The availability of thoracic ultrasonography (TUS) for the diagnosis of pulmonary infarct was demonstrated more than 15 years ago [1]. With so, the typical TUS aspect of the embolic lesion remain largely unknown by physicians that otherwise use this tool in an every-day basis. More than two triangular or rounded hypo-echogenic areas bigger than 5 mm, occasionally accompanied by small pleural effusion are suggested TUS criteria for pulmonary infarct diagnosis [2]. Computed tomography angiography (CTA) is the gold standard for the diagnosis [3].
The ultrasonographic aspect of pulmonary embolism is shown here correlating to the accompanied computed tomography of the same lesion.
A 28-year-old man, affected by Smith-Lemli-Opitz syndrome, was admitted to the intensive care unit because of a severe respiratory failure and hemodynamic shock requiring mechanical ventilation and vasopressors. Two weeks before admission, ambulatory antibiotic treatment was started for suspected pneumonia. The CTA study (Panel A) shows multiple pulmonary infarcts on both lungs (arrows). TUS examination (Panel B) of the right thorax shows the corresponding sonogram image for the tomography finding (arrowhead).
Multiple sub-pleural lesion occupied the entire space between two ribs. The lung parenchyma behind the lesion is hyperechoic and shows typical B lines of interstitial lung (small arrows). The central hyperechogenic rounded image at the ultrasonography matches the hypodense rounded bronchi (black arrows) at the CTA. The limit between the hypo-echogenic area and the surrounding lungs is shattered. A deeper bronchial reflex with air-flow Doppler signal can be seen at times when the lung tissue becomes consolidated [4].
Thrombotic occlusion of the right peroneal vein and posterior tibial vein found at duplex ultrasonography was the source of the embolism.
The patient condition responded to heparin treatment.
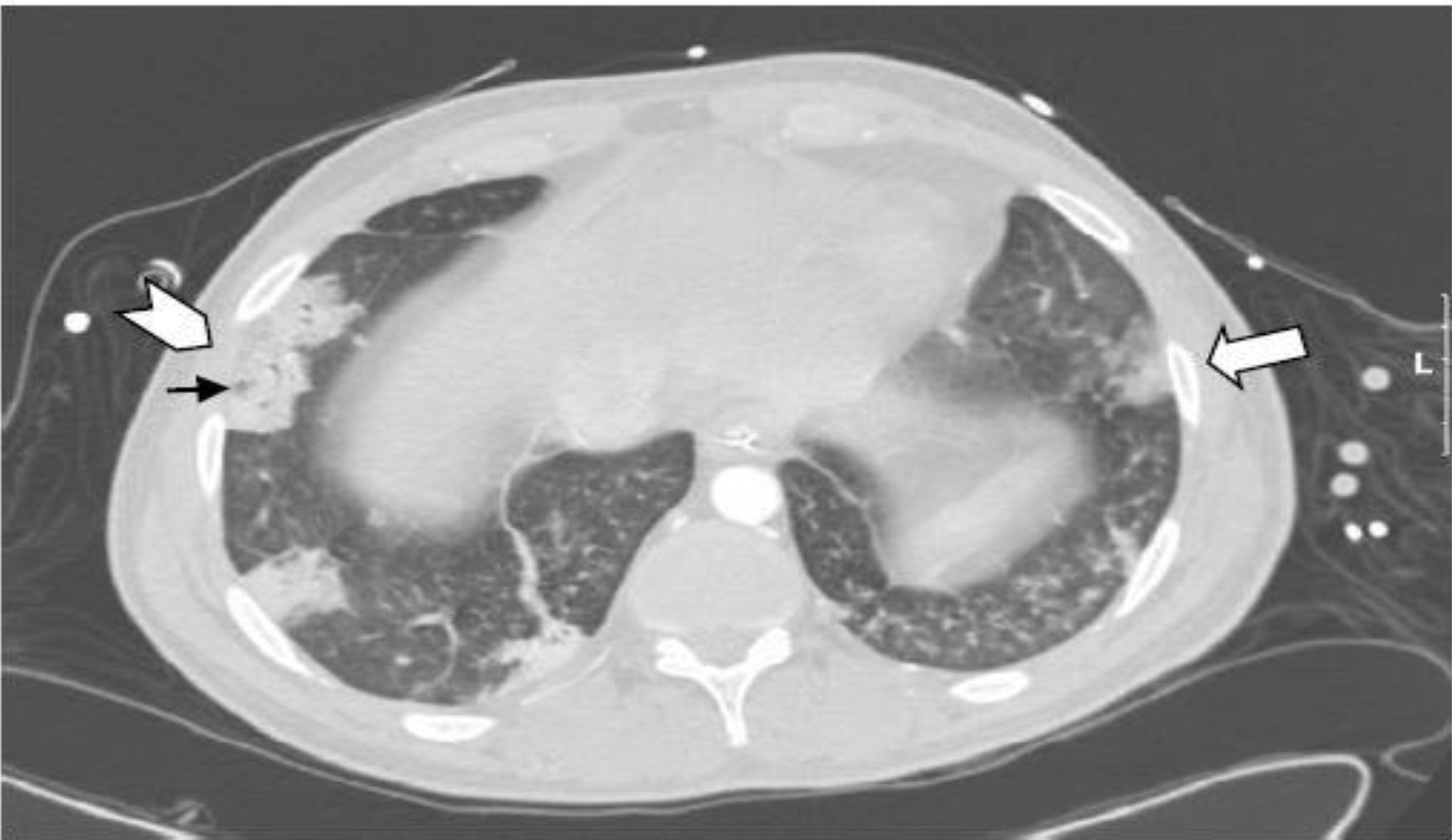
Panel A. Computed Tomography image.
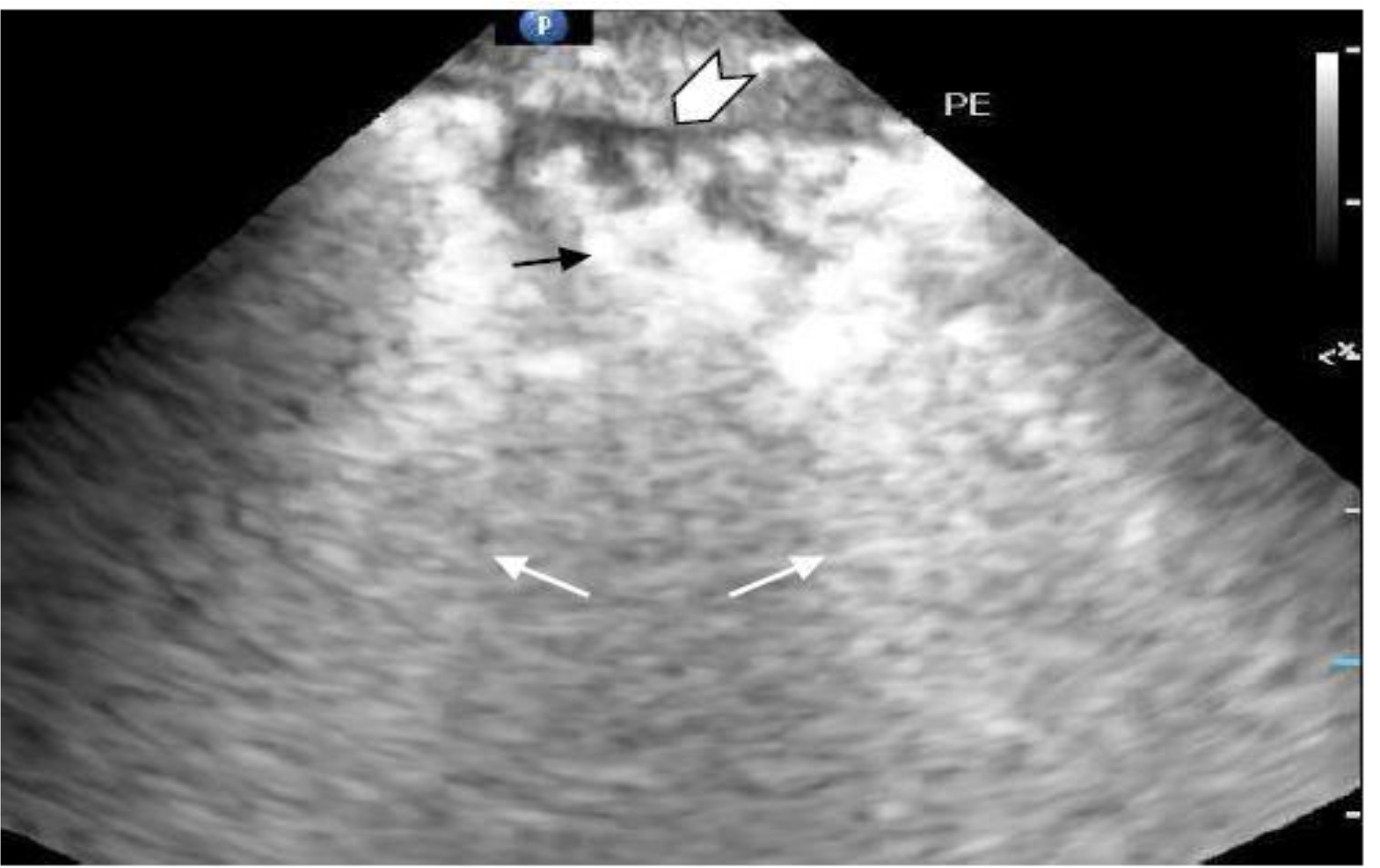
Panel B. Ultrasound image.
References
- Mathis G, Wolfgang B, Reissig A, et al. (2005) Thoracic ultrasound for diagnosing pulmonary embolism: a prospective multicenter study of 352 patients. Chest 128: 1531–1538.
- Reissing A, Heyne JP, Kroegel C (2001) Sonography of lung and pleura in pulmonary embolism: sonomorphologic characterization and comparison with spiral CT scanning. Chest 120: 1977–1983.
- RathbunSW, Raskob GE, Whitsett L. (2000) Sensitivity and specificity of helical computed tomography in the diagnosis of pulmonary embolism: a systematic review. Ann Intern Med 132: 227–232.
- Blancas R, Ballesteros-Ortega D, Martinez-Gonzales O (2018) Central bronchial reflex finding in pulmonary infarct. Med Intensiva 42: 69.