The availability and adoption of mobile money services have transformed financial inclusion and service delivery in many developing countries (Donovan, 2012). In Liberia, the immunization program post Ebola Virus Disease (EVD) has faced challenges in efficiently managing financial resources and making timely payments to vaccinators and other health workers, thereby hindering the effectiveness of immunization service delivery. Hence, this mixed- method study was conducted in November 2024 to assess the impact of integrating mobile money payment mechanisms into the financial management system of the Expanded Program on Immunization in Liberia. The review of existing literature suggests that mobile money has the potential to enhance financial inclusion and improve the efficiency of immunization service delivery and other health services in the health sector. Mobile money has been shown to facilitate risk-sharing and promote welfare, though the evidence on its direct economic impact is still limited. (Aron, 2018) The use of mobile money for immunization programs specifically has shown promising results in increasing vaccination coverage through SMS reminders and educational tools for health workers. (Oliver‐Williams et al., 2017). In the case of Liberia, the integration of mobile money into the immunization program’s financial management modalities has helped address the challenges of timely payments and better assurance that payments reach persons for which they are intended, thereby improving health worker motivation and the overall effectiveness of the program. Liberia is dealing with the aftermath of brutal civil wars, the last of which ended in 2003. The infrastructure challenges include poor road infrastructure and underfunded health sector. Gavi, the vaccine alliance is the main funder for routine immunization in the Liberia. An review by the funder’s auditors in 2018 recommended improvements in the financial management systems for the grants at the Ministry of Health. The actions put in place included assurances that payments that MOH/EPI made at community level reached their targeted beficiaries, with timely submission of accountability reports to the center in Monrovia. In 2019, in response to severe economic constraints, the government implemented a salary harmonization exercise which included a cap on personnel recruitments. Subsequently, the development partners provide funding for monthly stipends for recruited health workers.
Highlights from Liberia’s Routine Immunization Program
Despite being one of the world’s least developed countries with low health sector funding, having a health expenditure per capita of $112 in 2021, Liberia immunization coverage for DTP 3 / Penta 3 is 82% (WUENIC 2023 Report) of its targeted population between the ages of 0-23 months by December 2023, from 78% in 2022 thereby recording a percentage increase of 4%. The country relies on the support of international organizations like GAVI, The Vaccine Alliance, USAID, The World Bank, WHO and UNICEF to undertake activities which assure a high immunization coverage. The COVID-19 pandemic affected immunization seeking behaviours because of fear, hesitancy, and mistrust about vaccines, which resulted in a drop in immunization coverage rates for routine vaccines. However, the government of Liberia and its partners were strategic in making a substantial comeback through the development and implementation of an immunization recovery plan, which culminated in increased immunization coverage, as evidenced by the WUENIC 2023 report. It can be recorded that the use of a mobile money payment mechanism for timely and transparent payment of fit-for-purpose immunization workforce (vaccinators and other health workers) was one of the enablers for Liberia’s success in the attainment of 81% fully vaccinated coverage for COVID-19 vaccine. Based on the progress made in increasing the immunization coverage as measured by DTP3 and MCV1, Liberia has been consistent over the past two years with attaining the Millennium Challenge Corporation (MCC) indicator for immunization thereby setting the government on track for obtaining a new MCC Compact.
Trend in Routine Immunization Coverage Despite Low Spending
By 2023, Liberia achieved a notable increase in vaccination coverage. For instance, according to the WUENIC report, the DPT3 vaccine coverage will rise from 65% in 2020 to 82% by 2023. This improvement was largely due to intensified and targeted vaccination efforts (i.e., Outreach, Periodic Intensification of Routine Immunization-PIRI campaigns, etc.), timely payments of remunerations, supportive supervision and the strengthening of the immunization program and, by extension, the health system. Despite these gains, challenges remain, including reaching zero-dose children in remote and underserved areas and maintaining consistent vaccine supply chains. Continued efforts and support from global health partners will be crucial to sustain and further improve immunization coverage in Liberia (Figure 1).
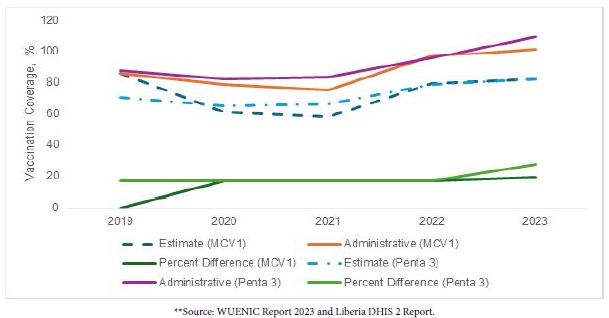
Figure 1: Efforts and support from global health partners.
A Key Lesson on the Use of Mobile Money Payment Mechanism in Enhancing Transparency, Accountability, and Improving Program Performance within the Liberia Expanded Program on Immunization
Mobile money has significantly transformed financial transactions of the Expanded Program on Immunization at the Ministry of Health, Republic of Liberia since its introduction in 2021. The Expanded Program on Immunization entered into contract with the two main mobile telecommunications services providers, MTN Lonestar and Orange. With the contracts, the mobile providers set up payment platforms at the Ministry of Health Office of Finance Management (OFM) and trained users. The EPI and OFM teams conducted a nationwide registration of vaccinators and their particulars including, health facilities assigned, county, names, phone number, and supervisor names. With this information, a payee master list was created and submitted to the mobile providers who validated the names and phone number. With this validated list, the Ministry of Health was able to make periodic payments to health workers. Liberia’s implementation of mobile money and significant advancements in routine vaccination coverage rates exemplify the impact of innovative digital solutions in enhancing the speed and efficiency of financial transactions, as well as in developing customized strategies for expanding coverage and addressing outbreaks of vaccine-preventable diseases. This situation illustrates the substantial outcomes that can be achieved through appropriate innovation and tailored strategies, even in constrained fiscal conditions. The accomplishments of Liberia’s Expanded Program on Immunization can be distilled into seven essential lessons.
National and Subnational Leadership
Based on one of the findings from Gavi’s Audit and Investigation in 2018, Gavi contracted a financial management firm to provide technical support and capacity building to the Expanded Program on Immunization and the Office of Financial Management (OFM). Said recommendation was embraced by the honorable minister and the senior management team of the ministry of health which play a crucial role in the effective implementation of mobile money for immunization programs in Liberia. At the national level, the honourable minister of health, the senior management team of the ministry, the EPI manager, the Office of Financial Management, the internal audit unit, and the compliance unit play pivotal roles in creating policy frameworks that facilitate the adoption and use of mobile money systems by the Expanded Program on Immunization (EPI) and other programs subsequently. This includes providing regulatory support and ensuring that the mobile money payment is secure and accessible to all immunization service providers (e.g., vaccinators and other health workers). For instance, a mobile money steering committee was established and headed by the honourable deputy minister for administration. By promoting public-private partnerships, national leaders encourage investment in mobile money infrastructure and ensure that the technology reaches even the most remote areas, thereby ensuring that other projects and programs adopt said payment mechanisms. At the sub-national level, county health officers, officers-in-charge, and community structures were essential in bridging the gap between national policies and community practices. At the community and health facilities levels, the community development committee and the health facility development committee were charged with the responsibility during their monthly sitting to leverage their close ties with community members in advocating and explaining the use of mobile money in health services, including immunization programs. Working directly with health workers and subnational leaders has helped in the effective implementation of mobile money systems that align with the specific needs and contexts of health facilities and their communities. Moreover, the collaboration between national and subnational leadership is crucial to enhancing the overall effectiveness of mobile money in immunization programs. National leaders can provide the necessary resources and policy support, while subnational leaders ensure that these policies are effectively implemented on the ground. By fostering a coordinated approach, leaders at all levels can address challenges such as technological literacy, network connectivity, and financial inclusion. Strong leadership ensures that the benefits of mobile money are maximized, leading to improved vaccination coverage rates and better health outcomes for the population. A key lesson learned is that strong leadership at the national and sub-national levels through collaborative effort is essential in transforming health service delivery, including immunization, and achieving broader public health goals in Liberia. The successful implementation of mobile money payments within the Expanded Program on Immunization is a glaring demonstration.
Vaccinators’ Satisfaction with Mobile Money Payment
Bringing payment directly to the payees is a transformative digital solution that has been a game changer within the immunization landscape because of its availability and the reduction of bureaucratic bottlenecks and logistics. Out of 252 fit-for-purpose vaccinators interviewed from 252 health facilities across nine counties from northwest, north-central, south-central, and south-eastern Liberia, 63.1% (n=159) said that they were satisfied with the use of the mobile money for immunization transaction which demonstrates increased financial inclusion, especially for those who previously had limited access to traditional banking services due to geographical location and struggle to receive their just remuneration after conducting immunization services. Additionally, they indicated that it has brought a sense of respect and dignity to them within their communities. Table one provides a detailed breakdown of respondents’ reactions to the use of mobile money payment mechanisms for immunization operations. Several key lessons have been learned from mobile money platform use as an innovation in financial management, particularly in Liberia. These lessons include but are not limited to the following (Table 1):
- Challenges associated with traditional banking: The issue of limited banking facilities and long distances due to its geographical location has been eliminated.
- Improve access and convenience: Immunization services have been significantly enhanced, thereby eliminating the need for physical cash transactions and reducing logistical barriers for vaccinators and other health workers working in remote and underserved areas due to the absence of bank access and direct access to cash on the mobile phone.
- Enhanced transparency and accountability in the financial aspects of the immunization program through the provision of digital records for all financial transactions.
- Strengthening trust and engagement between the vaccinators and the This ensures the continuous access and utilization of immunization services by the communities, which is crucial to improving immunization coverage and the larger public health goal of Liberia.
Table 1: How satisfied are you with receiving your payments through mobile money?
| Frequency | Per cent |
Valid Percent |
||
|
Valid |
Very satisfied |
89 |
35.3 | 35.3 |
|
Satisfied |
159 | 63.1 |
63.1 |
|
| Neutral |
4 |
1.6 | 1.6 | |
|
Total |
252 | 100.0 |
100.0 |
|
Transactional Time: How Long Does it Usually Take for Vaccinators to Receive Payment after the Outreach Vaccination Campaign?
Payment of vaccinators for an outreach and/or vaccination campaign can vary widely based on several factors. Ideally, a well- structured mobile money system should be able to effect payment within 24 to 48 hours after the conduct of a health facility outreach and/ or vaccination campaign has ended. However, out of 252 vaccinators interviewed, 54.4% (n=137) stated that they received payments for health facilities outreach within one to two days upon completion. At the same time, 45.6% (n=115) indicated that it takes more than five days. A key lesson learned is that the system is effective to an extent because more than fifty per cent of the participants attest to receiving their payment within one to two days. However, it is noteworthy that there are some situations in which payment may not come so quickly. For instance, administrative inefficiencies, verification processes, loss of network and/or technical issues related to the mobile money platform can further delay the payment period. In some instances, delays for vaccinators might last for days or even weeks to receive the requirements for payment due. Indefinite delays could lead to considerable inconvenience and dissatisfaction among vaccinators, which will negatively impact their morale and the effectiveness of the program. Hence, having a well-structured system for resolving issues in a timely manner will also help to enhance mobile money payments’ reliability and efficiency for this fit-for-purpose immunization workforce and other health workers.
What is Your Overall Experience with Mobile Money Payments Compared to Traditional Payment Methods for Vaccinators?
The use of mobile money platforms as cashless payments has greatly improved the payment process for vaccinators when compared to the traditional system (e.g., hauling cash around) as payments are sent directly to their mobile phones, vaccinators no longer must spend long hours travelling to collect their salary. Out of 252 vaccinators interviewed about their experience with the use of mobile money platforms compared to the traditional system, 59.9% (n=151) indicated that they had a better experience with the use of mobile money as opposed to the traditional system, citing bureaucratic bottlenecks and logistics as major challenges associated with the traditional system as shown in table 2. It was highlighted that mobile money saves time and minimizes the risk involved with transporting cash. Finally, the instantaneous nature of mobile money transactions means that vaccinators are paid quickly, boosting their finances and morale in an immediate fashion. That said, mobile money payments come with their challenges. However, remote areas may experience network issues that could result in delayed transactions, while some vaccinators may not be digitally inclined and thus could face challenges in using mobile money platforms. While mobile money is deemed efficient, some vaccinators expressed concern about abuse and/or other lingering concerns, as the threat of fraud or unauthorized access to accounts is ever-present. Nonetheless, mobile money has generally been a positive change, providing both greater efficiency and greater access over traditional banking and cash-based systems (Table 2).
Table 2: What is the overall experience with mobile money payments compared to traditional payment methods for vaccinators?
|
Frequency |
Per cent | Valid Percent | ||
|
Valid |
Much better |
70 | 27.8 |
27.8 |
| Better |
151 |
59.9 | 59.9 | |
|
About the same |
26 | 10.3 |
10.3 |
|
| Worse |
5 |
2.0 | 2.0 | |
|
Total |
252 | 100.0 |
100.0 |
|
How Would You Rate Challenges Associated with Accessing Payments through Mobile Money Platforms for Immunization Activities?
Out of 252 vaccinators interviewed, the majority (48%, n=121) indicated that accessing mobile money is easy when compared to the traditional system because their incentives and/or salary are paid directly on their mobile phone, meaning that they (e.g., vaccinators) no longer need to journey long distances to collect their wages. This payment method has enhanced the time spent on financial transactions while minimizing the risk of carrying cash. The real- time characteristic of mobile money payments is that vaccinators receive their payments immediately, allowing them greater financial stability – and, with that, motivation. However, there are still issues being faced when using mobile money payments. For instance, network challenges are one of the key challenges highlighted by vaccinators working in rural and underserved areas. Transforming immunization financial landscape using mobile money platforms, however, has been a journey that while positive overall, has not been without some bumps along the way, such as sub-optimal network coverage, therefore it is imperative to have a cross-sectoral approach to improving telecommunications access and digitial payments in the more remote areas of the country (Figure 2).
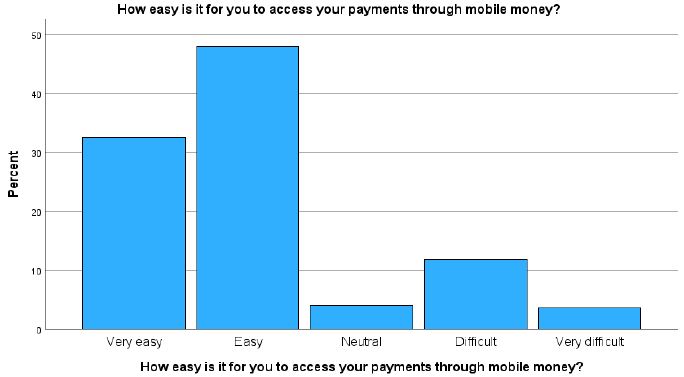
Figure 2: Cross-sectoral approach to improving telecommunications access and digitial payments in the more remote areas of the country.
Leveraging Data, Tracking Performance and Payments, and Course Correction
To ensure efficient immunization spending, data-driven strategies like health facility microplanning, mobile money payment reconciliation, and community profiling have been essential in identifying, monitoring, and improving vaccination efforts. By mapping and profiling communities, the immunization program can develop tailored service delivery interventions to reach zero-dose children, missed children, and underserved communities. This targeted approach allows districts and counties to use health microplanning to pinpoint areas with low vaccination coverage rates effectively. By doing so, their efforts were concentrated on specific areas, enabling them to apply targeted interventions and adjust strategies in real- time. The use of data ensured that no community was overlooked and that corrective measures were both timely and effective. A key lesson learned is that understanding the target population and their locations is crucial to achieving successful immunization outcomes.
Hence, it is imperative to underscore the need for high-quality data to implement targeted interventions effectively. Therefore, investing in data quality is therefore critical for both routine immunization programs, financial decisions, and outbreak response efforts.
Immunization Supply Chain and Logistics Management Information System
In Liberia, the use of mobile money services has significantly enhanced communication on the immunization supply chain and logistics management information system by ensuring the conduct of monthly health facilities outreach and averting potential and/or reducing stockouts of vaccines and vaccine supplies. 70% (n=176) of respondents indicated that with the timely payment of outreach support and monthly incentives, they could transport their vaccines to avoid stockouts and maintain the health facility’s integrity with the communities. A key lesson learned is the importance of local leadership at the health facility level to avert stockouts of vaccines and supplies, especially in hard-to-reach areas, where delivering multiple vaccines is challenging due to geographical accessibility.
Association Between Outreach Payment and Increased DTP3/Penta3 Immunization Coverage
A study was conducted to determine the association between outreach payment and increased DTP3 / Penta3 immunization coverage. Out of 252 vaccinators interviewed, a chi-square test analysis was run to determine the likelihood of an association. However, the findings revealed that a value of 0.282 with 1 degree of freedom (df) and an asymptotic significance (p-value) of 0.595 were observed. This indicates that the observed data are not significantly different from what would be expected under the null hypothesis. Hence, the observed data reveals that there is no association between outreach payment and an increase in DTP3/ Penta 3 coverage (Table 3).
Table 3: Chi-Square Tests
|
Value |
df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) |
Exact Sig. (1-sided) |
|
| Pearson Chi-Square |
.282a |
1 | .595 | ||
|
Continuity Correction |
.141 | 1 |
.708 |
||
| Likelihood Ratio |
.286 |
1 | .593 | ||
|
Fisher’s Exact Test |
.642 |
.357 |
|||
| Linear-by-Linear Association |
.281 |
1 |
.596 |
||
| N of Valid Cases |
252 |