Abstract
A life of an urologist, who thrived in academia after early postgraduate training in the US, was presented. Through this somewhat “game-changing” pathway lessons learned and advices were given for young generation of urologists.
Keywords
Urology, Pathway, Game-changing, Academia
Introduction
My pathway in urology is unusual as described below. The president of Western Society of Japanese Urological Association 2020 meeting (Professor Seichi Saitoh, Ryukyu University) thought this game-changing in a way, and asked me to deliver the lecture based on this life to inspire and advise next generation of urologists. The following is its excerpt.
Early Postgraduate Training:
After medical school Hokkaido University in 1964 and a year of internship I went to the US in 1965. US Educational Commission funded travel grant as a Fulbright scholar. As my internship was not approved in the US I had to take another one and a year of surgery residency in Chicago before eligible for urology program in the US. Hard reality was waiting for this foreign medical graduate with no pulling strings for the well-approved programs. Almost all favored their native sons. Nonetheless I made a tour of interviewing several from mid-west to north-east looking for a glimmering hope. When I received a letter of acceptance from the University of Michigan it was an eureka moment.
Urology training at University of Michigan:
The year 1967 when I started the residency training UM was at the midpoint of century old history [1]. The helm was transiting from Reed M. Nesbit to Jack Lapides. By virtue of happenstance I was lucky to receive training by these two legendary urologists. Dr. Nesbit insisted that he is a clinician and that his close friend and roommate during internship, Nobel Laureate Dr. Charles Huggins, is the true researcher. He knows that basic concept and new ideas could be evolved in the clinic and on the ward without necessity of going to the animal laboratory, which should be volitional and not compulsory [2]. (Fig.1 Reed M. Nesbit (1898~1979) Dr. Lapides always believed that practice of medicine should be based on physiological principle and that unsustainable “facts” should always be questioned. He abhorred simple accumulation of knowledges and insisted on deep thinking or “cerebration” and shrewd skepticism [3]. (Fig.2 Jack Lapides (1914~1995)
Figure 1.
Figure 2.
Under their auspices this neophyte, who knew nothing about urology when he came to UM, grew to a confident one toward the end of residency. If mentors are the ones worthy of gratitude for the warmth vital for the growth, I have no hesitation to name both as my true ones. Appreciating his insight to pick me up as a sole FMG Japanese resident of UM’s long history I wrote a thanking note to Dr. Nesbit just before the completion of residency. His reply came back promptly. (Fig.3 Nesbit’s hand written letter dated May 14, 1970) He described how I served well and consoled me for withstanding hardship of the training. He concluded by stating that “I hope also that you will enjoy the stimulating privilege of training other young men in your field of specialization. That is one of our obligation as well as caring for the afflicted, and also one of the most rewarding that can come to a man.” With these inspiring words (privileges obligation and reward) in my heart as a leading guide I returned to my alma mater HU in 1970.
Figure 3.
An early Academic Life at HU:
Working together with young men at HU became a core activity of early academic life. The following are some from these activities.
Pediatric Urology
1.1 Vesicoureteral reflux: Association of bladder dysfunction (uninhibited bladder) with VUR in children with urinary tract infection was reported very first in the world in 1977 [4], preceding two years ahead of the similar work by Koff and Lapides [5]. When I made an appeal for their mis-stated priority Dr. Lapides was apologetic about Koff’s writing “to be the first” in his reply dated 12/2/79. (Fig.4 Hand-written letter (dated December 2, 1979) from Jack Lapides, Apologizing sentence was encircled in red, and typed out below)
1.2 Disorders of UVJ other than VUR: The role of ureteral sheath in megaureter, be it in refluxing MU or primary MU, was addressed both morphologically and functionally [6]. In view of USh involved in the structure of ureteral hiatus, the role of differences in the hiatus, be it common(C), intermediate (I) and/or separate (S) in duplex anomaly was analyzed [7]. In ectopic ureter this was more relevant than ectopic orifice in associated renal anomaly and also in its surgical management [8]. Duality of USh was confirmed in the study of muscular development of the urinary tract in the human embryo [9].
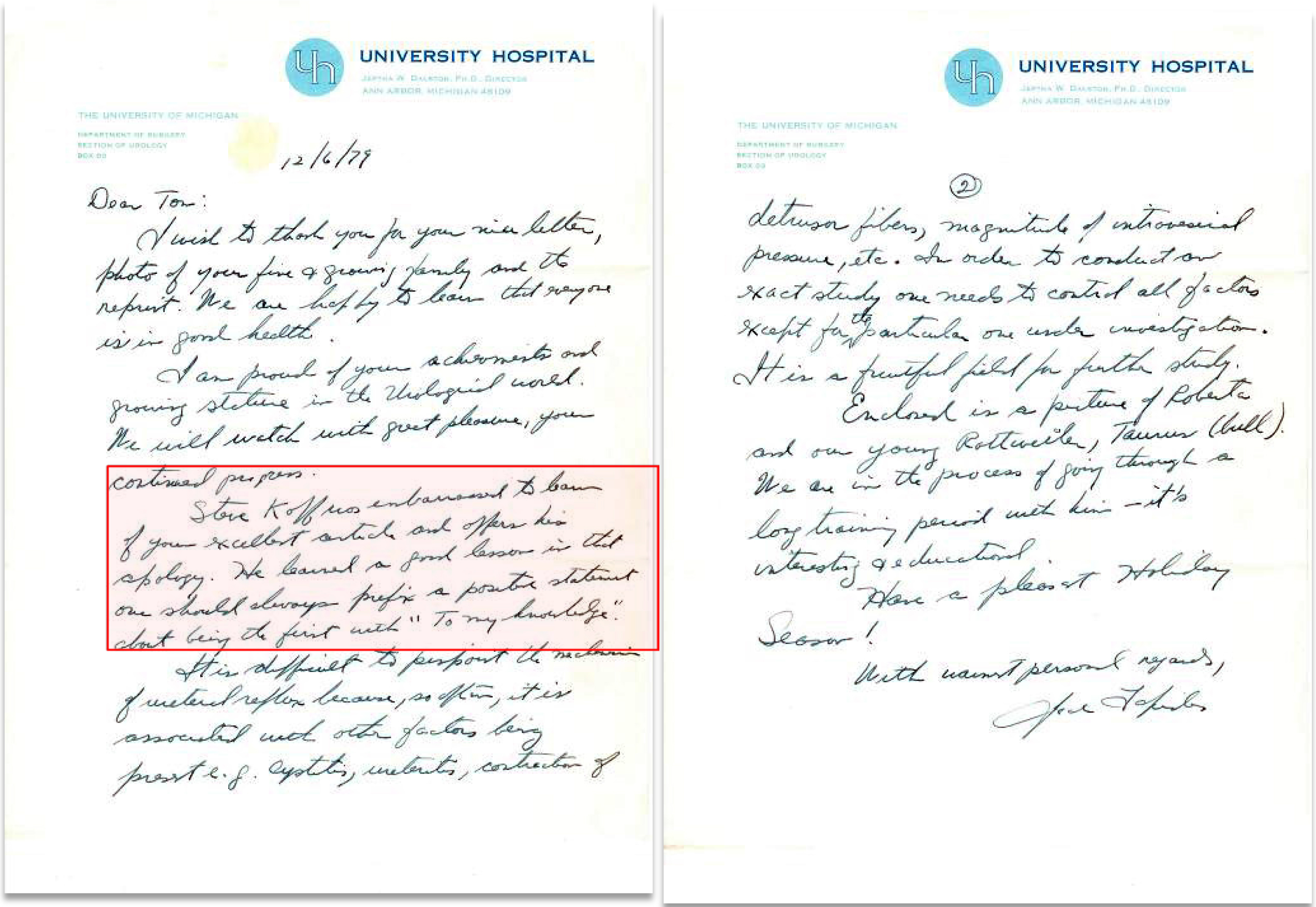
Figure 4.
…Steve Koff was embarrassed to learn of your excellent article and offers his apology. He learned a good lesson in that one should always prefix a positive statement about being the first with “To my knowledge”.…
Neurourology, Urodynamic and BPH
2.1 Sympathetic innervation of the lower urinary tract: In neurogenic bladder the bladder respond supersensitively to para-sympathomimetic, while the urethra not, but rather to sympathomimetic. This is also the very first report of the denervation supersensitivity of the urethra [10]. The mechanism was found to be in the short adnergic system, the activity of which is increased as freed from an inhibitory parasympathetic postganglionic synapse [11] This is the reason for its failure to relax or augmenting activity (DSD) in neurogenic bladder [12]. DS was also confirmed in the refluxing ureter of spinal subjects confirming neural control in the function of UVJ [13]. All these clinical findings are compatible with contemporary basic studies which unfolded intricate innervation pattern of lower urinary tract distinctly different from the traditional one [14, 15].
2.2 Surgical application of neurourology in TURP: TURP is a technique learned at UM. I wanted it not to be a mere operative technique in BPH but also to be applicable in male spinal cord injured. Meanwhile revised concept of the prostate and prostatic urethra was proposed by McNeal [16]. In view of abundant adrenergics in peripheral zone in our study [17] radical TURP by resecting PZ as well was proposed as a manner of surgical sympathectomy to relieve DSD [18]. This surgical application of neurourology in TURP in spinal subjects was a success. Urodynamic confirmations as to relieving voiding dysfunction while not jeopardizing continence were presented [19, 20]. Application of radical TURP in BPH not only yielded high success rate [21], but also shed light on the role of external urethral sphincter [22]. It should be stressed that all these early studies are clinical ones to answer the spectrum of questions from daily practice, literally abiding Nesbit’s admonition. At the same time they exemplify my role as an academic urologist which, I believe, is to bridge basic science and clinical urology.
New Fields in late Academic Life:
In 1982 I was endowed helmsmanship of the department. I focused on two fields to light a way forward. Development of one-stage hypospadias repair (OU) was addressed as ACU lecture on the occasion of 2018 JUA/UAA meeting [23]. The experience in renovacular and renal surgery was presented [24, 25] and addressed as a presidential lecture at JUA meeting in 2000 [26]. Along with reconstructive surgery in kidney transplantation of children [27] stressed that these are the new fields to be tackled by the next generation to make urology a true discipline of surgery.
Lessons and Advices to be heeded:
- Study abroad while young to broaden your scope.
- Pathway is there to be built not to be walked on.
- Seek mentor of your life time.
- Have a healthy skepticism for the dogma.
- Clinical work is demanding as both intellectually and physically as any basic research.
- The role of academic urologist is to bridge the basic science and clinical urology.
- Stay tuned to daily clinical problem where study themes are abundant.
- Publish preferably in leading journals.
- Have working colleagues in the field.
- You did well when surpassed by the young generation. These are the words to be heeded albeit the one from by-gone era.
Summary
Early sojourn to US, urology training at UM, and an academic life at HU were reflected personally. Through these lessons learned and advices were given. I was privileged in that my education and trainings (medical school and US training) were supported by the public fund (Japanese and US government, respectively). Subsequently it was a natural obligation to serve as an academic urologist at HU. It was also rewarding in that I was able to train many next generation of urologists who surpass me both surgically and scientifically. By practicing Nesbit’s admonition (privilege, obligation and reward) I may say the life is well lived.
Abbreviations
JUA- Japanese Urological Association
US- United States
FMG- Foreign Medical Graduate
UM- University of Michigan
HU- Hokkaido University
VUR- Vesicoureteral Reflux
UVJ- Ureterovesical Junction
USh- Ureteral Sheath
MU- Megaureter
DS- Denervation Supersensitivity
TURP- Transurethral Resection of Prostate
DSD- Detrusor Sphincter Dyssynergia
BPH-Benign Prostatic Hypertrophy
OU- One stage Urethroplasty
ACU-Asia Congress of Urology
UAA- Urologic Association of Asia
References
- Konnak JW, Pardanani DS. A history of urology at the University of Michigan 1920–2001 (2002) Historical center for the health sciences monograph series No.7.
- Lapides J, Reed M. Nesbit. His Biography. The University of Michigan Medical Center Journal (1973) 39: 99–100.
- Kogan BA (1990) Jack Lapides Clinician, Teacher, Investigator and Innovator. J Urol 144: 514–516.
- Koyanagi T, Ishikawa T, Tsuji I (1977) Vesicoureteral reflux and uninhibited neurogenic bladder. Int Urol & Nephrol 9: 217–224.
- Koff SA, Lapides J. Piazza DH (1979) Association of urinary tract infection and reflux with uninhibited bladder contractions and voluntary sphincteric obstruction. J Urol 122: 373–376. [crossref]
- Tokunaka S, Koyanagi T (1982) Morphologic study of primary non-reflux megaureters with particular emphasis on the role of the ureteral sheath and ureteral dysplasia. J Urol 128: 399–402. [crossref]
- Koyanagi T, Tsuji I (1979) Experience of complete duplication of the collecting system. Int Urol & Nephrol 11: 27–38.
- Koyanagi T, Hisajima S, Goto T, Tokunaka S, Tsuji I (1980) Everting ureteroceles: Radiographic and endoscopic observation, and surgical management. J Urol 123: 538–543. [crossref]
- Matsuno T,Koyanagi T, Tokunaka S (1984) Muscular development in the urinary tract. J Urol 132: 148–152. [crossref]
- Koyanagi T (1978) Denervation supersensitivity of the urethra to α-adrenergics in the chronic neurogenic bladder. Urol Res 6: 89–93. [crossref]
- Koyanagi T (1979) Further observation on the denervation supersensitivity of the urethra in patients with chronic neurogenic bladder. J Urol 122: 348–351. [crossref]
- Koyanagi T, Arikado K, Takamatsu T, Tsuji I (1982) Relevance of sympathetic dyssynergia in the region of external urethral sphincter: Possible mechanism of voiding dysfunction in the absence of somatic sphincter dyssynergia. J Urol 127: 277–282. [crossref]
- Koyanagi T, Tsuji I (1981) Study of ureteral reflux in neurogenic dysfunction of the bladder: The concept of neurogenic ureter and the role of periureteral sheath in the genesis of reflux and supersensitive response to autonomic drugs. J Urol 126: 210–217. [crossref]
- Elbadawi A (1982) Neuromorphologic basis of vesicourethral function: Histochemistry, ultrastructure, and function of intrinsic nerves of the bladder and urethra. Neurourol & Urodyn 1: 3–50.
- Norlen LJ (1982) Influence of sympathetic nervous system on the lower urinary tract and its clinical implications. Neurourol & Urodyn 1: 129–148.
- McNeal JE (1972) The prostate and prostatic urethra: A morphologic synthesis. J Urol 107: 1008–1016. [crossref]
- Kobayashi S, Demura T, Nonomura K, Koyanagi T (1991) Autoradiographic localization of the adrenoceptors in human prostate: Special reference to zonal difference. J Urol 146: 887–890. [crossref]
- Koyanagi T, Arikado K, Tsuji I (1981) Radical transurethral resection of the prostate for neurogenic dysfunction of the bladder in male paraplegics. J Urol 125: 521–527. [crossref]
- Koyanagi T, Morita H et al. (1987) Radial transurethral resections of the prostate in male paraplegics revisited: Further clinical experience and urodynamics considerations for its effectiveness. J Urol 137: 72–76.
- Shinno Y, Koyanagi T, Kakizaki H, Kobayashi S, Ameda K et al. (1994) Urinary Control after radical transurethral resection of the prostate in male paraplegics: Urodynamic evaluation of its effectiveness in relieving incontinence. Int J Urol 1: 78–84. [crossref]
- Machino R, Kakizaki H, Ameda K, Shibata T, Tanaka H et al. ( 2002) Detrusor instability with equivocal obstruction: A predictor of unfavorable symptomatic outcomes after transurethral prostatectomy. Neurourol & Urodynamics 21: 444–449. [crossref]
- Koyanagi T (1980) Studies of the sphincteric system located distally in the urethra: The external urethral sphincter revisited. J Urol 124: 400–406. [crossref]
- Koyanagi T (2018) ACU lecture: One-stage hypospadias repair- Future is Asia the East. Int J Urol 25: 314–317. [crossref]
- Seki T, Koyanagi T, Togashi M, Chikaraishi T, Tanda K et al (1997) Experience with revascularizing renal artery aneurysms: Is it feasible and worth attempting? J Urol 158: 357–362. [crossref]
- Nobuo Shinohara, Katsuya Nonomura, Tohru Harabayashi, Masaki Togashi, Satoshi Nagamori et al. (1995) Nephron sparing surgery for renal cell carcinoma in von Hippel Lindau disease. J Urol 154: 2016–2019.
- Koyanagi T, Nonomura K, Takeuchi I, Watarai Y, Seki T et al. (2002) Surgery for renovascular diseases: A single center experience in revascularizing renal artery stenosis and aneurysm. Urol Int 68: 24–31. [crossref]
- Chikaraishi T, Nonomura K, Kakizaki H, Seki T, Morita K et al. (1998) Kidney transplamtation in patients with neurovesical dysfunction. Int J Urol 5: 428–435. [crossref]