An 86-year-old man presented to his cardiologist for regular follow up with chest pain and exertional intolerance with tachycardia and palpitations. The patient had further medical history of paroxysmal atrial fibrillation, chronic back pain with cement vertebroplasty, ischaemic heart disease with previous multivessel coronary stenting, hypertension, hypercholesterolaemia, type two diabetes mellitus, stage four diabetic kidney disease and previous upper GI bleed whilst on dual antiplatelets. His medications were apixaban 2.5 mg BD, metoprolol 25 mg BD, digoxin 62.5 mcg daily, irbesartan 300 mg daily, lercanidipine 10 mg daily, atorvastatin 40 mg daily, dapagliflozin 10 mg daily, metformin 1 g daily and pantoprazole 40 mg daily.
ECG showed atrial fibrillation with a heart rate of 57 bpm and no ischaemic changes. Subsequent Holter monitor showed atrial fibrillation throughout with a minimum heart rate of 41 and maximum of 141. Transthoracic echocardiogram showed normal left ventricular size and function with stable mild valvular disease.
The patient described his symptoms as being like a previous presentation which led to a diagnosis of obstructive left main coronary artery disease. The patient underwent invasive coronary angiography which illustrated only moderate non obstructive coronary artery disease with patent stents. There was the unexpected finding of radio-opaque masses in the right atrial appendage and the right ventricle. This was associated with new T12 cement vertebroplasty (Figure 1).

Figure 1: Coronary angiogram showing two radio-opaque masses in the right atrial appendage and the right ventricle.
Upon review of previous imaging, the radio opaque masses were not present on chest X-rays from prior to vertebroplasty but appeared on X-ray following vertebroplasty. A non-contrast CT chest confirmed the presence of high attenuation material in the right atrial appendage (Figure 2) and inferior right ventricle (Figure 3) and bone cement in the thoracic vertebrae that had extravasated to the region of the paravertebral venous plexus (Figure 4). This was consistent with cardiac embolism of vertebral bone cement.
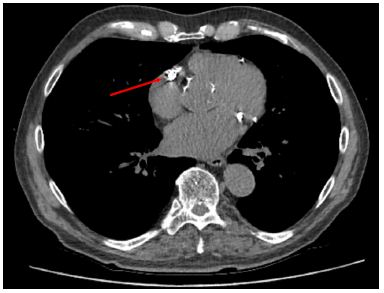
Figure 2: Axial view of CT chest showing high attenuation material in the right atrial appendage.
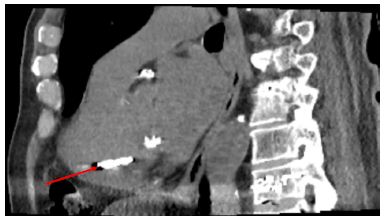
Figure 3: Sagittal view of CT chest showing high attenuation material in the inferior right ventricle.

Figure 4: Sagittal view of CT chest showing cement in T12 vertebral body, extravasating into the paravertebral region.
Retrospective review of previous transthoracic echocardiogram showed a calcified area noted in the right ventricle near the moderator band and another in the right atrial appendage (Figure 5).

Figure 5: Transthoracic echocardiogram illustrating a bright, calcified area in the right ventricle.
The case was discussed at a cardiology multidisciplinary team meeting regarding invasive or medical management due to the risk of cement embolism erosion. The consensus was to manage the case conservatively with anticoagulation to prevent thrombus formation on the cement as the patient had not had any complications of the embolism to date and due to his advanced age and comorbidities. The patient’s apixaban was increased to 5 mg BD and his symptoms remained stable.
Discussion
Percutaneous vertebroplasty is used to treat osteoporotic fractures to reduce pain and provide stability to the spine [1]. The procedure involves injecting polymethylmethacrylate (PMMA) cement into the diseased vertebrae and the main risks are associated with the leakage of cement into the surrounding structures. With absorption into the iliolumbar and epidural veins, the cement can gain access to the central circulation.
The rate of extravasation into central veins during this procedure is estimated at 23% however usually particles of cement are small, and the patient remains asymptomatic. Symptomatic intracardiac embolism is estimated to occur in only 0.3% of cases [2]. Sequelae of embolism can involve arrhythmia, valve dysfunction, pulmonary embolism and rarely cardiac perforation resulting in tamponade.
If the suspicion for intracardiac cement embolism (ICE) is high, CT chest and TTE should be performed to confirm the diagnosis, location of the embolism and to assess for complications. The bone cement is high attenuation and has been described as 373-1600 Hounsfield units when embolised to the heart [3]. However as seen in this case other modalities including chest X ray and fluoroscopy can make the diagnosis.
Risk factors for embolism include higher number of segments, injection into the thoracic vertebrae, tumour related fractures, higher amounts of bone cement used and lower viscosity cement [4].
Prevention of ICE includes the use of high viscosity cement to reduce extravasation, avoiding over pressurisation and injecting under fluoroscopy to assess for embolization during the procedure [5].
Recommendation on management of ICE depends on the patient’s status. In asymptomatic patients, observation without intervention is most appropriate. Small cement emboli routinely do not cause symptoms so routine post procedural imagining is not recommended.
Symptomatic patients may require intervention. Patients with cardiac rupture and tamponade require urgent surgical intervention to remove the fragment and repair the myocardial defect. There have been case reports of percutaneous removal of fragments that are amenable to do so that are either high risk of causing cardiac rupture or impinging on the tricuspid valve apparatus [5].
References
- Jay B, Ahn SH (2013) Vertebroplasty. Semin Intervent Radiol. [crossref]
- Kim YJ, Lee JW, Park KW, Yeom JS, Jeong HS, Park JM, Kang HS (2009) Pulmonary cement embolism after percutaneous vertebroplasty in osteoporotic vertebral compression fractures incidence characteristics and risk factors. Radiology. [crossref]
- Oshinsky C, Bhavani S, Funaki A (2018) Cement cardiac embolism following kyphoplasty noted on thoracic imaging. Radiol Case Rep. [crossref]
- Wang L, Lu M, Zhang X, Zhao Z, Li X, Liu T, Xu L, Yu S (2023) Risk factors for pulmonary cement embolism after percutaneous vertebroplasty and radiofrequency ablation for spinal metastases. Front Oncol. [crossref]
- Zhao Z, Wang R, Gao L et al. (2024) Pulmonary embolism and intracardiac foreign bodies caused by bone cement leakage a case report and literature review. J Cardiothorac Surg. [crossref]