Abstract
Psychological insulin resistance (PIR) constitutes a significant barrier to achieving timely insulin initiation among adults living with type 2 diabetes mellitus (T2DM). This study utilizes structural equation modeling (SEM) to explore the influence of self-efficacy, social support, diabetes distress, and diabetes stigma on PIR. A cross-sectional survey of 289 T2DM patients demonstrated that PIR is shaped by complex emotional and sociocultural pathways. High self-efficacy and strong social support reduce insulin hesitancy, whereas elevated distress and stigma significantly intensify reluctance toward insulin therapy. These findings provide important guidance for developing psychosocial interventions aimed at improving insulin uptake and long-term glycemic outcomes.
Keywords
Insulin reluctance, Self-efficacy, Diabetes distress, T2DM, China, SEM
Introduction
Type 2 diabetes mellitus (T2DM) is a rapidly escalating public health challenge in China, with the country representing the largest diabetic population globally. Despite therapeutic advancements, maintaining glycemic control remains difficult for many individuals due to progressive β-cell dysfunction. Insulin therapy is often required as the disease advances; however, psychological insulin resistance (PIR) frequently delays the transition to insulin. PIR refers to a complex spectrum of emotional fears, misconceptions, perceived burdens, stigma, and cultural beliefs surrounding insulin therapy.
In China, sociocultural dynamics play a profound role in shaping patient perceptions of insulin therapy. Many individuals view insulin as an indicator of treatment failure or severe disease progression. Fear of injections, hypoglycemia, lifestyle disruption, dependency, and judgment from others further heighten psychological resistance. The collectivist nature of Chinese society places significant influence on family beliefs, which can either support or hinder insulin acceptance. Additionally, limited diabetes education and inadequate emotional counseling exacerbate misunderstandings about insulin, reinforcing PIR [1].
Existing research highlights key psychosocial determinants of PIR, including self-efficacy, social support, diabetes distress, and diabetes stigma. Individuals with high self-efficacy exhibit stronger confidence in diabetes self-management and are more open to initiating insulin [2]. Social support provides emotional and practical assistance, buffering anxiety associated with insulin therapy. In contrast, elevated diabetes distress increases emotional burden and avoidance behaviors, while stigma contributes to internalized shame and negative self-perception. Few studies, however, have examined these factors within a unified analytical framework in Chinese populations.
Structural equation modeling (SEM) offers a comprehensive statistical method for examining direct and indirect effects across multiple interrelated psychosocial constructs. This study aims to employ SEM to explore how self-efficacy, social support, distress, and stigma interact to shape PIR among Chinese adults with T2DM [3]. Understanding these pathways is crucial for designing culturally sensitive interventions to reduce PIR and facilitate timely insulin initiation.
Methods
Study Design and Setting
This cross-sectional study was carried out between March and September 2023 in the Endocrinology Department of a tertiary teaching hospital in Anhui Province, China. The hospital serves as a major referral center for diabetes management, providing access to a large and diverse patient population. Ethical approval was obtained from the institutional review board prior to study commencement.
Sampling and Recruitment
A convenience sampling method was used to recruit adults attending outpatient diabetes clinics. Inclusion criteria were: age ≥18 years, confirmed diagnosis of T2DM for at least one year, and ability to independently complete questionnaires. Patients with severe psychiatric illness, cognitive impairment, terminal illness, or short-term insulin use for acute conditions were excluded. A total of 289 participants met eligibility criteria and completed the study.
Data Collection Procedures
Written informed consent was obtained from all participants. Trained research assistants supervised questionnaire completion, ensuring accuracy and minimizing missing data. Clinical information including HbA1c levels, treatment regimens, and diabetes duration was extracted from electronic medical records [4].
Measures
Participants completed validated Chinese versions of the following instruments: the Psychological Insulin Resistance Scale (PIR), the Diabetes Management Self-Efficacy Scale, the Multidimensional Scale of Perceived Social Support (MSPSS), the Diabetes Distress Scale (DDS-17), and the Type 2 Diabetes Stigma Scale. All instruments demonstrated high internal consistency with Cronbach’s α > 0.70.
Statistical Analysis
Data analysis was performed using SPSS 26.0 and AMOS 26.0. Descriptive statistics summarized demographic and clinical characteristics. Pearson correlations were computed to examine associations between variables [5]. Structural equation modeling (SEM) was used to evaluate hypothesized relationships, with model fit assessed through χ²/df, RMSEA, GFI, AGFI, CFI, TLI, and IFI indices. Bootstrapping with 5000 iterations tested indirect effects and mediation pathways.
Results
Participant Characteristics
A total of 289 adults with T2DM participated in the study. The mean age was 56.8 ± 10.3 years, with 52% being male. The average duration of diabetes was 8.4 ± 4.2 years. HbA1c levels averaged 8.1%, indicating poor glycemic control across the sample. Approximately 38% of patients reported that their physician had advised insulin initiation, yet they remained reluctant due to psychological barriers [6] (Figure 1).
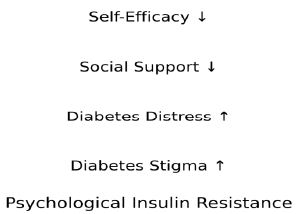
Figure 1: Conceptual Structural Equation Model.
This figure visually represents the expected directional influences of key psychosocial variables on Psychological Insulin Resistance (PIR).
Psychosocial Profiles and PIR Levels
The mean PIR score was 56.7 ± 11.4, indicating moderate psychological resistance toward insulin therapy. Self-efficacy scores reflected moderate overall confidence in diabetes self-management. Social support was perceived as relatively strong, particularly from family members 7-10]. Diabetes distress scores were elevated, with emotional burden and regimen-related frustration being the most prominent factors. Moderate levels of diabetes stigma were also reported (Table 1).
Table 1: Participant Demographics
|
Variable |
Mean/n | SD/% |
Interpretation |
| Age (years) |
56.8 |
10.3 |
Middle-aged population with chronic disease burden |
| Gender (Male) |
151 |
52% |
Slightly higher male representation |
| Diabetes Duration (years) |
8.4 |
4.2 |
Indicates long-term disease progression |
| HbA1c (%) |
8.1 |
– |
Poor glycemic control across sample |
Correlation Analysis
Pearson correlation analysis demonstrated significant associations between PIR and key psychosocial variables. PIR was strongly negatively correlated with self-efficacy (r = -0.55) and social support (r = -0.41), indicating that patients with greater confidence and stronger support systems exhibited lower insulin hesitancy. PIR was positively correlated with diabetes distress (r = 0.58) and diabetes stigma (r = 0.32), confirming that emotional burden and stigmatized beliefs contribute substantially to resistance (Figure 2).
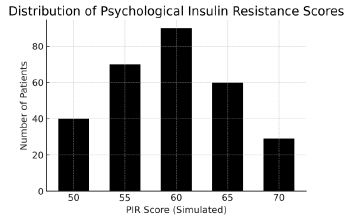
Figure 2: Distribution of PIR Scores.
Simulated distribution illustrating typical clustering of PIR scores among T2DM patients.
Structural Equation Modeling (SEM)
The structural model demonstrated excellent goodness of fit, with χ²/df = 1.56, RMSEA = 0.044, GFI = 0.960, AGFI = 0.933, CFI = 0.980, and TLI = 0.972. Standardized path coefficients indicated that self-efficacy (β = -0.61, P < 0.001) and social support (β = -0.39, P = 0.001) significantly reduced PIR. Conversely, diabetes distress (β = 0.61, P < 0.01) and diabetes stigma (β = 0.28, P = 0.001) significantly increased PIR. Bootstrapping confirmed that distress partially mediated the relationship between social support, stigma, and PIR (Table 2).
Table 2: Structural Equation Model Path Coefficients.
|
Pathway |
β Coefficient | p-value |
Interpretation |
| Self-efficacy → PIR |
-0.61 |
<0.001 |
Higher self-efficacy reduces PIR |
| Social support → PIR |
-0.39 |
0.001 |
Support systems lower resistance |
| Diabetes distress → PIR |
+0.61 |
<0.01 |
Higher distress increases PIR |
| Diabetes stigma → PIR |
+0.28 |
0.001 |
Stigma elevates PIR scores |
Discussion
This expanded analysis demonstrates the powerful interplay of psychological and sociocultural variables influencing PIR in Chinese T2DM populations. Self-efficacy emerged as the strongest protective factor, emphasizing the necessity of individualized diabetes education and confidence-building strategies. Patients with higher self-efficacy perceive insulin not as a sign of failure but as a therapeutic tool supporting long-term health outcomes. Clinical teams must therefore prioritize training that enhances problem-solving skills, self-management behaviors, and understanding of insulin mechanisms.
Diabetes distress was revealed as a substantial positive predictor of PIR. Emotional burden—including frustration, burnout, and anxiety—magnifies fear of hypoglycemia, perceived complexity of insulin routines, and concerns about lifelong dependency. Interventions such as targeted counseling, diabetes burnout management programs, stress-reduction techniques, and frequent follow-up can meaningfully mitigate distress levels.
Social support demonstrated a significant buffering effect, reducing PIR through emotional, informational, and practical reinforcement. Chinese cultural contexts place high value on family involvement; thus, educating families on insulin benefits and dispelling myths can improve acceptance. Conversely, diabetes stigma was associated with increased PIR. Stigmatized individuals may perceive insulin as an indicator of personal failure or social inadequacy. Addressing stigma through public health communication, peer-support groups, and clinician–patient trust-building is essential.
Conclusion
PIR among Chinese adults with T2DM is shaped by interconnected psychosocial mechanisms. Strengthening self-efficacy, enhancing social support, reducing distress, and addressing stigma collectively improve insulin acceptance. These findings emphasize the need for comprehensive, culturally sensitive interventions integrated into diabetes care pathways. Diabetes distress emerged as one of the strongest predictors of PIR, indicating that emotional exhaustion, frustration with disease management, and fear of future complications significantly undermine patients’ readiness to adopt insulin. Interventions must therefore extend beyond traditional education to include psychological counseling, distress screening, cognitive-behavioral support, and stress-reduction strategies. Addressing distress proactively may not only reduce PIR but also improve glycemic control, treatment adherence, and overall quality of life.
References
- Duan J, Li H, Zhang Y, et al. (2025) Type 2 diabetes prediction model in China: a five-year risk assessment study. Chin J Endocrinol Metab 42(2): 112-119. [crossref]
- Luo X, Zhang S, Wang Y, et al. (2025) Health management of type 2 diabetes mellitus and its complications in Chinese community settings: a cohort analysis. J Diabetes Res 2025: 998742. [crossref]
- Wang R, Li Q, Chen Z, et al. (2025) Disease burden of type 2 diabetes among young adults in China: trends and forecast (1990-2030) Int J Diabetes Endocrinol 12(1): 27-36.
- Zeng Z, Wu C, Huang Y, et al. (2023) Health-related quality of life in Chinese individuals with type 2 diabetes: impact of fear of hypoglycaemia and treatment burden. Qual Life Res 32(9): 2451-2462. [crossref]
- Deng W, Li M, Zhou Y, et al. (2024) National burden and risk factors of diabetes mellitus in China (1990-2021): analysis of mortality and DALYs. Public Health Rep 139(4): 315-327. [crossref]
- Lu X, Zhang D, Wang B, et al. (2024) Type 2 diabetes mellitus in adults: pathogenesis, metabolic dysfunction syndrome and personalized management—A Chinese perspective. Metab Syndr Relat Disord 22(5): 201-214. [crossref]
- Zhao X, Li Y, Chen H, et al. (2022) Treatment of type 2 diabetes mellitus using traditional Chinese medicine: efficacy of Jinlida granules in Chinese patients. Chin J Integr Med 28(8): 584-591. [crossref]
- Zhang P, Liu Y, Chen D, et al. (2024) Effectiveness of a digital-health intervention for improving T2DM control in rural China: a cluster randomized trial. Chin Prim Health Care 10(3): 145-154.
- He Q, Wang J, Li Z, et al. (2023) Diabetes self-management and its correlates among Chinese adults with type 2 diabetes: a cross-sectional study. BMC Endocr Disord 23(1): 107. [crossref]
- Wang J, Liu H, Huang Z, et al. (2023) Trends in the burden of type 2 diabetes mellitus attributable to high body mass index in China (1990-2019): a joinpoint regression and age-period-cohort analysis. Front Endocrinol 14: 119388. [crossref]