In the paper “Neuroinflammation and osteomyelitis in adults with Type 2 diabetes mellitus and peripheral neuropathy without and with foot lesions. What comes first?” published in September 2025 [1], diabetic foot disease, the leading causes of major and minor non-traumatic amputation worldwide, was originally described as a destructive, progressive bone tissue process beginning from perypheral nerve functional damage (Figure 1a-f, see main paper inn ref. [1]). An innovative framework was proposed, in which chronic oxidative stress, induced by hyperglycemia, may trigger epigenetically mediated adverse neuronal signals as proNGF expression in post-mitotic cells. This neuronal injury could initiate a domino-like cascade involving innervated peripheral tissues leading to neuro-ischemic gangrene or infected necrosis, remembering different tissue damages as myocardial heart failure, diabetic retinopathy and end-stage renal disease where similar irreversible behaviors could share convergent pathogenic mechanisms.
In the paper “Neuroinflammation and Osteomyelitis in Adults with Type 2 Diabetes Mellitus and Peripheral Neuropathy Without and With Foot Lesions. What Comes First?” published in September 20251 , diabetic foot disease—the leading cause of major and minor non-traumatic amputations worldwide—was originally described as a progressive, destructive bone tissue process that begins with peripheral nerve functional damage (Figure 1 a–f, see main paper1). The authors propose an innovative framework in which chronic oxidative stress induced by hyperglycemia may trigger epigenetically mediated adverse neuronal signaling, such as proNGF expression in post-mitotic cells. This neuronal injury could initiate a domino-like cascade affecting innervated peripheral tissues, ultimately leading to neuro-ischemic gangrene or infected necrosis. This process resembles other tissue injuries observed in conditions such as myocardial heart failure, diabetic retinopathy, and end-stage renal disease, where similar irreversible changes may share convergent pathogenic mechanisms.
The updated definition for diabetes-related foot disease proposed by the International Working Group on the Diabetic Foot (IWGDF, 2023 update) [2] describes it as a “disease of the foot of a person with current or previously diagnosed diabetes mellitus that includes one or more of the following: peripheral neuropathy, peripheral artery disease, infection, ulcer(s), neuro‐osteoarthropathy, gangrene, or amputation”. This statement reads more as an updated descriptive framework than a definition, because it describes coexisting or concomitant events and does not illustrate a progression or a prognosis of the phenomenon. Our hypothesis was that hyperglycemia alters the mitochondrial milieu and triggers danger-associated neurotrasmission signals capable of affecting both central and peripheral neuronal function. In particular, distal sensory and autonomic neuropathy could activate neuroischemic and endothelial signaling pathways, inflammatory responses and induce bone cell apoptosis, thereby exposing coating tissues to fatal damage prone to infections (Figure 1).
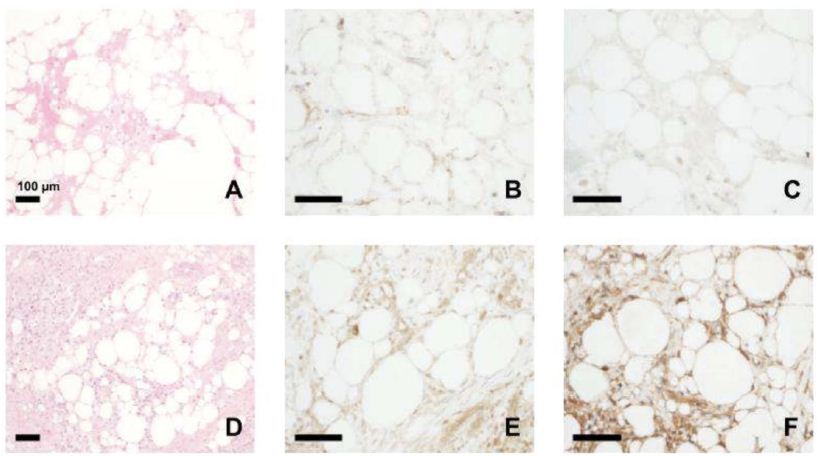
Figure 1: Hematoxylin/eosin staining and CX3CL1 and RORɣ imunohistochimic change expression in femoral head controls (a-c) versus foot bone of diabetic patients with HIOM (d-f). Magnification for A and B 200X, for B-E 400X (Figure 6 [1]).
Based on this hypothesis, we tried to identify an early marker of the phenomenon. Fractalkine (CX3CL1), a constitutively expressed transmembrane chemokine with different neurovascular distribution and unique cleavage-dependent signaling properties, emerged as a candidate [3]. Elevated expression of both the membrane-bound and soluble forms [4] of CX3CL1 has been shown to enhance fractalkine receptor (CX3CR1)-mediated recruitment of inflammatory cells, promote vascular endothelial dedifferentiation, and contribute to tissue fibrosis in non-obstructive vascular diseases. The spread of neuroinflammatory signals throughout peripheral innervated tissues can ultimately converge cytotoxic and apoptotic pathways, leading to irreversible damage in the foot.
It was described that CX3CR1 expression has an important role in early activation of endothelial and peri-endothelial cells both involved in ostructive and non obstructive coronary diseases [4]. In vitro studies have demonstrated that CX3CL1 is not only an endothelial chemokine and a monocyte adhesion molecule, but also acts as a dysfunctional endothelial trigger by promoting the production of reactive oxygen species (ROS), which leads to reduced nitric oxide (NO) bioavailability in vascular smooth muscle cells [4]. Experimental peripheral nerve injuries demonstrated the presence of Fractalkine/CX3CR1 axis beetween neuron and activated glia where clivating enzimes deliver soluble fractalkine for axonal preservation and vascular regeneration [5]. In our neuropathic patients, analysis of bone proteins involved in signal transduction pathways revealed a prominent reduction in ERK1/2 activating phosphorylation (P-ERK1/2) in bone tissue rich of fractalkine, accompanied by increased Akt activation (P-Akt) (See main paper [1] Figure 8C), supporting the hypothesis of a contributory role in the apoptotic cascade. These findings raise a critical question: what is the impact of reduced intraneuronal activity on peripheral nerve function and the integrity of innervated tissues?
In our paper, we reported data of 374 adults with Type 2 diabetes mellitus (T2DM) and diabetic neuropathy (DN) divided into progressive, at risk, or with established foot damage subgroups: 106 neuroparthic subjects without foot lesions (DNp); 119 non-macrovascular neuropathic subjects with ulcers/lesions/osteomyelitis (DNpU); 149 revascularized neuropathic subjects with ulcers/lesions/osteomyelitis (DNpUV) and a group of 53 healthy adults as normal control (NC). We performed biopsy specimens from exposed bone (grade III University of Texas wound classification, TUC) to obtain microbiological standards and histological analysis. Based on TUC classification which defines from stage I (dermal) to stage III (bone) the ulcer depth, we correlated CX3CL1 migration marker with EMG parameters of neuropathy and analyzed pro/anti-inflammatory cytokines, blood cells subsets (lymphocytes subpopulations, classical, non-classical and SLAN+ monocytes, classical DCs, innate lymphoid cells), Nerve Growth Factor (NGF) species, autophagy markers (Ulk1, Beclin1, LC3, and p62), pro/anti-apoptotic proteins (Bax, Bcl2, cleaved Caspase-3) and signal transduction proteins involved in inflammation and cell survival (p65-NF-kB, Akt and ERK1/2). Our results are interesting puzzle pieces in diabetic foot labyrinth. Electrophysiological parameters as Sural nerve (sS) conduction velocity (CV) and sensory Action Potential (sAP) thresholds confirmed the presence and severity of diabetic neuropathy. Worsening in neuronal function was correlated with depth of foot lesions, with or without peripheral critical ischemia and increased immature neurokine NGF (proNGF) circulating levels. Furthermore, we found higher numbers of SLAN+ monocytes co-expressing CX3CR1 in all TUC III versus I TUC groups; these inflammatory cells directly correlated with proNGF levels and worsened autonomic and sensory testing. All bone lesions were positive for CX3CL1 and RORɣ (lymphoid marker) in our immunohistochemical analysis1; in the same bone biopsies, sympathetic TH-positive nerves resulted positive by immunofluorescence for the co-expression of CX3CL1 and NGF receptors (p75, TrkA receptors; see main paper Figure 7 in [1]).
Finally, bone cleaved caspase 3 and Bax directly correlated with % of CX3CR1+SLAN+CD16+ inflammatory monocytes and inversely with bone ERK1/2 activating phosphorylation. Multiple RNA array sub-analysis confirmed potential impairments in autophagy and upregulated mTOR/RHEB apoptotic signaling co-expressed with CX3CR1 on bone species (see main paper [1] Figure 9C-E).
Collectively, these findings indicate that diabetic neuropathy represents a primary pathogenic driver in diabetic foot disease, triggering a domino-like neuroinflammatory process. Loss of sensitive function and autonomic dysregulation appear to compromise foot integrity, alter intrabone neurotrophins and CX3CL1 expression and induce vascular dysfunction, early bone apoptosis and CX3CR1+monocytes chemotaxis preceding and potentially occurring independently of infected osteomyelitis. These data redefine the hierarchy of pathogenic events in diabetic foot disease and may mark the way for the development of new targeted therapies.
Abbreviations
BAX: Bcl2 Associated X Protein; Bcl2: B-Cell Lymphoma 2; CD: Cluster Differentiation; CV: Conduction Velocity; CX3CL1: Chemokine (C-X3-C Motif) Ligand 1; CX3CR1: C-X3-C Motif Chemokine Receptor 1; DC: Dendritic Cell; DN: Diabetic Neuropathy; EMG: Electromyography; ERK1/2: Extracellular Signal-Regulated Kinase; HIOM: High Infected Osteomyelitis; IWGDF International Working Group on the Diabetic Foot; LC3: Microtubule-Associated Protein 1A/1B-Light Chain 3; mAP/sAP: Motor/Sensory Action Potential; MIOM: Mild Infected Osteomyelitis; m/proNGF: Mature/Immature Nerve Growth Factor; mTOR: Mechanistic Target of Rapamycin; NC: Normal Control; nDFH: Non-Diabetic Femur Head; NF-kB: Nuclear Factor Kappa-light-chain-enhancer of Activated B Cells; nILOM: Non Infected Low Osteomyelitis; NGF: Nerve Growth Factor; NK: Natural Killer Cell; NO: Nitric Oxide; p75 NTR p75 Neurotrophic Receptor; PA: Plasminogen Activation; PB: Peripheral Blood; RHEB: Ras Homolog Enriched in Brain; ROS: Reactive Oxygen Species; ROR𝛾: RAR-related Orphan Receptor Gamma; SLAN: 6-sulfo LacNAc; ; sS: Sural; sSa: Saphenous; sSP: Superficial Peroneal; T2DM: Type 2 Diabetes Mellitus; TH: Tyrosin Hydroxilase; TrkA: Tropomyosin Receptor Kinase A; TUC: University of Texas Wound Classification; Ulk1: Unc-51 Like Autophagy Activating Kinase 1.
Keywords
Diabetic foot, Neuropathy, Osteomyelitis, Fractalkine CXC3L1/CXC3R1 axis
References
- Sambataro M, Sambado L, Colardo M, Furlan A, Stefani PM, Durante E, Antico A, Conte S, Bella SD, Nollino L, Barbara Z, Menegotto N, Vian E, Segatto M, Fassan M (2025) Neuroinflammation and osteomyelitis in adults with Type 2 diabetes mellitus and peripheral neuropathy without and with foot lesions What comes first? J Diabetes Complications. [crossref]
- Schaper NC, van Netten JJ, Apelqvist J, Bus SA, Fitridge R, Game F, Monteiro-Soares M, Senneville E (2024) Practical guidelines on the prevention and management of diabetes-related foot disease IWGDF 2023 update. Diabetes Metab Res Rev. [crossref]
- Umehara H, Bloom ET, Okazaki T, Nagano Y, Yoshie O, Imai T (2004) Fractalkine in vascular biology from basic research to clinical disease. Arterioscler Thromb Vasc Biol. [crossref]
- Stangret A, Sadowski KA, Jabłoński K, Kochman J, Opolski G, Grabowski M, Tomaniak M (2024) Chemokine Fractalkine and Non-Obstructive Coronary Artery Disease-Is There a Link? Int J Mol Sci. [crossref]
- Pottorf TS, Rotterman TM, McCallum WM, Haley-Johnson ZA, Alvarez FJ (2022) The Role of Microglia in Neuroinflammation of the Spinal Cord after Peripheral Nerve Injury. Cells. [crossref]