Abstract
Reliable fetal weight assessment is a crucial part of predicting delivery risks and planning suitable obstetric interventions. The chosen estimation method can impact clinical decisions, especially when access to advanced diagnostic tools is limited. This study compared the predictive accuracy of two clinical formulas, Johnson’s method and Dare’s formula, with ultrasonography in estimating fetal weight at term, using actual birth weight as the benchmark. In a prospective cohort of 200 women with term singleton cephalic pregnancies, fetal weight was estimated via Johnson’s method, Dare’s formula, and ultrasonography (Hadlock’s formula). Actual birth weights were recorded after delivery. For each method, mean differences, mean errors, standard deviations, and Pearson correlation coefficients were calculated against actual birth weight. Johnson’s method estimated an average fetal weight of 2914.08g compared to the actual mean of 3115.4g, with a mean error of 250.25g and a strong correlation (r = 0.7640), indicating underestimation. Dare’s Formula estimated a mean weight of 3147.01g versus an actual mean of 2898.1g, with a mean error of 298.15g and r = 0.745, indicating overestimation. Ultrasonography showed the highest accuracy, with an average estimated weight of 3015.5g against an actual mean of 2974.1g, a mean error of 202.5g, and a very strong correlation (r = 0.877). Ultrasonography was the most precise method for fetal weight estimation, displaying minimal bias and the strongest correlation with actual birth weight. Of the clinical methods, Johnson’s method performed better than Dare’s formula, making it a viable option when ultrasonography is unavailable, although its tendency to underestimate should be considered in clinical decision-making.
Keywords
Fetal weight estimation, Johnson’s method, Dare’s formula, Ultrasonography, Hadlock’s formula, Birth weight, Obstetric assessment, Term pregnancy
Introduction
Precise estimation of fetal biometry in late pregnancy is a cornerstone of modern obstetric practice, guiding critical decisions regarding the timing, mode, and place of delivery. The ability to reliably predict fetal weight enables clinicians to anticipate and prevent complications such as shoulder dystocia in macrosomic fetuses, identify and manage intrauterine growth restriction (IUGR), and reduce adverse maternal and neonatal outcomes. Over time, a number of clinical and sonographic methods have been developed for this purpose. Nonetheless, no distinct or singular methodology has attained widespread recognition as a gold standard [1-3]. Clinical methodologies for predicting fetal weights, including Johnson’s and Dare’s formulas, are predicated on straightforward anthropometric measurements, chiefly “symphysio-fundal height (SFH)” and “abdominal girth (AG)’’. R.W. Johnson was the first to write about the Johnson’s formula. He utilized the SFH and changed it for fetal station to come up with an estimated fetal weight. Dare’s formula, on the other hand, employs the product of SFH and AG to find the weight in grams [4-6]. These treatments are cheap, don’t need much equipment, and can be done at any level of healthcare, which makes them especially valuable in places with few resources [7,8]. But their accuracy might be affected by things including the mother’s weight, the amount of amniotic fluid, problems with the uterus, the location of the fetus, and the examiner’s experience [6,9]. Studies have reported a tendency for some formulas to systematically overestimate or underestimate fetal weight, which can affect clinical decision-making methodologies [9-11].
Ultrasonography (USG) has gained widespread acceptance due to its ability to incorporate multiple biometric parameters, including bi-parietal diameter, abdominal circumference, femur length, and head circumference into regression equations such as Hadlock’s formula [12-15]. It is generally perceived as a more objective and reproducible technique as compared to clinical palpation, with reported advantages in cases of abnormal fetal growth, altered maternal nutrition, and high body mass index [16,17]. However, ultrasonographic accuracy can still be influenced by operator skill, fetal position, placental location, and extreme fetal size [18]. Additionally, the lack of functional ultrasound equipment and trained personnel in many primary healthcare facilities, especially in developing countries, remains a significant barrier to its universal use [19,20]. Comparative studies between clinical methods and ultrasonography have produced mixed results. Some studies find ultrasonography to be superior, particularly at the extremes of birth weight [21,22], while others show comparable performance between the two methods, especially for fetuses within the normal birth weight range of 2500-4000g. Clinical palpation tends to be less accurate for estimating weights below 2500g, though ultrasonography may provide better accuracy in such cases [23]. Given these differences, evaluating the most appropriate method based on specific context is crucial for different healthcare environments.
Recognizing the clinical importance of precise fetal weight estimation and the variability in reported accuracies, the present study was undertaken to systematically evaluate and compare the performance of Johnson’s method, Dare’s formula, and ultrasonography in predicting actual birth weight in term pregnancies. By assessing name differences, estimation errors, and correlation coefficients, the study aimed to identify the method that most closely approximates actual birth weight, thereby providing a reliable basis for obstetric decision-making. Importantly, the comparison extends beyond determining statistical accuracy; it also considers the clinical applicability of each method within different healthcare contexts. In resource-rich settings, ultrasonography may be readily available and preferred; however, in many rural or rural resource environments, access to functional ultrasound equipment and trained personnel is often limited [23,24]. In such scenarios, cost-effective and easily implementable clinical formulas retain significant value provided their limitations are understood and accounted for. By directly comparing these three approaches in a uniform cohort under the same clinical conditions, this study seeks to generate evidence that can guide practitioners in selecting the most appropriate method for fetal weight estimation according to their resource availability and clinical setting. The findings are expected to contribute to more informed clinical judgment, better delivery planning, and ultimately improved maternal and neonatal outcomes [25,26].
Materials and Methods
The randomized clinical study was conducted at the District Hospital, Krishnanagar, Nadia, as an institution-based investigation. It was designed as a prospective cohort study involving pregnant women who met the specific inclusion criteria. All eligible participants were recruited from the hospital’s Obstetrics and Gynaecology Department, and the study was carried out within the institutional setting to ensure uniformity of procedures and consistency in data collection. The study was performed after clearance from the Board of Studies and the Ethical Committee in the Department of Obstetrics and Gynaecology, Nadia District Hospital.
Inclusion Criteria
- The study included pregnant women with a singleton pregnancy.
- The pregnancy should be of cephalic presentation.
- The pregnant woman should carry a live fetus.
- The participants were required to have a known last menstrual period (LMP) or a prior ultrasound scan confirming the expected date of delivery.
- Only those with a gestational age between 37 and 42 weeks at the time of assessment were eligible.
Exclusion Criteria
- Women were excluded from the study if they were carrying an anomalous fetus.
- Pregnant women with the presence of coexisting uterine or adnexal pathologies such as fibroids or ovarian cysts.
- Pregnant women who have been previously diagnosed with liquor abnormalities.
Sample Size Estimation
The required sample size for the study was determined using the formula for estimating a population mean within a specified precision at a 95% confidence interval:
![]()
where,
Zα/2 = 1.96 (standard normal variate at 95% confidence)
σ = 8 (assumed standard deviation)
E = 1.5 (allowed error).
Substituting these values gave:
![]()
n=109.3
Thus, a minimum of 110 participants was required. To enhance the reliability of the results and account for potential dropouts, the sample size was increased to 200 term singleton pregnancies meeting the inclusion criteria.
Study Procedure
After getting the go-ahead from the Institutional Ethical Committee, all patients were chosen based on the rules for who could and couldn’t be included. All patients underwent a detailed medical history, full physical examination, and appropriate standard and specific investigations. The study involved pregnant women who satisfied the inclusion and exclusion criteria at the Obstetrics and Gynecology Department of the District Hospital in Krishnanagar, Nadia. The study involved 200 women. A thorough history will be acquired, including the patient’s education, occupation, socio-economic position, menstrual history, obstetric history, previous medical and surgical history, and personal history. A thorough general physical exam will be done. All systems and vital signs will be checked. A general physical examination was performed, succeeded by an abdominal assessment in the supine posture. Patients were told to empty their bladders before the inspection. After correcting the uterus’s dextro-rotation, the height of the uterus is measured by feeling from the xiphisternum down. To measure the symphysio-fundal height (in cm), a flexible standard measuring tape is used to touch the skin while pointing it toward the patient. The upper boundary of the pubic symphysis is felt. Next, the abdominal circumference (in cm) is measured at the level of the umbilicus in the same way. Johnson’s and Dare’s formula is used to figure out the expected weight of the fetus. The patient will have an ultrasound test to check the baby’s weight because there wasn’t one last week. Fetal biometry was evaluated using many parameters, including body weight, biparietal diameter, head circumference, abdominal circumference, and femoral length..
Formulas Used for Calculations
Johnson’s Formula
FW = (SFH – y) x 155
where,
FW: Fetal weight (in g)
SFH: Symphysio Fundal Height (in cm)
y = 13 when the head is not engaged
y = 12 when the head is at the “0” station
y = 11 when the head is at the +1 station
The fundal height is reduced by 1 cm if the mother’s weight is >91 kg.
Dare’s Formula
EFW = SFH x AG
where,
EFW: Estimated Fetal Weight (in g)
SFH: Symphysio Fundal Height (in cm)
AG: Abdominal Girth (in cm)
Hadlock’s Formula
log10 BW = 0.3596 + (0.00061 x BPD x AC) + (0.042 x AC) + (0.174 x FL) + (0.0064 x HC) – (0.00386 x AC x FL)
where,
BW: Body weight (in g)
BPD: Bi-parietal diameter (in mm)
AC: Abdominal circumference (in cm)
FL: Femoral length (in mm)
HC: Head circumference (in cm)
Statistical Evaluation
The statistical analysis was conducted using SPSS version 25.0 after importing data into a Microsoft Excel spreadsheet. The quantitative data was expressed as the mean and standard deviation, whilst the qualitative data was represented as the frequency and proportion of each group. The Student’s t-test was employed to compare the mean values of the two groups, while the Chi-square test was used to evaluate the frequency differences between them. A p-value less than 0.05 is considered statistically significant.
Results and Discussion
The study evaluated the precision of fetal weight estimation utilizing Johnson’s approach against actual birth weights. The average actual birth weight was 3115.4g, while the average estimated fetal weight calculated using Johnson’s approach was 2914.08g. (Table 1 and Figure 1). The mean difference of 87.14g indicated a tendency of Johnson’s method to underestimate fetal weight. The mean estimation error was 250.25g, corresponding to approximately 84g/kg of actual weight. The standard deviation of the estimations was 421.15g, and the standard error of the mean was 41.15g. The Pearson product-moment correlation coefficient between actual and estimated weight was 0.764, denoting a strong positive correlation and suggesting that, despite its tendency to underestimate, Johnson’s method demonstrates a reasonable degree of accuracy in predicting fetal weight.
Table 1: Comparison of the mean actual birth weight with the mean estimated birth weight by Johnson’s method.
|
Sr. No. |
Parameters |
Estimations |
|
1. |
Mean actual birth weight | 3115.4 g |
|
2. |
Mean estimated fetal weight | 2914.08 g |
| 3. | Difference between the mean actual birth weight and the mean estimated fetal weight |
87.14 g |
|
4. |
Mean error of estimation |
250.25 g (∼84 g/kg) |
|
5. |
Standard deviation (SD) |
421.15 g |
|
6. |
Standard error of the mean (SE) |
41.15 g |
|
7. |
Person product-moment correlation coefficient |
0.764 |
| 8. | p-value |
0.001 |
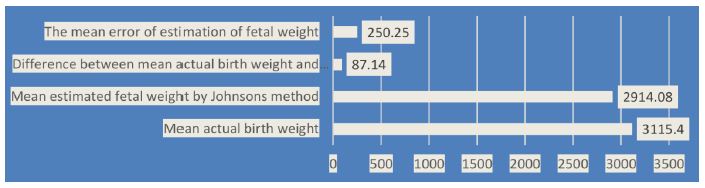
Figure 1: Comparison of the mean actual birth weight with the mean estimated birth weight by Johnson’s method.
The study assessed the accuracy of fetal weight estimation using Dare’s Formula in comparison with actual birth weights. The mean actual birth weight was 2898.1g, whereas the mean EFW obtained using Dare’s Formula was 3147.01g (Table 2 and Figure 2). The mean difference of 146.8g indicated a tendency for Dare’s Formula to overestimate fetal weight. The mean estimation error was 298.15g, corresponding to approximately 93g/kg of actual weight. The standard deviation of the estimations was 415.18g, and the standard error of the mean was 41.74g. The Pearson product-moment correlation coefficient between actual and estimated weight was 0.745, indicating a strong positive correlation. Despite its tendency to overestimate, Dare’s Formula demonstrated a reasonable degree of accuracy in predicting fetal weight.
Table 2: Comparison of the mean actual birth weight with the mean estimated birth weight by Dare’s formula.
|
Sr. No. |
Parameters |
Estimations |
| 1. | Mean actual birth weight | 2898.1 g |
| 2. | Mean estimated fetal weight | 3147.01 g |
| 3. | Difference between the mean actual birth weight and the mean estimated fetal weight | 146.8 g |
| 4 | Mean error of estimation | 298.15 g (~93 g/kg) |
| 5. | Standard deviation (SD) | 415.18 g |
| 6. | Standard error of the mean (SE) | 41.74 g |
| 7. | Person product-moment correlation coefficient | 0.745 |
| 8. | p-value | 0.001 |
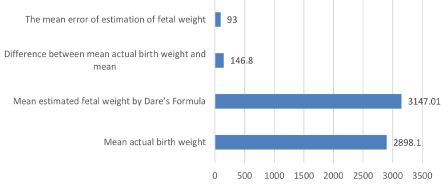
Figure 2: Comparison of the mean actual birth weight with the mean estimated birth weight by Dare’s formula.
The study evaluated the accuracy of fetal weight estimation using ultrasonography (USG) compared to actual birth weights. The mean actual birth weight was 2874.5g, while the mean EFW by USG was 2817.4g. The difference between these means was 12.95g, indicating that USG provided a very close estimation of fetal weight. The mean error of estimation was 46.95g/kg of actual weight (Table 3 and Figure 3). The standard deviation (SD) of the estimations was 475.75g, and the standard error of the mean (SE) was 47.57g. The Pearson product-moment correlation coefficient between actual and estimated weights was 0.911, suggesting a very strong positive correlation. These findings demonstrated that ultrasonography was highly accurate in predicting fetal weight, with minimal error and high correlation with actual birth weights.
The study compared the accuracy of fetal weight estimations by ultrasonography (USG), Johnson’s method, and Dare’s formula with actual birth weights (Table 4 and Figure 4). Within the ±50g range, 14% of cases were accurately estimated by USG, 7.5% by Johnson’s method, and 6% by Dare’s formula. In the ±100g range, USG accurately estimated 28% of cases, Johnson’s method 12%, and Dare’s formula 12.5%. For the ±150g range, USG had 34.5% accuracy, Johnson’s method 18%, and Dare’s formula 15%. In the ±200g range, USG accurately estimated 45% of cases, Johnson’s method 34.5%, and Dare’s formula 27.5%. Within the ±250g range, USG had 57% accuracy, Johnson’s method 49%, and Dare’s formula 43.5%. For the ±300g range, USG accurately estimated 79.5% of cases, Johnson’s method 57%, and Dare’s formula 50%. Within the ±500g range, USG had 100% accuracy, Johnson’s method 72.5%, and Dare’s formula 65%. For the ±1000g range, Johnson’s method accurately estimated 100% of cases, and Dare’s formula 82%, while USG did not have data for this range. For estimations beyond ±1000 grams, only Dare’s formula had data, accurately estimating 100% of cases. These findings highlighted that USG consistently provided the highest accuracy across most ranges, followed by Johnson’s method and Dare’s formula, with Dare’s formula showing the highest accuracy in the widest ranges beyond ±500g.
Table 3: Comparison of the mean actual birth weight with the mean estimated birth weight using USG.
|
Sr. No. |
Parameters |
Estimations |
| 1. | Mean actual birth weight | 2874.5 g |
| 2. | Mean estimated fetal weight | 2817.4 g |
| 3. | Difference between the mean actual birth weight and the mean estimated fetal weight | 12.95 g |
| 4 | Mean error of estimation | 46.95 g/kg |
| 5. | Standard deviation (SD) | 475.75 g |
| 6. | Standard error of the mean (SE) | 47.57 g |
| 7. | Person product-moment correlation coefficient | 0.911 |
| 8. | p-value | 0.001 |
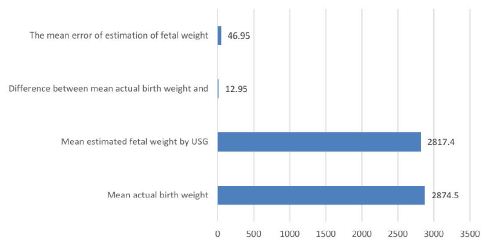
Figure 3: Comparison of the mean actual birth weight with the mean estimated birth weight by USG.
Table 4: Comparison of the clinical method with USG, Johnson’s, and Dare’s methods with actual birth weight.
|
Range |
USG (%) | Johnson’s Method (%) | Dare’s Formula (%) |
| ±50 g | 14 | 7.5 |
6 |
|
±100 g |
28 | 12 | 12.5 |
| ±150 g | 34.5 | 18 |
15 |
|
±200 g |
45 | 34.5 | 27.5 |
| ±250 g | 57 | 49 |
43.5 |
|
±300 g |
79.5 | 57 | 50 |
| ±500 g | 100 | 72.5 |
65 |
|
±1000 g |
– | 100 | 82 |
| >±1000 g | – | – |
100 |
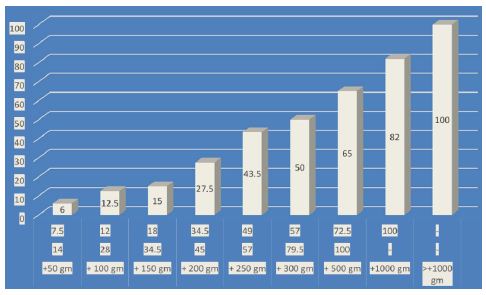
Figure 4: Comparison of clinical method and USG with actual birth weight.
The study compared the actual birth weights of babies to the fetal weight estimates made using Johnson’s method, Dare’s formula, and ultrasonography (USG). Johnson’s approach often gave a lower estimate of fetal weight. Lazer et al. (1986) discovered that Johnson’s approach often underestimates, particularly in larger fetuses, which affects preparation for delivery. Ouzounian et al. (1998) assert that mistakes in clinical estimating methodologies may result in unsatisfactory delivery decisions. The underestimations underscore the necessity for modifications or additional methodologies to improve accuracy in clinical environments. Because there is so much variation, a combination approach incorporating both clinical and ultrasound data is needed to get a more accurate estimate of the baby’s weight. Dare’s formula often gave too high of an estimate, which meant that it needed to be recalibrated or adjusted for certain situations to prevent making mistakes in the clinic. The USG gave the most precise estimates with very little inaccuracy and a strong link to actual birth weights. Boyd et al. (1983) commend the precision of ultrasonography in prenatal care. Berard et al. (1998) further support the dependability of ultrasonography in different maternal and fetal situations. The established accuracy reinforces ultrasonography as a fundamental component in prenatal diagnosis and delivery decision-making. Moreover, variability in accuracy, with ultrasonography generally being more reliable.When comparing clinical methods, where the ultrasonography (USG) consistently outperformed both Johnson’s method and Dare’s formula in terms of mean estimation error, correlation with actual birth weight, and minimization of bias. Ouzounian et al. (1998) discuss ultrasonography’s higher reliability over clinical methods in accurate weight estimation. Irion and Boulvain (2000) highlight the challenge of estimating weight in larger fetuses, with clinical methods often showing greater discrepancies. The systematic biases highlight the importance of method selection based on the clinical context. In settings where ultrasonography is unavailable, Johnson’s method may be preferred due to its similar mean bias while acknowledging its limitations. These insights underscore the superiority of ultrasound in fetal weight estimation and the need for its combination with clinical assessments, especially in cases of expected larger fetuses.
The results of this study underscore the trade-offs between clinical palpation-based formulas and ultrasonography. Ultrasonography offers the highest accuracy and should be preferred where accessible clinical methods retain relevance in resource-limited environments. Future research should focus on refining clinical estimation formulas, incorporating maternal and fetal parameters, to bridge the accuracy gap with ultrasonography. Additionally, combining clinical methods with portable low-cost ultrasound devices could enhance accuracy in peripheral healthcare settings.
Conclusion
This study evaluated the precision of fetal weight estimation employing three clinical techniques: Johnson’s method, Dare’s formula, and ultrasonography. The initial two techniques were evaluated using ultrasonography (Hadlock’s formula) in comparison to actual birth weight. The data indicated that although all three approaches had a statistically significant positive connection with actual birth weights, their performance differed in terms of accuracy, bias, and reliability. Ultrasonography emerged as the most accurate technique, with the least mean variation from actual birth weight, the lowest mean estimation error, and the highest correlation coefficient.. Because it can make estimates with little bias, it is the best way to estimate fetal weight in well-equipped healthcare systems, especially where accuracy is important for making decisions about obstetrics. Johnson’s technique tended to underestimate fetal weight, while Dare’s formula tended to overestimate it. Johnson’s technique had a slightly better association with actual birth weight than Dare’s formula. This suggests that it might be more accurate when an ultrasound isn’t available. Nonetheless, both clinical procedures demonstrated elevated estimating errors and increased variability compared to ultrasonography. These results show that even while ultrasound is currently the best way to estimate baby weight, clinical approaches are still useful in low-resource or rural areas where ultrasound is not easily available. In some cases, Johnson’s method might be better than Dare’s formula since it has a reduced mean bias, even though it tends to underestimate. However, professionals need to keep these limits in mind when looking at outcomes so that they don’t make mistakes during obstetric procedures. The selection of a method for estimating heat and weight should be determined by the resources at hand, the clinical situation, and the necessity for precision. Improving healthcare workers’ expertise in clinical estimating procedures and making portable, affordable ultrasound technology more available could work together to improve outcomes for mothers and babies, especially in places where resources are limited.
References
- Yomibo-Sofolahan TA, Ariba AJ, Abiodun O, Egunjobi AO, Ojo OS (2021) Reliability of a clinical method in estimating foetal weight and predicting route of delivery in term parturient monitored at a voluntary agency hospital in Southwest Nigeria. Afr J Prim Health Care Fam Med 13(1): e1-e6. [crossref]
- Dare FO, Ademowore AS, Ifaturoti OO, Nganwuchu A (1990) The value of symphysio-fundal height/abdominal girth measurements in predicting fetal weight. Int J Gynaecol Obstet; 31 (3): 243-8. [crossref]
- Whitworth M, Bricker L, Mullan C (2015) Ultrasound for fetal assessment in early pregnancy. Cochrane Database Syst Rev 2015(7): CD007058. [crossref]
- Shittu AS, Kuti O, Orji EO, Makinde NO, Ogunniy SO, et al. (2007) Clinical versus sonographic estimation of foetal weight in southwest Nigeria. J Health Popul Nutr 25(1): 14-23. [crossref]
- Lanowski JS, Lanowski G, Schippert C, Drinkut K, Hillemanns P, et al. (2017) Ultrasound versus Clinical Examination to Estimate Fetal Weight at Term. Geburtshilfe Frauenheilkd; 77(3): 276-283. [crossref]
- Lanowski JS, Lanowski G, Schippert C, Drinkut K, Hillemanns P and Staboulidou I (2017) Ultrasound versus Clinical Examination to Estimate Fetal Weight at Term. Geburtshilfe Frauenheilkd 77(3): 276-283. [crossref]
- Ingale A, Khade SA and Shirodkar S (2019) Clinical versus ultrasonographic fetal weight estimation and its correlation with actual birth weight. Int J Contracept Obstet Gynecol; 8(2): 503-512.
- Roy AG, Kathaley MH (2018) Comparison of Estimation of fetal weight by clinical method, ultrasonography and its correlation with actual birth weight in term pregnancy. MVP Journal of Medical Sciences; Vol 5(1): 75-81.
- Shittu AS, Kuti O, Orji EO, Makinde NO, Ogunniy SO, et al. (2007) Clinical versus sonographic estimation of foetal weight in southwest Nigeria. J Health Popul Nutr 25(1): 14-23. [crossref]
- Torloni MR, Sass N, Sato JL, Renzi AC, Fukuyama M, et al. (2008) Clinical formulas, mother’s opinion and ultrasound in predicting birth weight. Sao Paulo Med J 126(3): 145-9. [crossref]
- Belete W, Gaym A (2008) Clinical estimation of fetal weight in low resource settings: comparison of Johnson’s formula and the palpation method. Ethiop Med J 46(1): 37-46. [crossref]
- Malik R, Thakur P, Agarwal G (2016) Comparison of three clinical and three ultrasonic equations in predicting fetal birth weight. International Journal of Reproduction, Contraception, Obstetrics and Gynecology; 5(1): 210-6.
- Bajaj P, Kadikar GK, Kannani M, Bhatt M, Shah S (2017) Estimation of foetal birth weight clinically and sonographically and its correlation with its actual birth weight: A prospective and comparative study. International Journal of Reproduction, Contraception, Obstetrics and Gynecology; 6(7): 3103-8.
- Weiner E, Mizrachi Y, Fainstein N, Elyashiv O, Mevorach-Zussman N, Bar J, et al. (2017) Comparison between three methods of fetal weight estimation during the active stage of labor performed by residents: A prospective cohort study. Fetal Diagnosis and Therapy; 42(2): 117-23. [crossref]
- Hiwale S, Misra H, Ulman S (2019) Fetal weight estimation by ultrasound: development of Indian population-based models. Ultrasonography; 38(1): 50-57.
- Johnson RW, Toshach CE. Estimation of fetal weight using longitudinal measurementation. American journal of obstet and gynaecol 1954: 68(3)891-6. [crossref]
- Sharma R, Singh S, Bhartyia V, Gupta J, Radhakrishnan G (2015) Product of Symphysio-Fundal Height and Abdominal Circumference: A Predictor of Estimated Fetal Weight at Birth. Int J Sci Stud; 3(9): 125-127.
- Hadlock FP, Deter RL, Harrist RB, Park SK(1982) Fetal biparietal diameter: rational choice of plane of section for sonographic measurement. AJR Am J Roentgenol; 138(5): 871-874. [crossref]
- Hadlock FP, Kent WR, Loyd JL (1982) An evaluation of two methods for measuring fetal head and body circumferences. J Ultrasound Med; 1(9): 359-60. [crossref]
- Goldstein RB, Filly RA, Simpson G (1987) Pitfalls in femur length measurements. J Ultrasound Med 1987; 6(4): 203-7. [crossref]
- Kathiriya D, Patil Y, Patange RP (2014) Comparative Study of Various Methods of Fetal Weight Estimation at Term Pregnancy. Inter J Recent Trends in Sci Tech; 9(3): 453-6.
- Sowjanya R, Lavanya S (2015) Comparative Study of Clinical Assessment of Fetal Weight Estimation Using Johnson’s Formula and Ultrasonographic Assessment Using Hadlock’s Formula At or Near Term. J Dent Med Sci; 14(4): 20-3.
- Dongol A, Bastakoti R, Pradhan N, Sharma N (2020) Clinical estimation of fetal weight with reference to Johnson’s formula: An alternative solution adjacent to sonographic estimation of fetal weight. Kathmandu University Medical Journal; 18(70): 111-116. [crossref]
- Lertrat W, Kitiyodom S (2021) Accuracy of intrapartum fetal weight estimation using dare’s formula and transabdominal ultrasonography in pregnant women with normal and high prepregnant BMI at Maharat Nakhon Ratchasima Hospital. Thai Journal of Obstetrics and Gynaecology 29: 313 21.
- Pavithra K, Priyadarshini K, Annapoorna Y (2022) Estimation of fetal weight by clinical method and its comparison with ultrasonography and its correlation with actual birth weight in term singleton pregnancy. Indian J Obstet Gynecol Res 9(3): 347-351.
- Gurung SD, Shrestha J, Gauchan E, Subedi A, Shrestha A, Thapa S (2022) Comparison of Actual Birth Weight with the Ultrasonographic and Clinical Estimation of Fetal Birth Weight: A Prospective Study. Nepalese Journal of Radiology 12(1): 8-12.