARS-CoV-2. We recognize limitations with our study in that our data comes from individuals we have not examined who have been asked to complete on-line surveys. In fact, we only asked those who had been diagnosed with COVID-19 to respond to the survey, those who died could obviously not have completed the survey. The fact that many (132/153) completed the survey but only around 21 people with CMT actually had acquired COVID simply means that over 100 of the responders had not carefully read the instructions. Therefore, it raises questions about the actual percentages of patients with CMT and COVID-19 which is likely to be much less than the 13% of the CMT population cited here. However, we believe that our results suggest that there is not likely to be an increased risk of acquiring severe cases of COVID-19 for most patients with CMT. In part this is based on the fact that in past queries of our USA and Italian registries there are typically hundreds of patients who rapidly respond to our questionnaires. Thus, we think it unlikely that there were many patients in the registries who had COVID-19 but simply did not complete the questionnaires and that those that did acquire COVID were not more severely affected clinically than people without CMT based on the responses to queries about disease severity. We reasonably conclude that COVID infection is not common in the CMT patient population. Whether there are increased risks for patients with rarer forms of CMT with significant respiratory compromise remains unanswered and will require investigations focusing on these subgroups. We recognize the need for health professionals to increase efforts to carefully follow individuals with CMT to determine which if any CMT subtypes or symptoms are particularly predisposed to develop more severe forms of disease.
Acknowledgements
The authors thank the Inherited Neuropathy Consortium, the Italian CMT Network, Charcot Marie Tooth Association (CMTA), ACMT-Rete per la malattia di Charcot-Marie-Tooth OdV and the Associazione del Registro per le Malattie Neuromuscolari (http://www.registronmd.it/). Research reported in this publication was supported by a grant for the project from the CMTA in addition to funding from the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR002537. MES receives support from the NCATS and the NIH (U54NS065712), NINDS (R21TR003034; U01 NS1094301, R01NS105755), the MDA and the Charcot Marie Tooth Association. RZ, CP and DP are members of the European Reference Network for Rare Neuromuscular Diseases (ERN EURO-NMD). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The Italian CMT Network includes drs. Lucio Santoro, Fiore Manganelli, Stefano Tozza, Gian Maria Fabrizi, Tiziana Cavallaro, Marina Grandis, Stefano C. Previtali, Isabella Allegri, Luca Padua, Costanza Pazzaglia, Aldo Quattrone, Paola Valentino, Massimo Russo, Anna Mazzeo, Giuseppe Vita.
Ethical Publication Statement
We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Author Contributions
Riccardo Zuccarino, study concept and design, analysis and interpretation of data, drafting and critical revision of manuscript for intellectual content Chiara Pisciotta, statistical analysis and interpretation of data, critical revision of manuscript for intellectual content Valeria Prada, statistical analysis and interpretation of data, critical revision of manuscript for intellectual content Filippo Genovese, study concept and design, interpretation of data, critical revision of manuscript for intellectual content Amy Gray, interpretation of data, critical revision of manuscript for intellectual content. Angelo Schenone, study concept and design, analysis and interpretation of data, critical revision of manuscript for intellectual content Davide Pareyson, study concept and design, analysis and interpretation of data, critical revision of manuscript for intellectual content Michael E. Shy, study concept and design, analysis and interpretation of data, critical revision of manuscript for intellectual content
Author Disclosures
None of the authors has any conflict of interest to disclose.
References
- Du W, Yu J, Wang H, Zhang X, Zhang S, et al. (2020) Clinical characteristics of COVID-19 in children compared with adults in Shandong Province, China. Infection 48: 445-452. [crossref]
- Gou FX, Zhang XS, Yao JX, Yu DS, Wei KF, et al. (2020) Epidemiological characteristics of COVID-19 in Gansu province [in Chinese]. Zhonghua Liu Xing Bing Xue Za Zhi 41: E032. [crossref]
- Jeng MJ (2020) COVID-19 in children: current status. J Chin Med Assoc 83: 527-533. https://doi.org/10.1097/JCMA.0000000000000323.
- Wan S, Xiang Y, Fang W, Zheng Y, Li B, et al. (2020) Clinical features and treatment of COVID-19 patients in northeast Chongqing. J Med Virol 92: 797-806. [crossref]
- Zheng Y, Xu H, Yang M, Zeng Y, Chen H, et al. (2020) Epidemiological characteristics and clini- cal features of 32 critical and 67 noncritical cases of COVID-19 in Chengdu. J Clin Virol 127: 104366. [crossref]
- Veerapandiyan A, Wagner KR, Apkon S, McDonald CM, Mathews KD, et al. (2020) The care of patients with Duchenne, Becker, and other muscular dystrophies in the COVID-19 pandemic. Muscle Nerve 62: 41-45. [crossref]
- Reilly MM, Murphy SM, Laura M (2011) Charcot-Marie-Tooth disease. J Periph Nerv Syst 16:1–14.
- Gentile L, Russo M, Fabrizi GM, Taioli F, Ferrarini M, et al. (2020) Charcot-Marie-Tooth disease: experience from a large Italian tertiary neuromuscular center. Neurol Sci 41: 1239-1243. [crossref]
- Veerapandiyan A, Connolly AM, Finkel RS, Arya K, Mathews KD, et al. (2020) Spinal muscular atrophy care in the COVID‐19 pandemic era. Muscle Nerve 62: 46-49. [crossref]
- Prada V, Hamedani M, Genovese F, Zuppa A, Benedetti L, et al. (2020) People with Charcot-Marie-Tooth disease and COVID-19: Impaired physical conditions due to the lockdown. An International cross-sectional survey. Ann Phys Rehabil Med 63: 557-559. [crossref]