Abstract
Tuberculosis still remains one of the significant causes of morbidity and mortality in the globe despite the advances in diagnostic and treatment. In countries with high HIV prevalence like Malawi, the impact of the disease can be largely felt within the health systems. Understanding the demographic and clinical characteristic of diagnosed patients is extremely important for control and prevention of the disease. This present studied described the characteristics of TB patients in a rural district hospital of Malawi. The prevalence of the disease was predominantly higher among males and in the productive age group of 25-44. Affected patients were more likely to be co-infected with HIV and suffer for pulmonary tuberculosis. Majority of the people were newly diagnosed and heavily depended on farming for their day-to-day life. This study, clearly demonstrate that tuberculosis patients are diverse in nature and hence understanding the clinical and demographic determinants of the disease is extremely important for development of effective infection control and prevention programs.
Introduction
Tuberculosis still remains a major public health challenge in Malawi. Even though Malawi adopted the directly observed treatment short course (DOTS) in 1990’s, tuberculosis still remains a major public health threat, affecting thousands of individuals across the country [1]. Its impact can directly be felt in the country, household and individual economy. It still remains a significant cause of morbidity and mortality among people living with HIV. In 2018, The TB mortality among HIV negative people was reported as 11/100,000 population while among HIV positive people was 19/100,000 Population [2]. Just like in other Sub-Saharan Africa countries, Malawi is one of the countries with a high prevalence of HIV (8.9%) [3]. This has exacerbated the situation. Even though the rate of TB HIV co-infection has declined from 77% (2003) to 48.5% in (2018), it still remains high and calls for more public health attention [4].
Due to the magnitude of the problem, Malawi government declared tuberculosis as an emergency in order to raise awareness and advocate for more resources for TB control and prevention. Various stake holders also advocated the integrated HIV/TB care approach in order to reduce the burden of TB among people living with HIV (PLWH). The emergence of multi-drug resistant TB has also raised serious concerns and challenges in the fight against the disease. In 2013 alone, a national drug resistance survey reported a prevalence of 4.8% among retreatment and 0.48% among new patients [4].
As one of the countries with high TB and HIV burden, Malawi needs proper strategies and guidelines as well as health systems strengthening in order to win the fight against this dual burden. Malawi’s vision is to achieve TB and leprosy free Malawi in 2025.Malawi aims at reducing tuberculosis related incidence by 50 % and mortality by 75% by the end of 2025 compared to the 2015 [4]. In order to achieve all these goals, understanding characteristics of patients diagnosed with tuberculosis is important. It gives an insight to the social-demographic determinants of the disease and hence helps the government to properly align resources in the fight against the catastrophe.
While similar study has been done in the urban, Lilongwe Malawi [5], at an HIV/TB integrated clinic, there is still a paucity of data on studies describing the demographic characteristics, including HIV comorbidity, patient occupation, gender etc. within a rural district hospital in Malawi.
Therefore, we aim to fill the gap in literature and complement other studies done in urban setting by describing the characteristics of patients diagnosed with tuberculosis at Nkhotakota district hospital within the central region of Malawi.
Methods
Study Design and Population
This retrospective analysis of all patients diagnosed with TB in 2016 at Nkhotakota district hospital. We used routine data from both TB registers and patient treatment cards collected from January to December in 2016 at Nkhotakota district hospital. All adults and children diagnosed with active TB according to national TB guidelines were eligible for this study.
Setting
The study was conducted at Nkhotakota district hospital within the central region of Malawi. Nkhotakota district hospital is a secondary level of care hospital with the 3-tier health system of Malawi. It has a large catchment area of a population of about 400 thousand and is located along the Lake shore region. Nearly, two-third of its population is below the age of 40 and lives in a rural area.
Data Collection
All demographic data including gender, age, occupation and HIV related information were extracted from HIV and TB registers. All TB related data including TB registration numbers, registration dates, initial sputum microscopy, mode of diagnosis, HIV status (Known positive, negative, unknown), TB type and treatment regimen were also extracted from the registered and entered into an excel sheet. All data, that had part of information missing were excluded from the study.
Data Analysis
The Characteristics of TB patients were analysed by various categories, including age groups, HIV status, TB type, and occupation Categorical measures were presented as percentages and continuous measures were presented as means. Results are presented as percentages. Chi-square test were used for categorical variables. Statistical significance has been defined as P < 0.05.
Results
Of the 179 patients with TB, 107 (60%) were male and 72 (40%) were female. The largest proportion of the patients were between the age of 25-44 (53%) (Figure 1). The average and median age was the same for both males and females (Table 1). Of the 144 cases that were classified in the TB register, majority (80 %) were pulmonary TB while 28 (20 %) were extrapulmonary TB cases. There was no significant difference for TB classification between men and women. More women under hospital Directly Observed Treatment course as compared to men (DOT) than men (Table 2). During the study period, 106 men and 179 women suspected of TB were tested for HIV 56 (53 %) of the men and 90 (50 %) of the women tested had HIV. Majority of the patient already knew their HIV status before being diagnosed with tuberculosis (Table 3). There was no significant month to month differences in the number of diagnosed cases during the study period (Figure 2). Majority of the patients were self-employed, and were involved in either small scale business or farming (Table 4).
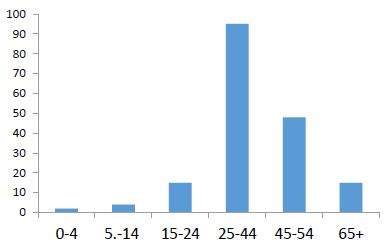
Figure 1: Age distribution among diagnosed TB patients in Nkhotakota (Malawi) in 2016
Table 1: Average and median age distribution among diagnosed TB patients in Nkhotakota (Malawi) in 2016
|
Average (s. dev) |
Median |
|
| Male |
41.6 (14.7) |
40 |
|
Female |
39.9 (15.9) |
38 |
| Total |
40.9 (15.1) |
39 |
Table 2: Distribution of diagnosed TB patients by TB Class, mode of treatment and patient category
|
Category |
Directly observed treatment (DOT) Option | TB Classification |
Patient Category |
|||||
|
Option |
Guardian | Hospital | Pulmonary | Extra Pulmonary | New | Relapse | Fail |
Other |
| Male |
62 |
9 | 53 | 19 | 62 | 6 | 2 | 3 |
|
Female |
38 | 34 | 63 | 9 | 38 | 34 | 63 |
9 |
Table 3: Patient distribution by HIV status and time of HIV test
|
Category |
HIV Test | Time of HIV Test | |||
| Option | Negative | Positive | Unknown | Before Report |
After Report |
| Male |
51 |
56 | 0 | 97 | 9 |
|
Female |
89 | 90 | 0 | 160 |
19 |
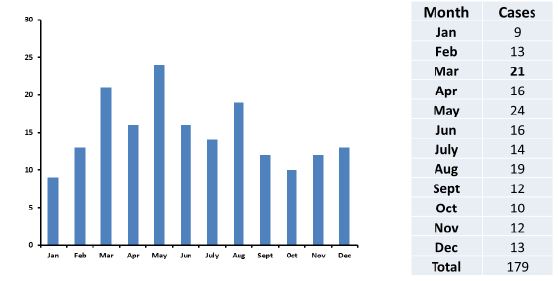
Figure 2: Patient distribution by month of diagnosis
Table 4: Distribution of occupation among TB suspects in Nkhotakota (Malawi) in 2016
| Farmer |
68 |
| Business |
30 |
| Housewife |
20 |
| Fisherman |
10 |
| Student |
9 |
| Teacher |
4 |
| Driver |
4 |
| Retired |
3 |
| Laborer |
3 |
| Drop Out |
2 |
| Health |
2 |
| Other |
12 |
| N/A |
12 |
| Total |
179 |
Discussion
This is one of the studies done in a rural Malawian district to describe the characteristics of patients diagnosed with Tuberculosis. We noted several characteristics of tuberculosis patients that are necessary for patient management. Our study noted that majority of patients were male, and within the productive age group of 25-44. This finding is comparable to a similar study that was done in 2012. This study reported the largest proportion of patients to be between the ages of 25-34 [4]. This demographic distribution is extremely important. This is also the group that is highly hit by HIV with the prevalence ranging as high as 10.5% [3]. HIV weakens the immune system and predispose the affected individual to active tuberculosis disease. Indeed, the rate of HIV/TB co-infection has always been reported to be high in Malawi. In 2013, alone, 56% of tuberculosis patients were reported to have HIV [6]. The socio-economic impact of tuberculosis on this group can also not be undermined. This is the group that is supposed to be economically productive. Our findings also agree with national findings from the national tuberculosis prevalence survey, where majority of patients were males [4].
Our study also reveals majority of the patients have pulmonary tuberculosis. This is also in line with the national data, where nearly 65% of all TB patients had pulmonary TB [4]. The rate of transmission of pulmonary TB is higher as compared to other forms of TB. With the high prevalence, there is a need for strong surveillance systems, to actively trace all contacts and screen them for tuberculosis.
Our present study also demonstrates that majority of our patients had HIV and already knew their status before diagnosis. The timing of HIV diagnosis in relationship to the diagnosis of tuberculosis is important. TB is an opportunistic disease. The coming in of universal ART coverage has led to a decrease in number of notified cases of tuberculosis. If the prevalence of the disease among people living with HIV still remains high, it may be assumed that there is poor adherence to ART. The high levels of TB/HIV co-infection have prompted the government and various stakeholders to call for an integrated TB and HIV program at all levels of care to ensure widespread implementation of interventions which reduce the burden of TB among People Living with HIV (PLHIV) and those which reduce the burden of HIV among notified TB case.
Most of the cases in this study were newly diagnosed and preferred home treatment, especially men. While there were reports of treatment failure, most of the people were successfully treated. Directly observed treatment short course was introduced to ensure strict adherence to TB treatment, thereby reducing the number of cases of drug resistant TB. However, in this present study, only few men preferred hospital treatment. This may be explained by the partially poor health seeking behaviours among men, hence most of them don’t want to return to hospital. When the government declared tuberculosis an emergency in 2007, one of the campaigns was universal access to tuberculosis treatment. As a result of the declaration there have been campaigns to shift from centralized institutional DOTS services to more innovative ways of reaching out to all target population groups with quality assured diagnosis and care regardless of socio-economic status and geographical location [6].
Majority of the patients in this study were farmers, probably owing to the fact that most of them resides in rural areas were, farming forms part of day-to-day life. This is a group that is already economically struggling and living in poor households, with overcrowding conditions. This increases risk of transmission of the disease.
Conclusion
This present study clearly demonstrates that tuberculosis patient varies by age, gender, HIV status and TB Type. If the country is to achieve sustainable development goals and win the fight against HIV and Tuberculosis, there is a need for increased commitment and collaborative action across all stake holders. This also highlights for the need of an operational research within rural district hospitals. The integrated HIV/TB programs should be advocated for and closely monitored for its success. The high prevalence of pulmonary TB (smear positive) also calls for increased effort on infection control, in order to curb the spread of the disease. Lastly, ensuring strict adherence, either by direct observation or family empowerment would be necessary to reduce cases of drug resistant TB.
Declarations
Ethics Approval and Consent to Participate
The study didn’t require full review by the national ethics committee, as there was no direct involvement with patients.
However, a written ethical waiver was provided by the district research and ethics committee and permission was granted by the district medical officer to collect data at the facility. There was no direct involvement with patient.
Consent for Publication
Consent to publish this material was sought from the district health office and it was granted.
Availability of Data and Materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Competing Interests
The authors declare that they have no competing interests
Funding
This study was partly funded by Clinical Research, Education and Management Services Ltd (CREAMS) under the student training package. The funding only covered data collection and analysis.
Acknowledgement
We would like to acknowledge CREAMS for financial help and also, we would like to acknowledge the management of Nkhotakota DHO for their unwavering support.
References
- Global tuberculosis report 2020 [Internet]. [cited 2023 Feb 5]. Available from: https://www.who.int/publications/i/item/9789240013131
- World Health Organization. (2018). Global tuberculosis report 2018. World Health Organization. https://apps.who.int/iris/handle/10665/274453. License: CC BY-NC-SA 3.0 IGO
- Second population survey of HIV in Malawi summary report 2022. [internet]. [cited 2023 Feb 5. Available from: https://phia.icap.columbia.edu.
- Ministry of health of Malawi. National tuberculosis and leprosy control strategic plan 2021-2025. https://shorturl.at/afFK6
- Feldacker C, Tweya H, Keiser O, Weigel R, Kalulu M, et al. (2012) Al Characteristics of adults and children diagnosed with tuberculosis in Lilongwe, Malawi: findings from an integrated HIV/TB clinic. https://doi.org/10.1111/j.1365-3156.2012.03041.x
- National tuberculosis and leprosy control strategic plan 2021-2025 http://nkhokwe.kuhes.ac.mw:8080/handle/20.500.12845/200